
Abstract
Objective:
To investigate if peritumor and/or intratumor vasculature is associated with high-grade tumor histology for renal cell carcinoma.
Methods:
A retrospective review at a tertiary care facility was performed of patients who underwent radical nephrectomy or partial nephrectomy for a renal tumor between January 2015 and December 2020. Data of tumor characteristics were collected from final pathology reports. A single radiologist specializing in genitourinary imaging reviewed all preoperative cross-sectional imaging for peritumor vessels and intratumor vessels. Single and multivariable logistic regression was utilized to identify variables associated with high-grade tumor histology.
Results:
The average tumor size on final pathology report was 6.4 cm (range 3.0–17.0 cm). Ninety-two patients (56.1%) had either an enlarged peritumor vessel (n = 72), an intratumor vessel (n = 3), or both a peritumor vessel and an intratumor vessel (n = 17). Of the 92 patients with either a peritumor vessel or both a peritumor vessel and intratumor vessel, 60.9% of these patients had high Fuhrman grade histology on final pathology report (60.9% vs 39.1%, p < 0.001). Pathologic stage T1a tumors with an enlarged peritumor vessel on preoperative imaging were associated with high Fuhrman grade histology (58.3% vs 41.7%, p = 0.015). Across all stages, the presence of an enlarged peritumor vessel was significantly associated with high Fuhrman grade (odds ratio: 2.37, 95% confidence interval 1.17–4.9, p = 0.01).
Conclusion:
Findings suggest that vessels surrounding small renal tumors and large renal tumors is associated with high tumor grade (Fuhrman grade >3). Further research is needed to support the association of peritumor vessels with high tumor grade.
Introduction
The incidental finding of renal masses has risen with an increase in the utilization of imaging. 1 –3 Although most solid contrast-enhancing masses in the kidney are malignant, the management of enhancing solid renal tumors suspicious for malignancy can vary based on tumor characteristics and patient factors.
Kidney cancer and renal pelvic tumors make up 4.0% of all new cancer cases. 4 The detection rates have been stable from 2008 to 2017 with age-adjusted death rates falling 1.4% each year from 2009 to 2018. 4 This is all despite an increase in the utilization of active surveillance (AS) for small renal tumors. 5,6 Identifying preoperative factors to assist with predicting tumor pathology analysis and thus potential behavior is critical in management decision-making.
CT and MRI have improved over the decades as well. Traditionally, common criteria used to assess the aggressiveness of disease include simple factors such as renal mass size, the status of vein involvement, lymph node assessment, and metastatic work-up. 7 There may be additional information that can help risk-stratify patients. Such additional data may better stratify patients for AS vs treatment or partial nephrectomy vs radical nephrectomy for those masses that leave the clinician “on the fence” as to the best management choice.
We hypothesized that those renal cancers that are biologically capable of developing and recruiting angiogenesis may be more aggressive tumors. We further hypothesize that there may be information in cross-sectional imaging that can capture tumors that have more vascularity associated with them as a possible surrogate marker for aggressiveness. In this regard, there are some findings on preoperative imaging that may have been historically overlooked. Specifically, peritumor vasculature and its link to aggressive tumor pathology analysis have only been described once. 8
We hypothesize that peritumor vasculature on preoperative imaging is associated with a high Fuhrman grade on final pathology report.
Methods
Institutional review board approval was obtained to retrospectively review patients who have undergone radical nephrectomy or partial nephrectomy for a renal tumor between January 2015 and December 2020. Patients included in the study were adult patients (≥18 years) with a solitary solid renal tumor and no past medical history of predisposing conditions to renal cell carcinoma (RCC). Tumor characteristics on final pathology report that were reviewed included subtype of RCC, tumor size, grade of tumor, presence of renal sinus or perirenal fat invasion, and presence of positive lymph nodes.
Patients who met inclusion criteria based on tumor characteristics were those who had malignant tumors on final pathology report, comprising a variety of RCC subtypes that were ≥3.0 cm. Subtypes of RCC included in the analysis were clear cell, papillary type I, papillary type II, chromophobe, RCC with sarcomatoid features, RCC with rhabdoid features, and clear cell papillary RCC. Benign renal tumors and renal cystic tumors were excluded from this analysis Patients with a previous history of tumor resection were excluded. Finally, patients with lymphadenopathy and/or presence of distant metastatic disease on final tumor pathology analysis were excluded.
