
Abstract
Objectives:
The aim of this study was to investigate the oncological outcomes and recurrence patterns in clinically node-negative patients with renal pelvic and/or upper or middle ureteral tumors after template-based retroperitoneal lymph node dissection (RPLND) in conjunction with retroperitoneal laparoscopic radical nephroureterectomy (LRNU).
Materials and Methods:
A total of 283 patients who received LRNU with and without RPLND at three Japanese institutions were enrolled. The template for RPLND included the renal hilar and para-aortic lymph nodes (LNs) (left side) and renal hilar, paracaval, retrocaval, and intra-aortocaval LNs (right side). The LNs and kidneys were removed en bloc. The primary endpoint was set as recurrence-free survival. All RPLND cases were matched one-to-one with no-RPLND cases using a propensity score matching approach, and 47 matched pairs were included in analyses.
Results:
Compared with the control group, significant differences were not observed in the RPLND group in terms of operation time, blood loss, postoperative complication rate, and pathological findings. The estimated 5-year recurrence-free survival was significantly higher in the RPLND group (86.8%) compared with the group without RPLND (64.2%) (p = 0.014). The estimated 5-year cancer-specific survival showed a similar tendency; however, it did not reach a statistically significant difference (87.5% vs 71.3%, respectively; p = 0.168). As for the first recurrence site, the RPLND group showed a lower incidence of distant recurrence, while no significant difference was observed in the rate of regional LN recurrence.
Conclusions:
This study suggests that template-based RPLND in conjunction with retroperitoneal LRNU efficiently improves recurrence-free survival by reducing distant recurrences.
Introduction
Upper tract urothelial carcinoma (UTUC) is a relatively rare cancer compared with bladder cancer and it accounts for 5%–10% of urothelial cancers. 1 The frequency of regional lymph node (LN) metastasis was reported to be as high as 15%–30%. Considering the possible survival benefit of lymph node dissection (LND) observed in muscle-invasive bladder cancer, one could hypothesize that LND in conjunction with radical nephroureterectomy (RNU) can improve survival in patients with UTUC. 2 –5
Indeed, template-based LND at the time of RNU for invasive UTUC is recommended in the European Association of Urology guidelines. 6 However, it was reported that LND is not widespread, and data about its oncological outcomes are still lacking.
Minimally invasive RNU, including laparoscopic RNU (LRNU), is currently a standard treatment option for organ-confined UTUC. 7 However, published reports on LND during minimally invasive RNU are limited and only provide few oncological outcomes. Urologic surgeons are unfamiliar with retroperitoneal lymph node dissection (RPLND) compared with pelvic LND during minimally invasive surgery, and it is speculated that laparoscopic RPLND for renal pelvic or upper ureteral tumors is underutilized. This is partly due to its technical difficulty and the lack of data for oncological outcomes.
A previously reported surgical technique can be performed to remove retroperitoneal LNs and kidneys en bloc using the retroperitoneal laparoscopic approach. 8 Its detailed perioperative complications were recently reported, 9 but the oncological outcomes of RPLND with en bloc kidney removal remain to be elucidated.
This multicenter study was conducted to investigate the effects of RPLND in conjunction with LRNU on cancer control and recurrence patterns in clinically node-negative patients with renal pelvic and/or upper or middle ureteral tumors.
Materials and Methods
This study was approved by the institutional review boards of Ijinkai Takeda General Hospital, Hamamatsu Rosai Hospital, and Rakuwakai Otowa Hospital (#R1581). The database of patients who underwent laparoscopic RNU at the three institutions from 2002 to 2020 was retrospectively reviewed. During this period, 283 patients underwent LRNU. 9 RPLND with retroperitoneal LRNU began in February 2009, as described previously. 8
The decision to perform RPLND for patients with renal pelvic tumors and upper or middle ureteral tumors was ultimately left to the surgeon's judgment. Of the 283 patients, 82 patients were excluded from the study cohort; these include 60 patients who had distal ureteral tumors only, 19 patients who had lymphadenopathy based on preoperative imaging (clinical stage N1–3), and 3 patients who did not have preoperative lymphadenopathy and underwent neoadjuvant chemotherapy. The final analysis included 201 patients.
