
Abstract
Purpose:
While erectile dysfunction and urinary incontinence are commonly cited side effects following radical prostatectomy (RP), climacturia and penile length shortening are less explored. The present study seeks to explore the incidence, risk factors, and predictors of recovery associated with climacturia and penile length shortening following robot-assisted radical prostatectomy (RARP).
Patients and Methods:
From September 2018 to January 2020, 800 patients underwent RARP for primary treatment of localized prostate cancer. A survey was sent to patients following 1-year follow-up assessing outcomes of continence, erectile dysfunction, climacturia, and penile length shortening. Descriptive statistics were utilized to describe incidence and risk factors and logistic regression modeling was used to identify predictors associated with recovery.
Results:
Of the 800 patients surveyed, 339 (42%) and 369 (46%) patients responded, with 127/339 (37.5%) and 216/369 (58.5%) endorsing climacturia and penile length shortening. In univariate analysis, a lack of bilateral nerve sparing was associated with climacturia; high body mass index (BMI), high prostate weight, lack of nerve-sparing, and high pathologic stage was associated with penile length shortening.
In logistic regression modeling, BMI, prostate weight, and p-stage were all significantly correlated with penile length shortening. Recovery from climacturia was associated with a preoperative International Index of Erectile Function-5 score >21. When patients were asked to rank the importance of these outcomes compared to erectile dysfunction and incontinence, <5% of patients ranked either climacturia or penile length shortening as a high priority following RP.
Conclusion:
While incidence of climacturia and penile length shortening following RP is significant, impact on patient- and partner-related quality of life are low in comparison to risks of erectile dysfunction and urinary incontinence.
Introduction
Prostate cancer (PCa) is the most common noncutaneous malignancy for men, with an estimated incidence of 1.4 million per year. 1 For these patients, the robot-assisted radical prostatectomy (RARP) is a common treatment for localized PCa. Common side effects of RARP include a 54% to 90% rate of erectile dysfunction and a 4% to 31% rate of urinary incontinence. 2,3 Less commonly studied side effects, however, include climacturia and penile length shortening.
Climacturia, the involuntary loss of urinary continence following sexual climax, is a common, yet less-studied side effect of RARP. In a study of 62 patients, Parra López et al. found that climacturia occurs in 20% to 40% of patients following RARP. However, none of the analyzed parameters could be defined as predictors of climacturia. 4 Similarly, a study of 42 patients by Lee et al. found the prevalence of climacturia in radical prostatectomy (RP) patients to be 45% and found no significant predictors. 5 O'Neil et al. found that the use of aides in achieving an erection as well as urinary incontinence were associated with climacturia in a study of patients receiving definitive PCa treatment via surgery and/or radiation. 6
Penile length shortening is another side effect of RP that impacts many patients but lacks robust literature. Kadono et al. found that the mean penile length shortening was 19.9 mm 10 days post-RP. The study of 102 patients found no significant predictor of penile length shortening at 12 months post-RP. 7 In contrast, a study by Vasconcelos et al. found a statistically significant reduction in penile length by 1 cm after 12 months. Penile length recovery was noted 48 months after RP and preserved erectile function was a predictor of penile length recovery. 8
While these studies begin to address under-represented side effects of RP, they are limited by low power, significant heterogeneity in patient populations, and do not provide context for impact on quality of life. Within this context, the present study seeks to explore the incidence, risk factors, and predictors of recovery associated with climacturia and penile length shortening following RARP. We also contextualize these results within patient concerns and quality of life, aiming to compare patient concern for climacturia and penile length shortening in comparison to side effects of erectile dysfunction and urinary incontinence following RARP.
Patients and Methods
Patient population
In 2010, 800 patients underwent RARP for the primary treatment of localized PCa at a single institution. Patients undergoing simple or cytoreductive prostatectomy, those undergoing adjuvant therapies, or those with pre-RARP treatments were not eligible for inclusion. Patients were sent a survey regarding their experience with urinary continence, erectile dysfunction, climacturia, and penile length shortening following 1-year follow-up from the date of the initial procedure. All data were retrospectively collected and entered electronic databases, under approval from Institutional Review Board protocols (HS No. 1998-84). All data collection was conducted in compliance with the Health Insurance and Accountability Act, and federal guidelines for informed consent were followed.