Patient characteristics retrospectively reviewed included basic demographics, such as age, gender, body mass index (BMI), and race. Past medical history data included hypertension, diabetes mellitus, hyperlipidemia, end-stage renal disease, and family history of RCC. After identifying patients who met our initial inclusion criteria, preoperative imaging for each patient was retrospectively reviewed by a single genitourinary radiologist (GI) who was blinded to the pathologic characteristics of the cancers. All patients included in the study had either CT or MRI preoperative imaging available to review.
Technique for evaluating contrast-enhanced CT and MRI
Contrast-enhanced CT or MRI was reviewed for the presence of collateral vasculature in the perinephric space adjacent to the neoplasm as well as for enlarged vessels within the neoplasm. When present, the largest vessel in the perinephric space and/or neoplasm was measured on a Picture Archiving and Communication Software system using digital calibers, perpendicular to the long axis of the vessel. An enlarged vessel in the perinephric space is defined as any vessel >1 mm in diameter. Any discrete vessel that could be identified within the neoplasm was considered enlarged. The images were also evaluated for renal vein involvement and if present, whether a segmental branch or main renal vein was involved. Figures 1 and 2 demonstrate preoperative CT and MRI showing peritumor and intratumor vessels, respectively. Both patients had high-grade tumors on final pathology report.
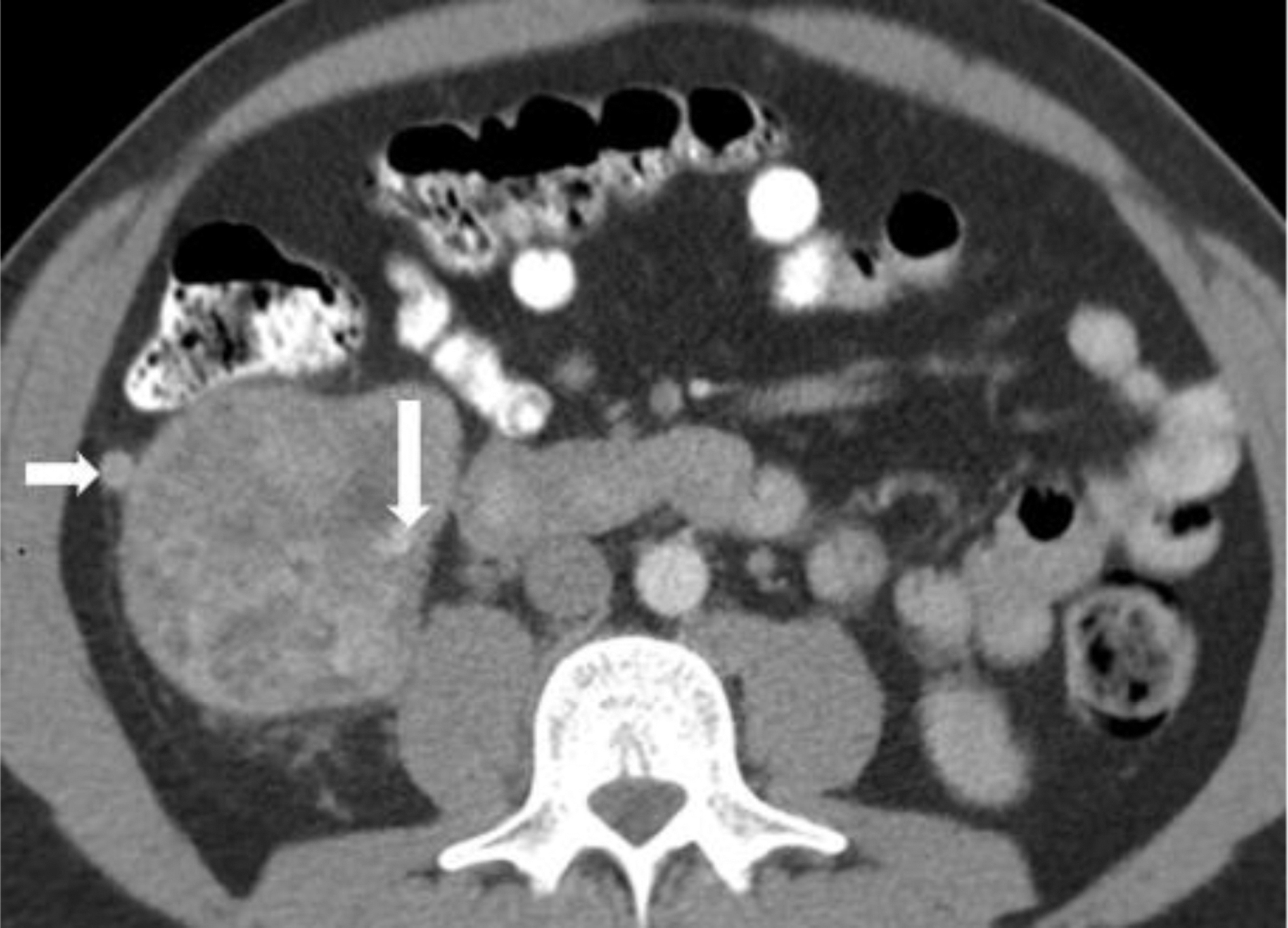
Axial CT image performed with IV and oral contrast demonstrates a right renal neoplasm containing a 6 mm intratumor vessel (long arrow) and 9 mm peritumor vessel (short arrow). Final pathology report: RCC, clear cell type, grade 3, pT3a, tumor extends into renal vein. RCC = renal cell carcinoma.

Axial fat suppressed T1-weighted MRI performed with IV contrast demonstrates a right renal neoplasm and peritumor vessels (arrows) measuring 5 mm. Final pathology report: RCC, clear cell type, grade 3, pT2b.
Statistical analysis