Surgical technique
In this study, en bloc resection with RPLND during retroperitoneal LRNU was performed, as previously described with video presentations (Fig. 1). 8,9 The template for left-sided RPLND included the renal hilar and para-aortic LNs, while that for right-sided RPLND included the renal hilar, paracaval, retrocaval, and intra-aortocaval LNs. The caudal border was the level of aortic bifurcation.
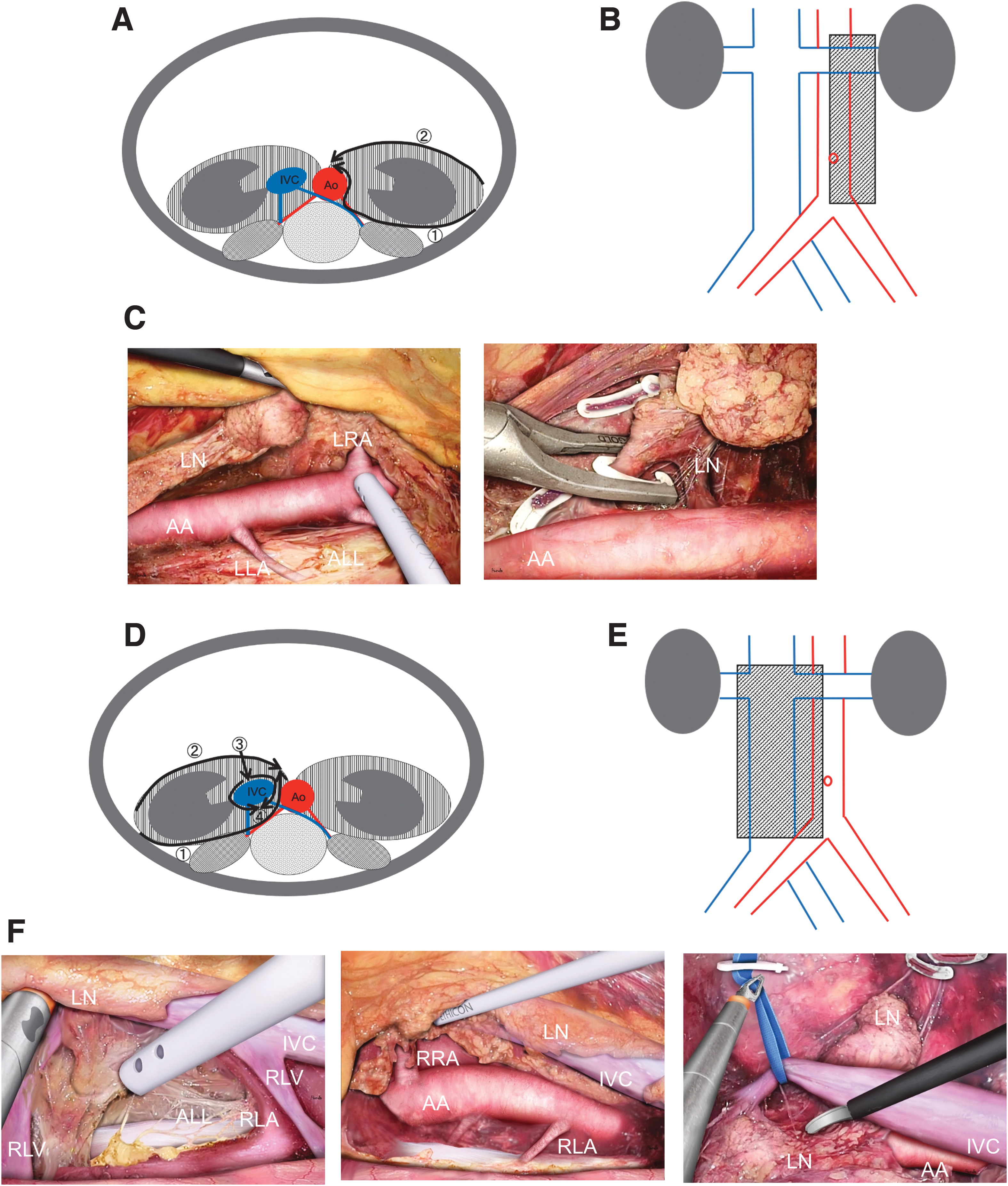
Left- and right-sided RPLND in conjunction with retroperitoneal LRNU.
