
Abstract
Background:
Laparoscopic nephroureterectomy (LNU) has become popular in treating upper urinary tract urothelial carcinoma (UTUC) and an emerging trend was observed in robotic approaches. Therefore, we compared robot-assisted radical nephroureterectomy (RANU) and LNU for the treatment of UTUC.
Materials and Methods:
This observational and retrospective case-series study included UTUC patients who underwent LNU or RANU. A pure laparoscopic approach was adopted in the LNU treatment group, and bladder cuff excision (BCE) was performed mostly with the open approach. Either the da Vinci Si or Xi surgical system was used for RANU. Extravesical BCE was performed, and bladder defects were closed intracorporeally. Perioperative and oncologic outcomes were compared between the LNU and RANU groups.
Results:
A total of 231 patients who underwent RANU (n = 87) or LNU (n = 144) were included. No significant differences were noted between the groups in terms of demographics, tumor characteristics, operative time, catheter time, or complications. Compared with LNU, RANU had a lower intraoperative blood loss (30 vs. 150 mL, p < 0.001) and shorter postoperative hospital stay (8 vs. 9 days, p = 0.009). The 5-year overall survival, cancer-specific survival, and bladder recurrence-free survival were comparable between the groups.
Conclusion:
Compared with LNU, RANU had similar perioperative and oncologic outcomes but was superior in terms of intraoperative blood loss and postoperative length of hospital stay. However, considering the potential biases owing to the heterogeneity of our cases, the interpretation of the results must be very cautious.
Introduction
Upper urinary tract urothelial carcinoma (UTUC) is a rare cancer, accounting for only 5% of all urothelial malignancies. 1,2 However, in Taiwan, it contributes to up to 20% to 25% of all urothelial malignancies. 3 –5 This prevalence of UTUC in Taiwan is unique compared with that noted in other countries, and its management has become an important public local health issue. Open nephroureterectomy (NU) with bladder cuff excision (BCE) is one of the surgical treatment modalities for UTUC patients, regardless of the tumor location. 6 Alternatively, laparoscopic nephroureterectomy (LNU) with BCE has been researched and performed for decades, and previous studies have shown that it has similar oncologic outcomes, better cosmesis, and comparable perioperative outcomes compared with its open counterpart 7,8 ; thus, LNU has gained popularity worldwide. 9
Several previous reports have demonstrated the perioperative feasibility and safety of robot-assisted radical nephroureterectomy (RANU) with BCE for UTUC. 10,11 However, only few studies comparing RANU with LNU have shown similar oncologic outcomes but better perioperative outcomes for RANU. 12 With the updated robotic system and advancing surgical techniques these years, the adoption of RANU in the treatment of UTUC has increased gradually. Moreover, in Taiwan, the increased prevalence of UTUC has provided more experience regarding its treatment. Thus, an investigation of the use of a robotic approach in NU with BCE in comparison with LNU may provide insight into improving surgical outcomes. To address this, we conducted a study to compare LNU and RANU in patients with UTUC.
Materials and Methods
Patients
This observational and retrospective case-series study was ethically approved by the Institutional Review Board (2020-12-007BC) from a prospectively maintained database; patients who underwent RANU or pure LNU between March 2012 and October 2017 for UTUC were retrospectively identified. The patients were divided into the RANU or LNU treatment groups. The type of surgical approaches was decided by individual surgeon. All surgeons involved were experienced in laparoscopic and robotic surgeries. Patients who underwent hand-assisted approaches, had distant metastasis, or received kidney transplantation were excluded. Lymph node dissection (LND) was not performed routinely unless enlarged lymphadenopathy was obvious upon preoperative computed tomography (CT) or magnetic resonance imaging (MRI).
Surgical procedures
Both da Vinci Si and Xi surgical systems (Intuitive Surgical, Sunnyvale, CA) are available at our institution. The Si system had been available since 2009 and Xi since 2017. Patients operated with the Si system were placed in the lateral flank position after general anesthesia. All procedures were performed with all four robotic arms. A 12-mm camera port was placed 1 cm lateral to the umbilicus, and an 8-mm robotic trocar was placed at the level of the umbilicus 10 cm away from the camera port. Two additional robotic trocars were placed at the midclavicular line 10 cm away from the camera port below the costal margin and at the anterior axillary line at the level of the iliac crest. A 12-mm assistant trocar was placed at the lower midline ∼5 cm below the umbilicus (Fig. 1A). The robotic system was first docked from the patient's shoulder at a 45° angle, facing the contralateral hip. Radical NU was performed in a standard manner, with the renal pedicle controlled by a laparoscopic endovascular stapler. After completion of the radical NU, the system was re-docked from the patient's hip at a 45° angle, facing the contralateral shoulder toward the distal ureter and bladder cuff. The assistant trocar was switched to the port below the costal margin. Distal ureterectomy and BCE were performed extravesically, and the urinary bladder defect was closed intracorporeally. Specimens were placed in a specimen retrieval bag and extracted from a lower midline incision extending from the assistant port.