We analyzed 164 patients utilizing chi-square tests and Student's t-test to describe differences in demographic factors between high (>2) and low Fuhrman grade tumors. We utilized single and multivariable logistic regression to identify factors associated with high-grade tumors, with results considered significant if p ≤ 0.05. To develop multivariable logistic regression models, we first conducted univariable logistic regression for each variable, carrying forward all variables with p ≤ 0.1 into a final multivariable model. All analyses were conducted in R version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
More than 400 pathology reports were reviewed for patients undergoing either radical nephrectomy or partial nephrectomy between 2015 and 2020. Patients with tumors <3.0 cm (n = 146), missing demographic data (n = 39), and missing imaging reports (n = 65) were excluded from the study. One hundred sixty-four patients met the inclusion criteria for our final analysis. Of these 164 patients, 108 (65.85%) underwent radical nephrectomy and 56 (34.15%) underwent partial nephrectomy. Patients within our cohort had an average age of 62 years (range 26–93), an average BMI of 31.2 (range 19.5–51.5) and were predominantly male (74%).
The average tumor size on final pathology report was 6.4 cm (range 3.0–17.0 cm). Tumors were divided by pathologic stage, with stage T3a being the most common subtype (32.93%) followed by T1a (25.61%) and T1b (25.61%). Clear cell RCC made up 75% of the RCC subtypes followed by papillary Type 1 (9.15%) and papillary Type 2 (6.71%). Low-grade tumors were slightly more common making up 51.83% of our cohort. Additional tumor characteristics can be seen in Table 1.
Demographics, Tumor Characteristics, and Staging
BMI = body mass index; CKD = chronic kidney disease; RCC = renal cell carcinoma.
Of the 164 CT or MRI examinations that were reviewed, 92 (56.1%) had either an enlarged peritumor vessel (n = 72) or both a peritumor vessel and an intratumor vessel (n = 20). Only three patients had an isolated intratumor vessel without the presence of a peritumor vessel. These three patients were excluded from the final analysis. The presence of renal vein involvement or involvement of a segmental branch of the renal vein draining the tumor was also noted. Thirty-six patients (21.95%) had involvement of the renal vein and 11 patients (6.71%) had involvement of a segmental branch.