Data collection and outcome measures
All patients were screened before RARP with the International Index of Erectile Function-5 (IIEF-5), American Urological Association Symptom Score (AUASS), and urinary quality of life questionnaires—derived from the AUASS questionnaires. Demographic and clinical information was collected prospectively via electronic medical record review. The main outcome measures were incidence and risk factors of climacturia and penile length shortening following RARP—measured subjectively by patients. Secondary outcome measures included a ranking of climacturia and penile length shortening against risks of erectile dysfunction and urinary continence outcomes.
Surveys were administered via REDCap—research electronic data capture, a HIPAA-compliant online questionnaire—and sent automatically with three reminders, 3 days apart. If no response was received within 14 days of initial survey, two phone calls by research staff were made to reach all patients in the cohort. Patients were contacted multiple times to allow for follow-up data. These surveys were conducted at 3, 9, 15, and 24 months postoperative and every year then after.
Statistical analyses
All statistical analyses were conducted in the Statistical Package for Social Sciences (SPSS) version 25 (© IBM Corp., Armonk, NY). Baseline demographics and clinical characteristics were summarized utilizing descriptive statistics, such that categorical variables were reported with n and % and continuous variables were reported with a mean and standard deviation. Univariate associations between these variables and incidence of climacturia and penile length shortening were assessed via Student's t-test for continuous variables and Pearson chi-square tests for categorical variables. Distribution of variables were assessed utilizing Levene's test for equality of variances. For variables violating homoscedasticity assumptions, the Mann–Whitney U test was utilized.
Variables yielding a p-value <0.15 on univariate analysis were included in multivariate modeling via linear and logistic regression models predicting climacturia and penile length shortening. A p-value <0.05 was considered statistically significant and 95% confidence intervals were reported for all odds ratios.
Results
Of the 800 patients surveyed, 339 (42%) and 369 (46%) patients responded, with 127/339 (37.5%) and 216/369 (58.5%) endorsing climacturia and penile length shortening.
Climacturia
Table 1 depicts demographic and clinical characteristics associated with climacturia status. The only variable associated with climacturia in univariate analysis was a lack of bilateral nerve sparing status. No other variables were significantly associated with climacturia. Multivariate analysis is not shown.
Clinical and Oncologic Demographics, Stratified By Climacturia Status
The bold values are significant variables.
AUA = American Urological Association; BMI = body mass index; IIEF-5 = International Index of Erectile Function-5; PSA = prostate specific antigen; SD = standard deviation.
Ad hoc analysis was conducted to determine recovery status. Of the initial 339/800 (37%) patients initially endorsing climacturia following RARP, 107 (31.5%) recovered at a median follow-up of 5 years. Table 2 illustrates a logistic regression model of factors predicting climacturia recovery, such that patients reporting a preoperative IIEF-5 score 22 to 25 were 3.9 times more likely to recover from climacturia, compared to those with an IIEF-5 score less than 22.
Logistic Regression of Factors Predicting Climacturia Recovery
The bold values are significant variables.
CI = confidence interval; OR = odds ratio; SE = standard error.
Penile length shortening
Table 3 illustrates demographic and clinical characteristics associated with penile length shortening. A lack of bilateral nerve sparing, a high body mass index (BMI), high prostate weight, and higher pathologic stage were also associated with penile length shortening. In the multivariate analysis illustrated in Table 4, penile length shortening was significantly associated with increased BMI, prostate weight, and higher pathologic stage. Nerve-sparing status and age were not significantly associated with penile length shortening.
Clinical and Oncological Demographics, Stratified By Penile Length Shortening Status
The bold values are significant variables.
PLS = penile length shortening.
Multivariable Analysis of Factors Contributing to Penile Shortening
Quality of life
Figure 1 demonstrates the concern of adverse effects post-RP. Figure 2 illustrates the concern of adverse effects compared to biochemical recurrence. When patients were asked to rank the importance of these outcomes compared to biochemical recurrence, 5% of patients ranked climacturia as a greater concern while 12% of patients ranked penile length shortening as a greater concern following RP. Furthermore, when asked to rank the importance of erectile dysfunction, urinary incontinence, climacturia, and penile length shortening, less than 5% of patients ranked either climacturia or penile length shortening as a high priority following RP.

Patient concern of adverse events postradical prostatectomy. BCR = biochemical recurrence; ED = erectile dysfunction; PLS = penile length shortening. Color images are available online.