Patient positioning for the Xi system was the same as that for the Si system. The first trocar was placed superior and lateral to the umbilicus at the paramedian line. Another trocar was placed 8 cm superior to the first trocar. The additional two trocars were placed inferior to the first trocar. All the trocars were arranged in a straight paramedian line and were ∼8 cm apart from each other. The 12-mm assistant trocar was inserted at the lower midline ∼5 cm below the umbilicus (Fig. 1B). For the NU, the robotic system was docked perpendicular to the operation table and the boom was targeted toward the kidney. The upper second trocar was assigned as the camera port. The operation with the Xi system was performed similar to that with the Si system. However, the Xi system was not re-docked after NU. Instead, the boom was retargeted toward the distal ureter and the camera port was switched from the upper second trocar to the third trocar.
Patients who underwent LNU were placed in the lateral flank position. A 12-mm camera port was placed 1 cm lateral to the umbilicus. Three 12-mm trocars were inserted at the subxyphoid, lower midline, and lower lateral quadrant. Once pure laparoscopic NU was completed, either a 7-cm Gibson's or lower midline incision was created for open distal ureterectomy and BCE or pure laparoscopic intracorporeal BCE was performed. The adoption of open or pure laparoscopic BCE was primarily at surgeons' discretion.
Data collection
UTUC grading and staging was performed according to the 2004 World Health Organization grade classification and the American Joint Committee on Cancer 7th edition (2009). Complications were graded according to the Clavien–Dindo classification system. 13 The follow-up protocol included physical examination, laboratory tests, imaging studies (e.g., sonography, CT, or MRI), and cystoscopy performed every 3 to 6 months. Disease progression was defined as radiologic or pathologic evidence of local recurrence, distant metastasis, or mortality rate from UTUC. Local recurrence was defined as ipsilateral nephrectomy bed, retroperitoneal lymph node, or pelvic lymph node recurrence. Distant metastasis was defined as organ or lymph node metastasis beyond the retroperitoneum or pelvis. Demographic data, histopathologic reports, perioperative complications, and oncologic outcomes were evaluated.
Statistical analysis
Continuous variables were reported as median and interquartile range and were compared using the Mann–Whitney U test. Categorical variables were reported as number and proportions and were compared using the Fisher's exact test. Survival rate and survival time were calculated according to the life table method. Survival curves were generated by Kaplan–Meier analysis and compared by log-rank test. A two-sided value of p < 0.05 was considered statistically significant. All statistical analyses were conducted using SPSS software for Windows version 22 (IBM, Armonk, NY).
Results
In total, 239 patients underwent RANU or LNU within the study period. We enrolled 231 patients who met the inclusion criteria (87 with RANU and 144 with LNU). Among the 87 patients in the RANU group, 79 (90.8%) underwent the operation with the Si system and 8 (9.2%) with the Xi system. There were no differences in baseline demographic and tumor characteristics between the RANU and LNU groups (Table 1).
Demographic and Tumor Characteristics in Patients Treated with Robotic-Assisted Radical Nephroureterectomy or Laparoscopic Nephroureterectomy for Upper Urinary Tract Urothelial Carcinoma
Data are given as count (percentage) or median (interquartile range).
Lymph node dissection is not routinely performed, and pNx represents patients whose lymph node specimen did not show metastasis after lymph node sampling or patients did not undergo lymph node sampling.
p-Values were calculated using Fisher's exact test or Mann–Whitney U test.
One patient whose final pathology analysis did not reveal a tumor, but biopsy pathology analysis revealed urothelial carcinoma of the ureter.
ASA = American Society of Anesthesiologists Physical Status Classification System; LNU = laparoscopic nephroureterectomy; RANU = robotic-assisted radical nephroureterectomy.