Of the 92 patients with either a peritumor vessel or both a peritumor vessel and intratumor vessel, 60.9% of these patients had high Fuhrman grade histology on final pathology report (60.9% vs 39.1%, p < 0.001). When controlling for renal vein involvement or involvement of a segmental vein, tumors with peritumor or intratumor vessels were still associated with high Fuhrman grade histology (61.4% vs 38.6%, p = 0.002). Subanalysis of the three patients with an intratumor vessel was performed. The average tumor size for these patients was 4.87 cm. None of these patients had high-grade histology.
Forty-two patients (25.61%) were pathologic stage T1a tumors with a tumor size between 3.0 and 4.0 cm. For T1a tumors, when an enlarged peritumor vessel was not present, 80% of tumors were of low grade. Pathologic stage T1a tumors with an enlarged peritumor vessel on preoperative imaging were associated with high Fuhrman grade histology (58.3% vs 41.7%, p = 0.015). Compared with pathologic stage T1a tumors, the relationship of Fuhrman grade histology to enlarged peritumor vessels and all other pathologic stages was variable, with higher pathologic stages, in general, more likely to have high Fuhrman grade (Table 2). Across all stages, the presence of an enlarged peritumor vessel was significantly associated with a high Fuhrman grade (odds ratio [OR]: 2.37, 95% confidence interval [CI] 1.17–4.9, p = 0.01).
Tumor Grade by Stage if Peritumor Vessel Present
Discussion
The utilization of imaging to predict tumor pathology analysis and aggressiveness has been described. 9 –11 The potential benefits are appealing. Being able to identify aggressive malignant tumors should be clinically useful. Larger tumors showing aggressive features on preoperative imaging can be planned for more aggressive surgical resection. For small renal tumors, <4.0 cm, patients considering AS should ideally have an absence of aggressive features on imaging. Up to now, the majority of series investigating renal tumor pathology analysis based on preoperative imaging has been limited to tumor enhancement and tumor morphology.
The diagnostic potential of contrast enhancement has been one area of interest. Alshumrani and colleagues showed a difference in contrast enhancement among clear cell RCC, oncocytomas, and papillary RCC tumors to be 65 HU, 80 HU, and 16 HU, respectively. 12 In another series investigating 122 patients who underwent contrast-enhanced MRIs, clear cell RCC had greater changes in signal intensity compared with papillary RCC (96.6% vs 32.1%, p < 0.001). 13 Moreover, compared with papillary RCC and chromophobe RCC, clear cell RCC has been more likely to demonstrate heterogenous enhancement. 14
Distinguishing between the different subtypes of RCC does not clearly distinguish tumor aggressiveness. For example, papillary Type II RCC tumors can be more aggressive than papillary type I RCC tumors. Clear cell RCC tumors are not all aggressive, and some clear cell RCC can be appropriately monitored on AS without an increase in mortality rate. Therefore, a method for distinguishing those tumors that are of higher grade may be more useful than the various histologic subtypes of RCC. Contemporary series investigating these factors are lacking.
One series showed tumors with an invasive/infiltrative pattern on imaging being associated with high-grade or sarcomatoid pathology analysis. 15 Another series identified an association of blood vessels surrounding the tumor with sarcomatoid RCC. 11 Our intraoperative observations of encountering peritumoral vessels often being associated with worse pathology analysis along with the aforementioned findings were ultimately the impetus for our study to further expand on this topic.
Our study shows that vessels surrounding the tumor were indeed associated with a high Fuhrman grade on final pathology report. This is the first study to investigate an association of vasculature around the renal tumor with high-grade histology for all RCC subtypes, and not only sarcomatoid RCC. When breaking down tumors by stage, the presence of a peritumor vessel persisted as significantly associated with high Fuhrman grade (OR: 2.37, 95% CI 1.17–4.9, p = 0.01) across all stages. These findings could have clinical implications. Patients with large renal masses planning to undergo surgical extirpation may be candidates for more aggressive resection.
Furthermore, although the debate persists about enucleation vs formal resection, these data might add to the argument for resection for those patients who have factors such as peritumor vessels that might predict more aggressive disease. As a pertinent negative, small renal masses (renal mass ≤4 cm) without a peritumor vessel may be more confidently selected as appropriate candidates for AS with 80.0% of these T1a tumors of low Fuhrman grade histology.