The range of dissection and operative method in the three facilities were completely unified.
Left-sided RPLND in conjunction with retroperitoneal LRNU
By dissecting along the psoas muscle and anterior longitudinal ligament, the aorta and left lumbar arteries were exposed, and the para-aortic LNs were lifted (Fig. 1–C). The left renal artery and left renal vein were transected. The anterior aspect of the left kidney was fully mobilized from the underside of the peritoneal envelope. Next, the left kidney with para-aortic LNs was anterolaterally pulled to clarify the medial border of the dissected para-aortic LNs and it was clipped and transected.
The monobloc specimen of the para-aortic LNs attached to the left kidney was completely freed. The monobloc specimen was removed through an extraperitoneal lower abdominal midline incision after dissecting the lower ureter and managing the bladder cuff.
Right-sided RPLND in conjunction with retroperitoneal LRNU
The posterior plane of LNs was dissected, and the anterior longitudinal ligament was exposed (Fig. 1D–F). The right lumbar veins and arteries were identified, and veins were transected. The aorta, right renal artery, and right lumbar arteries were exposed, and the inferior vena cava (IVC) and retrocaval LNs were ventrally lifted. The right renal artery was clipped and transected, and the anterior aspect of the left kidney was completely mobilized from the peritoneum envelope.
The medial border of the template was dissected with clips. Then, the anterior IVC surface was longitudinally incised. Using a split-and-roll technique, the IVC was circumferentially dissected by transecting the remaining lumbar veins and right renal vein. The monobloc specimen of LNs attached to the right kidney was completely freed.
Primary and secondary outcomes
The primary endpoint of the study was the nonurothelial recurrence-free survival rate, while secondary endpoints were cancer-specific survival rates and the first recurrence site. Kaplan–Meier curves were obtained to elucidate the time to recurrence and survival.
The sites of recurrence were classified as distant (lung, liver, bone, brain, extraregional LN, and port site), local (nephrectomy bed, retroperitoneal, and regional LN), and intravesical. In particular, to investigate the effect of RPLND, recurrence in regional LNs was also investigated independently.
Postoperative complications were reported according to the modified Clavien-Dindo classification system, and grade 3–5 complications were regarded as high grades.
The decision of whether to perform adjuvant chemotherapy for patients with pathologically advanced UTUC was left to the responsible doctor. The patients were followed up by computed tomography and cystoscopy every 3–6 months within the first 2 years and every 6–12 months thereafter.
Statistical analyses
Statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). 10 Propensity scores for RPLND treatment were estimated using a logistic regression model with RPLND as the outcome, and these were calculated using age, gender, presence of hydronephrosis, and clinical T stage (≥T2 or less).
Matched-pair analysis was performed between patients undergoing RNU with RPLND and those without a one-to-one propensity score matching method using a caliper width of 0.2 for standard deviations. The association of RPLND with recurrence was evaluated with logistic regression models, and odds ratios and 95% confidence intervals were summarized.
The chi-square test or Fisher's exact test was used to determine any significant differences in normal data. Two-tailed Student's t-test or Mann–Whitney U test was used to analyze the differences in continuous variables. A p-value <0.05 was considered significant.