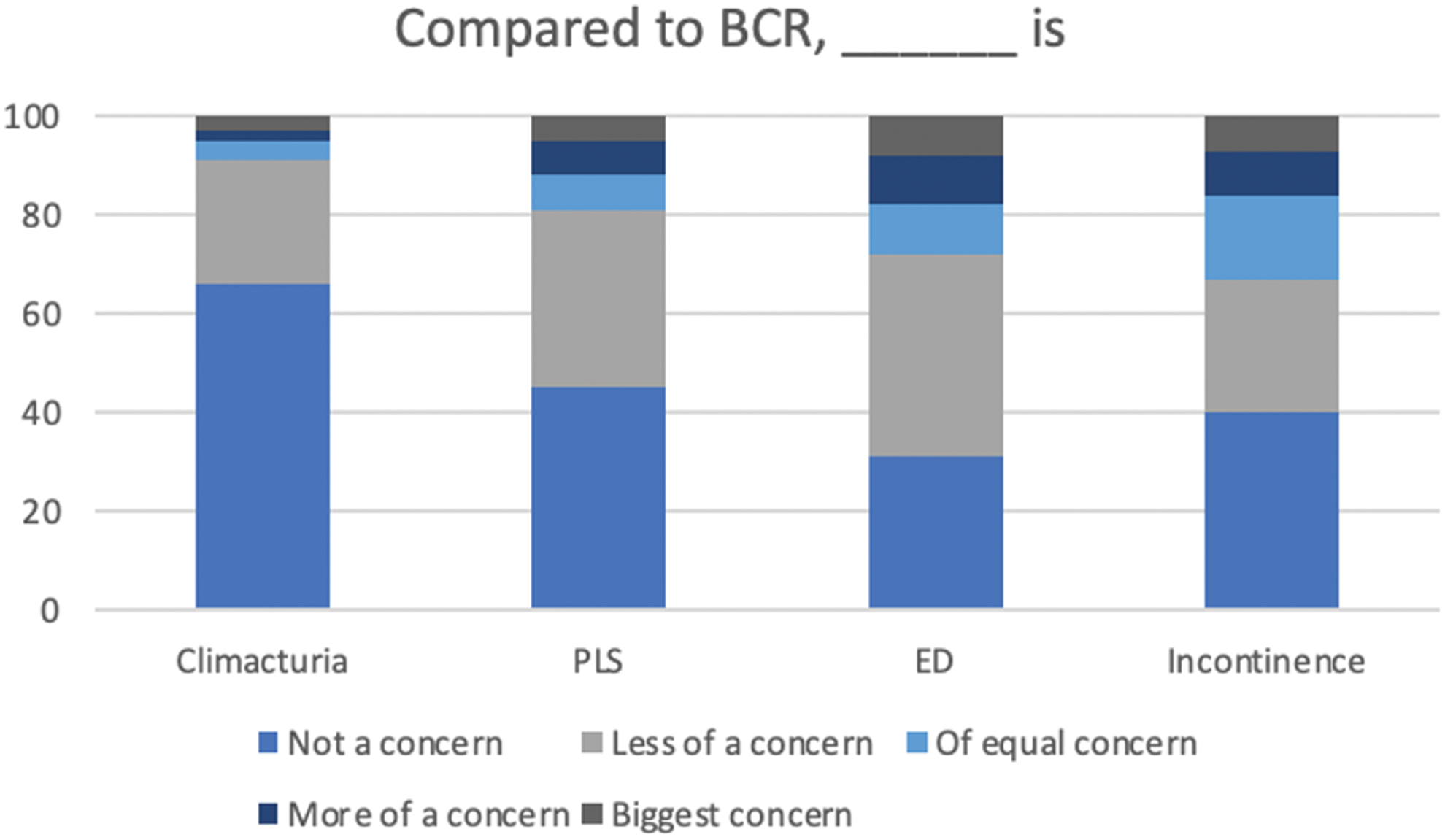
Concern of adverse events compared to BCR. Color images are available online.
Figure 3 depicts results of an orgasm-related quality of life item on our questionnaire. Of the 339 patients and partners surveyed, 271 patients and partners (79.9%) reported that they were mostly satisfied, pleased, or delighted with their orgasm-related quality of life.