Perioperative outcomes
Compared with patients in the LNU group, patients in the RANU group had a significantly lower estimated blood loss (30 vs. 150 mL, p < 0.001) and shorter postoperative hospital stay (8 vs. 9 days, p = 0.009). Total operative time and postoperative catheter time were similar between the groups (Table 2). Regarding the BCE approach, all patients in the RANU group had pure laparoscopic approaches. In patients in the LNU group, there were more open approaches with Gibson's incision than with the lower midline incision (72.2% vs. 13.2%). Only 21 (14.6%) patients underwent pure laparoscopic BCE.
Perioperative Outcomes in Patients Treated with Robot-Assisted Radical Nephroureterectomy or Laparoscopic Nephroureterectomy for Upper Urinary Tract Urothelial Carcinoma
Data are given as count (percentage) or median (interquartile range).
p-Values were calculated using Fisher's exact test or Mann–Whitney U test.
BCE = bladder cuff excision.
LND was not performed routinely unless enlarged lymphadenopathy was obvious upon preoperative CT or MRI. There were 9 patients (10.3%) who accepted LND in the RANU group and 15 patients (10.4%) in the LNU group for enlarged lymph nodes. The surgical modality was the same for patients who accepted LND in both groups. The perioperative outcomes including operative time, blood loss, and complications between patients who accepted LND versus no LND were not different both in RANU and LNU groups (Supplementary Table S1).
Operative and postoperative complications showed no differences between the groups. There was one grade 3 intraoperative complication in each group. No conversion was needed in either case. There were no high-grade postoperative complications encountered.
Pathologic results were similar between groups. There were no significant differences in tumor grade and pathologic T and N stages between groups (Table 1).
Oncologic outcomes
Patients in the LNU group had a longer follow-up duration than those in the RANU group (29 vs. 20 months, p = 0.006). No significant differences were noted in incidence of bladder recurrence, adjuvant chemotherapy, disease progression, local recurrence, distant metastasis, cancer-specific mortality rate, or overall mortality rate between the RANU and LNU groups (Table 3). Kaplan–Meier survival analysis revealed no significant difference in the 5-year overall survival (p = 0.534), cancer-specific survival (p = 0.923), or bladder recurrence-free survival (p = 0.363) between the patients treated with RANU versus LNU (Fig. 2).
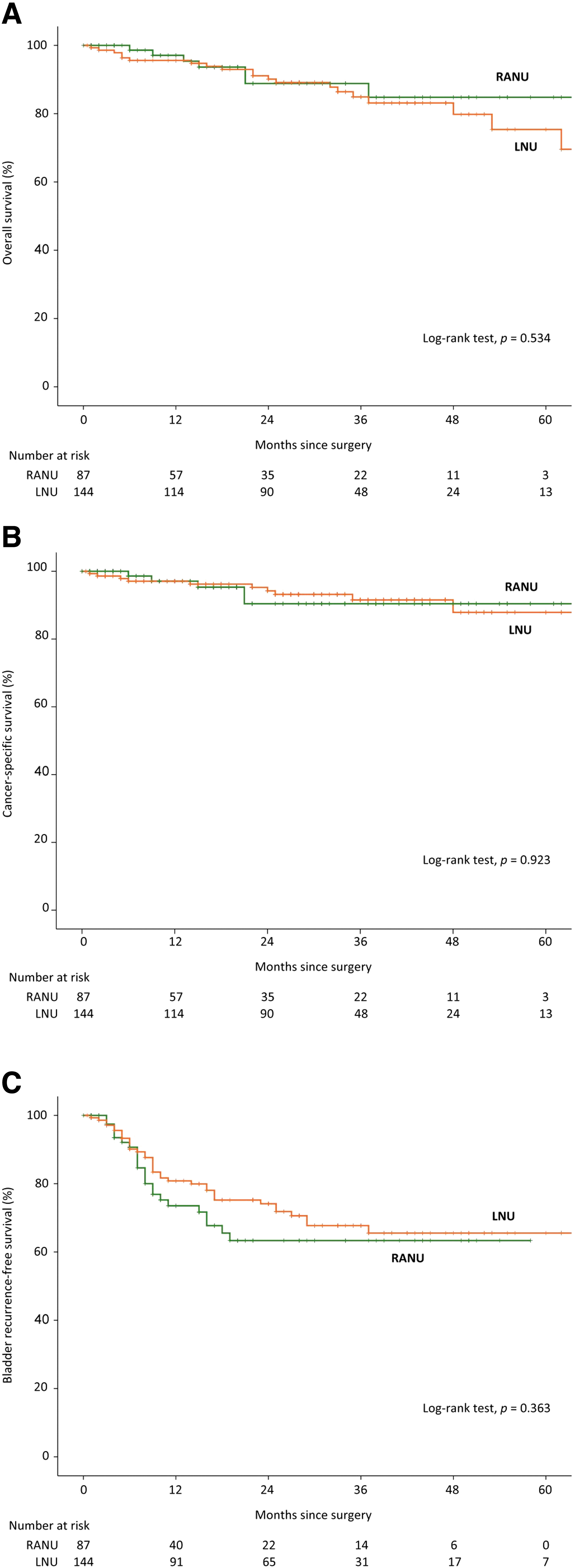
Kaplan–Meier curves of overall survival
Oncologic Outcomes in Patients Treated with Robot-Assisted Radical Nephroureterectomy or Laparoscopic Nephroureterectomy for Upper Urinary Tract Urothelial Carcinoma
Data are given as count (percentage) or median (interquartile range).