Results
Patient characteristics
A flow diagram of patient enrollment in this study is shown in Figure 2. Among the 201 patients who had renal pelvic and/or upper or middle ureteral tumors (clinical N0M0) and underwent retroperitoneal LRNU at the three institutions, 73 (36%) patients underwent RPLND and 128 (64%) patients did not undergo RPLND.

Flow diagram of patient enrollment.
After propensity score matching, 47 matched pairs with and without RPLND were analyzed (Table 1). The two populations had similar preoperative characteristics, such as age, clinical stage, gender, and tumor site, and were well balanced, with a standardized mean difference of ≤0.1 for each covariate, except for side.
Preoperative Characteristics Stratified by Performance of Retroperitoneal Lymph Node Dissection in the Entire and Matched Cohort
eGFR = estimated glomerular filtration rate; IQR = interquartile range; RPLND = retroperitoneal lymph node dissection.
Perioperative outcomes
Table 2 shows the intra- and postoperative findings. As for factors associated with surgical outcomes, there were no differences in operation time, blood loss, and postoperative complication rates. Significant differences were also not observed in cases with RPLND compared with the control group in terms of pathological findings, such as pathological stage, grade, and histological subtype.
Perioperative and Oncological Outcomes Stratified by Performance of Retroperitoneal Lymph Node Dissection in the Matched Cohort
The median number of LNs removed during RPLND was 9 (interquartile range, 5.0–13.5). No significant difference in the rate of adjuvant chemotherapy was also noted in both groups.
Oncological outcomes
The analysis using the Kaplan–Meier method showed that the estimated 5-year recurrence-free survival was significantly improved in the RPLND group (86.8%) compared with the group without RPLND (64.2%) (p = 0.0164) (Fig. 3A). Cox univariate analysis revealed that the hazard ratio for RPLND was 0.31 (95% confidence interval [CI], 0.11–0.85; p = 0.023) for recurrence-free survival.