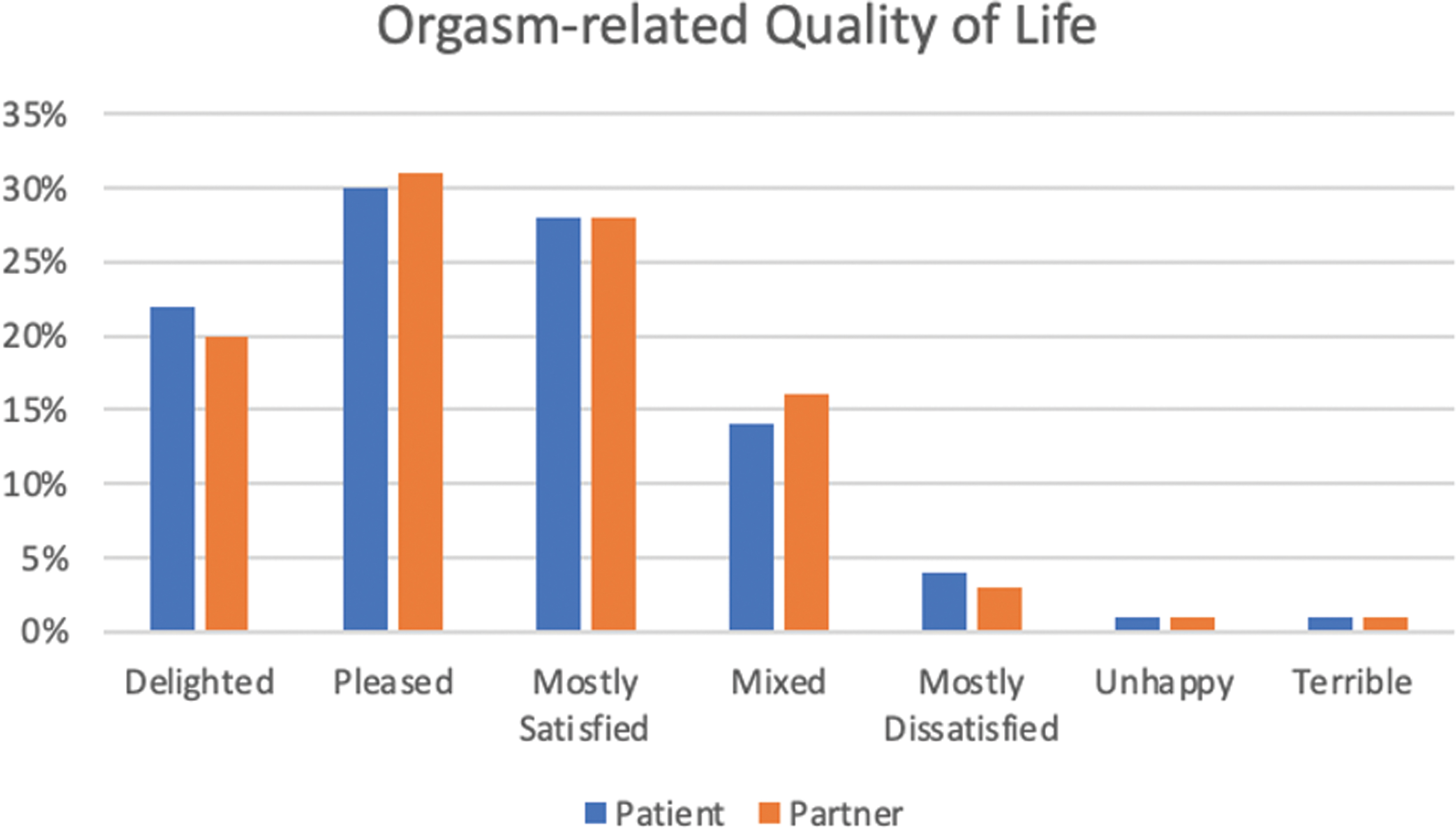
Patient-reported orgasm-related quality of life following robot-assisted radical prostatectomy. Color images are available online.
Discussion
In this survey of 800 patients who underwent RP for primary treatment of localized PCa, ∼37.5% and 59% of patients reported experiencing climacturia and penile length shortening. Risk factors for these adverse effects included a lack of bilateral nerve sparing, high BMI, high prostate weight, and higher pathologic stage at the time of RARP. While the proportion of patients reporting these effects are significant, when contextualized within PCa treatment and potential for erectile dysfunction and urinary incontinence, less than 5% of patients ranked either climacturia or penile length shortening as a high priority concern. These findings not only add to risk stratification efforts for identifying patients at-risk for climacturia and penile length shortening but also contextualize the importance of these findings within PCa treatment.