p-Values were calculated using Fisher's exact test, Mann–Whitney U test.
Log-rank test.
Discussion
Compared with open NU with BCE, LNU with BCE has become popular in the last decade for treating UTUC owing to its comparable oncologic outcomes, lower intraoperative blood loss, and better perioperative parameters. 14,15 The European Association of Urology guidelines suggest that this minimally invasive approach is an acceptable surgical alternative for treating UTUC. 16 Many laparoscopic urologic procedures such as radical prostatectomy and partial nephrectomy have been challenged by robotic platforms. However, very few studies have focused on NU with BCE, especially in terms of comparison with the laparoscopic approach. One of the reasons for this is the rarity of UTUC; this condition is not a prevalent entity in Western countries but is more common in Eastern Asia. 3,4 Therefore, we compared RANU and LNU for treating UTUC and found that the outcomes were comparable with previous reports in terms of complication rates and oncologic outcomes. 17,18 However, RANU was superior to LNU, with significantly lower intraoperative blood loss and shorter hospital stay.
Ambani et al compared RANU and LNU and reported that mean operative time (298 vs. 251 minutes, p = 0.03) and estimated blood loss (380 vs. 233 mL, p = 0.02) were significantly higher for RANU than for LNU. 12 Melquist et al compared 37 patients treated with RANU with 63 patients treated with LNU and reported that robotic approach for retroperitoneal LND with NU was associated with increased lymph node procurement and a lower risk of major bleeding but had longer operation time (5.1 vs. 3.9 hours, p < 0.001) and longer hospital stay (5.0 vs. 4.0 days, p < 0.001). 18 In our experience, there was no significant difference in the total operative time between RANU and LNU, which could be attributed to increased surgical experience.
Several techniques for distal ureterectomy and BCE have been described in previous studies, including open excision, transurethral resection of the ureteral orifice (pluck technique), ureteral intussusception, and pure laparoscopy or pure robotic approaches. 19 Each technique has its advantages and disadvantages in terms of cancer control, wound complications, and other criteria. In our series, the adoption of the approaches of BCE was primarily at surgeons' discretion. Approximately 85% of patients in the LNU group accepted open BCE; however, 100% of the patients in the RANU group accepted pure robotic approaches. Many studies have also adopted pure robotic approaches for performing distal ureterectomy and BCE. 12,17,18 It is obvious that with the dexterity provided by a robotic system, the approach method for distal ureterectomy and BCE should no longer be an issue in RANU. Furthermore, the lower intraoperative blood loss of RANU in our series may be related to the pure robotic BCE. The delicate dissection of the robotic approach in BCE may lead to less blood loss. Another possibility of the lower intraoperative blood loss in the RANU group might have resulted from different approaches of BCE between the RANU and LNU groups. In majority of the LNU group, the BCE was performed in an open manner in contrast to the pure robotic approach in the RANU group. We may speculate that the difference of blood loss was probably owing to the difference between the open versus closed BCE and not between the robotic versus laparoscopic approach.