AS for small renal tumors, <4.0 cm, was once underutilized at rates between 10% and 20%. 5,16 Recent literature suggests increased utilization of AS. In the MUSIC trial, rates of AS among T1a tumors were 53.5%. 17 This increased utilization of AS was seen among academic and private practice. 17 Overwhelming evidence exists supporting the safety of AS for small renal tumors. Rare metastatic events were reported in the RCC Consortium of Canada (1.12%, 2/178 patients), 18 and no metastatic events were reported for AS patients in the Delayed Intervention and Surveillance for Small Renal Masses registry. 19
Most recently, a study investigating outcomes of AS for patients aged 60 or younger found no difference in overall survival between primary intervention and delayed intervention (94.0% vs 98.6%, p = 0.2) with a 100% cancer-specific survival in both groups. 20 Importantly, 30.4% of patients aged 60 years or younger chose AS further demonstrating increased utilization of this management strategy even in the younger patient. 20
With broader usage of AS of small renal masses, it is important to understand tumor characteristics associated with progression. A retrospective review of 123 small renal masses at a tertiary care cancer center showed when using standardized progression criteria for patients on AS, delayed intervention is more likely for tumors of high-grade histology (Fuhrman grade ≥3) or high stage (stage ≥T3a) on final pathology report. 21 Progression criteria used in the study included tumor growth >4.0 cm, growth rate >5 mm/year for tumors <3.0 cm and growth rate >3 mm/year for tumors >3.0 cm. 21 No metastatic events were reported in this study, again supporting the safety of vigilant AS for small renal masses.
However, another perspective on these findings is that tumors of high grade and high stage are more likely to progress and are destined for surgery. Therefore, a diagnostic tool to help identify patients with high-grade tumors may be clinically useful. High-grade small renal tumors are not rare, as one study found that ∼20% of small renal masses between 3.0 and 4.0 cm are of high-grade histology. 22 Of the 42 patients with renal tumors between 3.0 and 4.0 cm in our study, an association was seen between the presence of peritumor vessels and high-grade tumors. Indeed, further investigation to see if there is a survival benefit associated with these findings is warranted.
The findings of our study do not come without limitations. This was a retrospective study, which comes with inherent biases that exist within this type of study design. Tumors <3.0 cm and benign tumors were excluded from this study. Future research should focus on the relationship between peritumor vessels or intratumor vessels with tumors <3.0 cm and benign tumors. Both findings would be clinically useful as tumors <3.0 cm are commonly placed on AS. Furthermore, tumors without peritumor vessels can be surveilled with more confidence if associated with benign pathology report.
For this study, a single experienced GI reviewed and commented on the presence of peritumor vessels. Therefore, the generalizability and reproducibility of our findings are unknown. The findings of our study may have been strengthened with a design that utilized two radiologists to evaluate for interobserver agreement for identifying peritumor vessels. Despite these limitations, we do believe the findings of this study describe an expanding role for preoperative imaging in predicting renal tumor aggressiveness. The other strength of this finding is that the information for these findings already exists with all patients undergoing proper renal mass imaging.
Admittedly, this is purely speculation, but it is possible that the radiologic finding of peritumoral vessels could be a reflection of the biology of certain RCCs that have developed the ability for angiogenesis on the continuum of developing more aggressive disease. Future directions include validating this finding among a larger cohort of radiologists (and urologists) as well as prospectively following these patients. Ultimately, it would be highly valuable to research if peritumoral vessel identification in patients who are on AS or who get treated is an independent predictor of clinical outcome.
Conclusion
Our findings suggest that vessels surrounding small renal tumors and large renal tumors are associated with high tumor grade (FG ≥3). These findings can potentially help guide conservative and surgical management decisions of small and large renal masses. Further research is needed to support the association of peritumor vessels with high tumor grade.
Footnotes
Authors' Contributions
E.M.G., J.N., M.B., H.N., G.I., and D.S. made equal contributions to study design, data collection, data analysis, and article production.
Ethical Approval
Research conducted for this article was compliant with all ethical standards put forth by our institutional review board committee.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.