First, the current study represents the largest cohort of patients examined for risk factors associated with climacturia specifically following RARP. A 2014 systematic review of neglected side effects after RP identified a total of 43 articles reporting that 20% to 93% of RP patients experienced orgasm-associated incontinence. 9 The two largest studies examined risk of climacturia in unique contexts. First, a 2007 study by Choi et al. investigated the incidence of orgasm-associated incontinence between open and laparoscopic RP, respectively. Other than surgical technique, however, authors were unable to identify a correlation between orgasm-associated incontinence with nerve-sparing status, urinary incontinence, or age. 10 Similarly, a 2010 study on the University of California Los Angeles prostate cancer index could not distinguish between orgasm-associated incontinence and urinary incontinence at the time of sexual stimulation.
Combined, this study reported 36% of patients experiencing some degree of sexual bother related to urinary continence—a proportion of patients similar to the current study. 11 A third study, by Nilsson et al., found in a survey study of 1288 men after either an open or RARP that about a fifth (268 men) experienced climacturia. 12 However, in contrast to these three previous explorations, the present study identified nerve-sparing status as a potential risk factor for climacturia. Similarly, in multivariate analysis, it was found that pre-existing erectile dysfunction (i.e., pre-operative IIEF-5 score less than 22) impedes recovery from climacturia following RARP.
Distinct from climacturia, 59% of patients in the present study reported penile length shortening. This value is similar to that of an initial study by Fraiman et al., illustrating a penile shortening of >1 cm in 45% of patients undergoing open prostatectomy. 13 However, more recent explorations by Briganti et al. have shown a lack of penile shortening for patients who maintained their erectile function following surgery. This leads to the conclusion that preserving erectile function preserves penile length and girth. 14 In addition to this postoperative phenomenon, this study has also identified BMI, pathologic stage, and prostate weight to be significant predictors of penile length shortening. This finding is challenged by Engel et al. who reported that, while penile length shortening was observed postoperatively, penile length had returned to preoperative lengths by 9 months. 15
Given these findings, it is important to contextualize these outcomes within RP, cancer recurrence, erectile dysfunction, and urinary incontinence. Despite 46% and 37.5% of patients reporting climacturia and penile length shortening, respectively, when patients were asked to rank the importance of these outcomes compared to erectile dysfunction and incontinence, <5% of patients ranked either climacturia or penile length shortening as a high priority following RP (Fig. 1). Furthermore, when asked to rank the importance of these outcomes compared to biochemical recurrence, 5% of patients ranked climacturia as a greater concern while 12% of patients ranked penile length shortening as a greater concern following RP (Fig. 2). Finally, when asked to assess orgasm-related quality of life, ∼80% of patients reported that they were mostly satisfied, pleased, or delighted with their orgasm-related quality of life—despite over 45% reporting either climacturia or penile length shortening (Fig. 3).
The current study has several limitations to consider. First, all outcomes were assessed via patient-reported surveys and no quantitative measurements were taken. Patient-reported surveys are imperfect research tools that limit the validity of results and conclusions compared to other methodologies. For example, given that penile length shortening and quality of orgasm are closely related, it is difficult to discern directionality and causation in this relationship. Similarly, climacturia recovery was assessed at a median of 5 years following RARP; as such, recovery over time was unable to be assessed and recall bias may have overestimated recovery rates. Ad hoc analysis revealed normal preoperative sexual function (defined as an IIEF-5 of 22–25) to correlate with climacturia recovery. Finally, the present study was a single surgeon experience; as such, the effect of surgical technique on climacturia and penile length shortening was unable to be assessed.
Overall, in the present study, there is significant incidence of climacturia and penile length shortening following RP. Patient-related factors such as high BMI, high prostate, lack of nerve-sparing procedures, and high-risk disease may contribute to risk of these outcomes. However, when contextualized with risk of cancer recurrence, erectile dysfunction, and urinary incontinence, patients did not prioritize climacturia and penile length shortening as concerns following RARP.
Footnotes
Acknowledgments
The research presented in full in this article was also presented at the European Urological Association in July 2022 in Amsterdam. While our article was under review in Journal of Endourology, we provided a version of this work to AUA News where it was published in October 2022.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This study is self-funded.