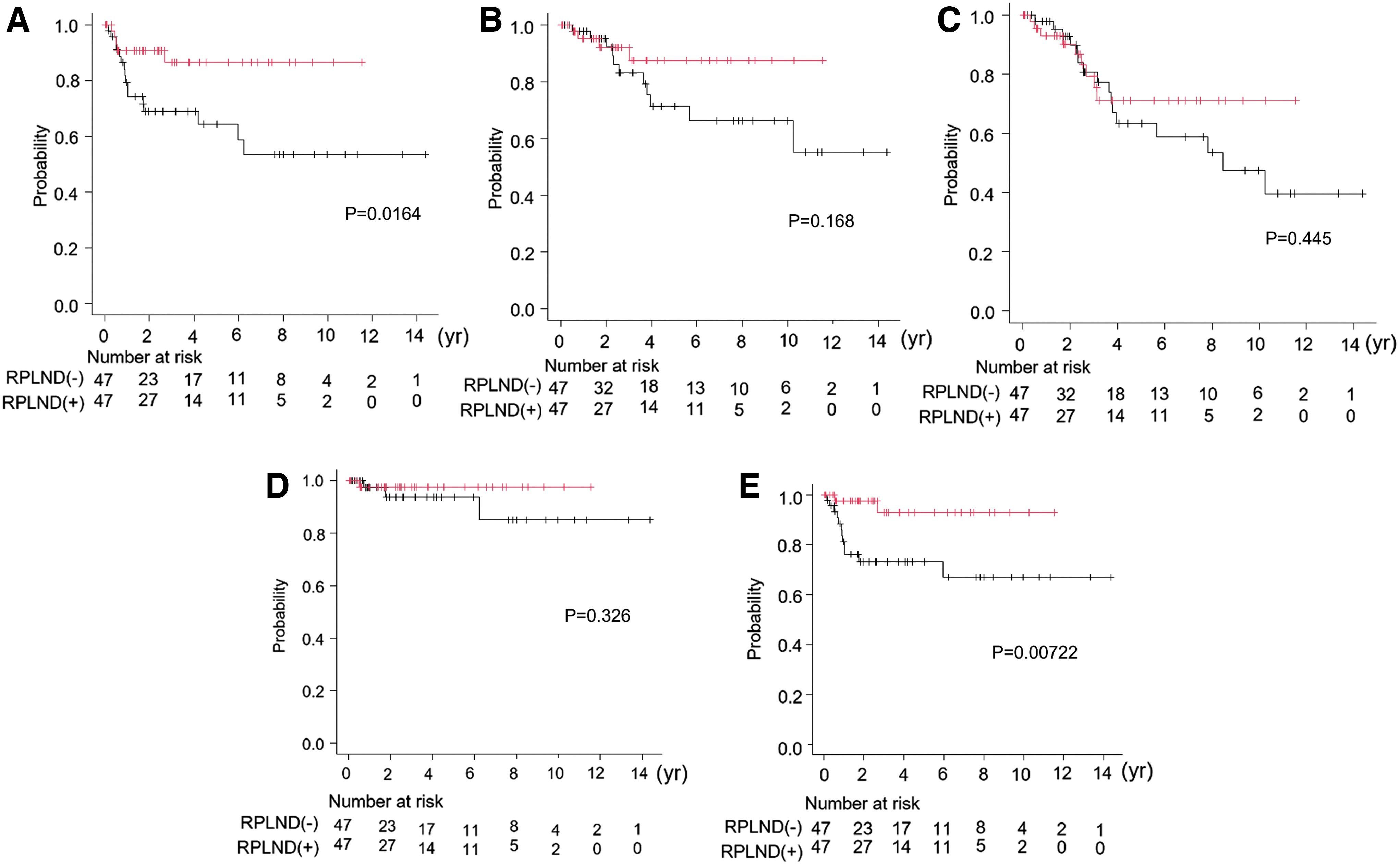
Kaplan–Meier curves showing the
The estimated 5-year cancer-specific survival showed a similar tendency; however, it did not reach a statistically significant difference (87.5% vs 71.3%, respectively; p = 0.168) (Fig. 3B), and the hazard ratio for RPLND was 0.45 (95% CI, 0.14–1.43; p = 0.144). The estimated 5-year overall survival also did not reach a statistically significant difference (Fig. 3C). The regional LN recurrence-free survival and metastasis-free survival were also analyzed (Fig. 3D, E).
Kaplan–Meier curves showed that there was no significant difference in the estimated 5-year regional LN recurrence-free survival (97.6% vs 93.6% in the groups with and without RPLND, respectively; p = 0.326). However, the estimated 5-year distant recurrence-free survival was statistically higher in the RPLND group (92.9%) than in the no-RPLND group (73.1%) (p = 0.0072).
A detailed examination of the first recurrence sites showed that the rates of local recurrence, including regional LN recurrence, were similar between the groups with and without RPLND (Table 2). In contrast, the rates of distant recurrences decreased significantly in the RPLND group compared with the no-RPLND group (4.3% vs 25.5%, respectively; p = 0.0038). Notably, there was a significant reduction in lung metastasis in the RPLND group (2.1% vs 21.3%, respectively; p = 0.010).
Discussion
In this Japanese multicenter study, we clarified that template-based RPLND in conjunction with retroperitoneal LRNU significantly improved the recurrence-free survival in clinically node-negative patients with renal pelvic and/or upper or mid ureteral tumors. Furthermore, the detailed analysis of recurrence sites revealed that the RPLND group showed a lower incidence of distant recurrence, while a significant difference was not observed in the rate of regional LN recurrence compared with the control group.