The transition from the upper urinary tract to the lower urinary tract after completion of NU is a frequently discussed issue in robotic approaches. Several docking and positioning methods have been proposed in the Si system. For example, Ambani et al placed their patients' upper body in a flank position and lower body in a lithotomy position. They performed renal and proximal ureteral dissection with the table rotated around the vertical axis at a 45° angle and the robot positioned on the patient's ipsilateral side. When they performed distal ureteral dissection and BCE, they undocked the robot and rotated the table back to the neutral position. Then, the robot was repositioned between the patient's legs and re-docked. 12 Melquist et al proposed a single-docking approach using a Si system. They positioned the robot over the patients' hip at a 45° angle, facing the contralateral shoulder and did not need to switch the robotic arms to complete the NU and BCE during operation. 18 In our Si series, patients were placed in the lateral flank position, and the robot was positioned over the tumor's ipsilateral side to face the contralateral hip when performing renal and proximal ureteral dissection. We re-docked the robot facing the contralateral shoulder to perform distal ureterectomy and BCE. However, for the Xi system, re-docking was not necessary, with only retargeting needed while transitioning from NU to BCE.
When using the Xi platform, the robot was docked perpendicular to the patient, who was in the flank position, from behind the ipsilateral side. Ports were then placed linearly along the lateral border of the rectus muscle. Patel et al proposed performing NU and BCE on the Xi platform with single docking and single robotic port placement, which was similar to our approach. 20 In addition, Patel et al compared perioperative outcomes between the older da Vinci Standard/S/Si platform and the newer Xi robotic platform during NU. The total operative time was shorter in the newer Xi system than in the older da Vinci Standard/S/Si platform (184.4 vs. 232.09 minutes, p = 0.0035). 21 In our patients in the RANU group, both total operative time and console time were slightly shorter in the Xi system than in the Si system (275.5 vs. 308.9 minutes, p = 0.919; 192.1 vs. 210.8 minutes, respectively, p = 0.476), but this difference was not statistically significant.
One strength of our study was the relatively large sample size and the single-center cohort design. There were fewer confounding factors in the single-center cohort than in the multicenter cohort. However, this study also has several limitations. First, two different generations of the da Vinci surgical system were adopted, which could cause technical variations in some details. Nevertheless, 79 of the 87 patients in the RANU group were operated with the Si system, which represented a significant portion of the robotic series. Second, only 14.6% of patients in the LNU group underwent pure laparoscopic BCE, but 100% in RANU group underwent intracorporeal BCE. The comparison was not totally equivalent from the perspective of the BCE technique. However, such practice reflected our actual clinical practice pattern. Furthermore, our laparoscopic and robotic approaches in the management of BCE may reflect the changing trend of the technique. Third, although a lower intraoperative blood loss was observed in RANU, we did not divide the amount of bleeding into NU part and BCE part. However, we may speculate that the delicate dissection offered by the robot in BCE may lead to less blood loss. In addition, the more adoption of closed BCE in the RANU group is another possibility that resulted in lower blood loss. Fourth, the follow-up duration of patients in the LNU group was longer than that of patients in the RANU group owing to the later adoption of this newer technology. Despite this difference in the follow-up duration, no significant oncologic differences were observed. Finally, our cases analyzed were very heterogeneous: difference in the indications of procedure, different surgical techniques, difference in follow-up time, and so on. Considering the potential biases, the interpretation of the results must be very cautious.
In conclusion, from our experience in a UTUC-prevalent region, RANU and LNU had comparable perioperative and oncologic outcomes. RANU was superior to LNU in terms of intraoperative blood loss and hospital stay. However, considering the potential biases owing to the heterogeneity of our cases, the interpretation of the results must be very cautious. Nevertheless, to perform NU with BCE in a more costly way with robotics, we truly saw some advantages.
Footnotes
Authors' Contributions
Y.P.H.: data collection and management, data analysis, article writing. E.Y.H.H.: project development, data collection and management, data analysis, article editing. H.J.C.: data collection. M.C.T.: data collection and management, data analysis. T.H.H.: data collection. T.C.W.: data collection. Y.H.F.: data collection. C.C.L.: data collection. T.P.L.: data collection. J.Y.K.: data collection. S.H.L.: data collection. Y.H.C.: data collection. A.T.L.L.: data collection. W.J.S.H.: data collection.
Availability of Data and Material
The datasets analyzed during this study are available from the corresponding author on reasonable request.
Ethics Approval
The study was ethically approved by the Institutional Review Board (2020-12-007BC).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
Patients signed informed consent regarding publishing their data and photographs.
Author Disclosure Statement
The authors declare that they have no conflicts of interest related to the subject matter or materials discussed in this article.
Funding Information
This work was supported in part by the Ministry of Science and Technology, Taiwan [MOST 104-2314-B-075-079] and Taipei Veterans General Hospital, Taiwan [V109C-176, V109EP-014, V110C-164, 110EP-009].
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.