Although recent guidelines recommend lymphadenectomy for patients who were planned for RNU, 6,11 the impact of LND on survival outcomes of patients with UTUC remains controversial, 12 with some studies demonstrating a clear benefit, while others showing no difference. This discrepancy may be explained by several factors, including the variable LND template, completeness of LND, and heterogeneous patient inclusion criteria. 2,3
Indeed, several studies that described the template with a clear range of dissection showed improved survival with lymphadenectomy, while multicenter studies that did not clearly describe the template showed that lymphadenectomy had no therapeutic effects. 2,3 In addition, Kondo and colleagues reported that a complete LND improved the survival rates of patients with renal pelvic and upper/mid ureteral tumors compared with incomplete LND or no LND. 13
Several studies from Western databases reported significantly lower rates of performing RPLND for UTUC with LRNU than with open RNU, mainly due to technical concerns. 14 –16 Therefore, the number of reports about laparoscopic RPLND in patients with UTUC and renal pelvic and/or upper/mid ureteral tumors is extremely limited, and data about oncological outcomes after laparoscopic RPLND are scarce. We recently reported on the safety of RPLND during retroperitoneal LRNU in the same cohort, 9 and we believe that the current study is also significant.
Our retroperitoneal approach enabled easy access to the side and back of the aorta and IVC and complete removal of tissues around the great vessels, such as the para-aortic or retrocaval LNs. In addition, the thorough removal of lymphatic tissues in this template was made possible by removing LNs and kidneys en bloc during our surgical method.
In this study, we show that anatomical template-based RPLND significantly improved recurrence-free survival in patients with renal pelvic and/or upper/mid ureteral tumors. Consistent with our results, several groups also reported excellent oncological outcomes after a template-based lymphadenectomy.
Kondo and colleagues reported in a prospective study that an anatomical template-based lymphadenectomy significantly improved survival in patients with renal pelvic tumors, along with a significant reduction in regional node recurrence. 3,17 The authors speculated that the plausible reason for improvement of survival in patients who underwent RPLND may be the removal of LN micrometastasis.
Studies by Matsumoto and colleagues, which reported the long-term oncological outcomes of lymphadenectomy for 105 clinically node-negative patients with UTUC, 18 also backed up our results. In this study, better survival rates and local control rates were observed, although the control group was lacking. Interestingly, pan-cytokeratin immunohistochemistry revealed micrometastasis in five (4.8%) patients in addition to seven (6.7%) patients with LN metastasis detected by routine pathological examination. They concluded that anatomical LND could promote local disease control by eliminating micrometastasis in patients with clinically node-negative invasive UTUC.
In our current study, only 3 of 47 patients who underwent RPLND had pathologically confirmed positive LNs, but the RPLND group showed improved recurrence-free survival. We speculate that removal of the micrometastasis, which was not detected by routine pathological examination, might improve oncological outcomes.
Surprisingly, the improvement of oncological outcomes by RPLND was mainly due to significant reduction in distant recurrence, not regional LN recurrence. The reason for this is unclear, but we hypothesize that surgical resection of microtumor deposits inside regional LN tissues possibly contributed to the reduction in distant recurrences because micrometastasis in the regional LN is thought to be the site of initial metastasis and can trigger late distant metastasis.
This study had several limitations that should be addressed. First, this was a retrospective study. Therefore, although the propensity score matching method was used, the possibility of bias cannot be excluded. Second, the number of matched pairs and follow-up duration were limited. Third, the involvement of several surgeons in this multicenter study can influence its results even though uniform dissection templates and surgical procedures were adopted.
However, this study is believed to have important implications because reports about oncological outcomes after laparoscopic RPLND for node-negative UTUC are scarce.
Conclusions
This study shows that anatomical template-based RPLND in conjunction with retroperitoneal LRNU efficiently improves the recurrence-free survival rates, possibly by reducing distant recurrences.
Footnotes
Authors' Contributions
T.K. and H.Y. contributed to study conception and design. T.K., G.K., H.N., T.T., N.T., and S.S. contributed to acquisition of patients' data. T.K. contributed to analysis and interpretation of the data and statistical analysis. T.K., K.N., M.I., Y.M., and Y.H. contributed to drafting the manuscript. T.K., K.I., and H.Y. contributed to revising it. H.Y. contributed to obtaining funding. G.K., K.I., and M.I. contributed to administrative, technical, or material support. S.M., T.A., and H.Y. contributed to supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.