
Abstract
Introduction:
It is acknowledged that the COVID-19 pandemic has had a major impact on health care services around the globe with possible worse outcomes. It has resulted in stretch of resources with canceled or delayed procedures. Patients with urinary calculi have also suffered the negative impact. This systematic review aims to assess the impact of the early COVID-19 pandemic on the presentation and management of urinary calculi around the globe.
Methods:
We reviewed the impact of early COVID-19 on the clinically important aspects of stone disease using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology. We searched Medline, Embase, and Central databases using themes of COVID-19 OR Sars-Cov-2 OR pandemic OR coronavirus AND kidney stone, urinary calculi, urolithiasis, and similar allied terms. Inclusion criteria were studies with data on both pre- and COVID-19 period covering one or more of eight clinical domains.
Results:
Our search returned 231 studies, after removal of duplicates, of which 18 studies were included for analysis. The number of patients presenting to hospital declined by 21%–70% at the beginning of the pandemic, whereas majority of studies reported increased associated complications. There are mixed reports in terms of delay to presentation and use of conservative management. There was a consistent trend toward reduction in elective procedures with wide variations (shockwave lithotripsy 38%–98%, percutaneous nephrolithotomy 94%–100%, and ureteroscopy 8%–98%). There was a trend toward increased nephrostomy insertion with the onset of the pandemic.
Conclusion:
This review demonstrated the differences in the number of patients presenting to hospital, complication rates, and management of urinary calculi, including surgical interventions, with the onset of the COVID-19 pandemic. It offers baseline global information that would help understand the impact of early pandemic, variations in practices, and be useful for future comparisons.
Introduction
The severe acute respiratory syndrome-Cov-2 pandemic began >2 years ago. It is widely acknowledged that the COVID-19 pandemic has had a major impact on health care services around the globe. Many hospitals have seen a decline in patient admissions with some only functioning at a 50% capacity during the first wave. 1 Some of the findings of a study suggested that decreased hospital admissions were because of fear of patients contracting COVID-19 and some patients having a certain stigma toward infected patients. 2 The pandemic has also led to large volumes of scheduled treatments to be postponed to allow beds and staff to be available for patients seriously ill with COVID-19. 3
A multicenter study concluded that there was an increase in average surgery waiting time from 85.8 to 92.6 days in 2020, which led to an average 8% increase in waiting times. 4 The delay of being seen by a health care worker caused by patient anxiety, government regulation, and postponement of treatment may suggest higher complication rates during the pandemic. The urology department has also seen changes to the services, particularly pertaining to the cases of urinary calculi, as a result of the COVID-19 pandemic.
Urinary calculi, or urolithiasis, is a common condition that is found in 1 of 12 patients (8%) who have a CT scan performed. 5 It has been reported that 12% of males and 6% of females will get urinary calculi. 6 Associated complications include urinary tract infection, sepsis, renal tract obstruction, hydronephrosis, acute kidney injury (AKI), and urinoma. Over the years there have been advancements in the treatments of urinary calculi, which include percutaneous nephrolithotomy (PCNL), ureteroscopy (URS) and laser lithotripsy, and extracorporeal shockwave lithotripsy (SWL). Stones can also be managed conservatively along with medical expulsive therapy where the stone is monitored and in many cases the stone can be passed spontaneously. 7
It has been reported that procedures related to urolithiasis have been postponed during the pandemic because of the fear of acquiring COVID-19. 8 A study showed that 10% of patients had asked to postpone procedures such as URS and PCNL. 9 An average decrease of emergency department (ED) attendance of 35% was reported, whereas another study showed a 40% decline during the first wave. 10,11 Patients who avoid seeking treatment from hospitals may potentially lead to their symptoms or disease becoming more severe with the resultant increased risk of complications.
The journey of a patient with urinary calculi involves different steps. It is likely that many of the steps might have been affected to different extent. Assessment of the impact of the pandemic would give a better understanding from the point of view of different stakeholders that would also be useful for the future.
This systematic review aimed to assess the impact of the early COVID-19 pandemic on the presentation and management of the urinary calculi around the globe.
Methods
The systematic review was performed as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A systematic search was carried out on databases Medline, EMBASE, and CENTRAL. The following search terms were utilized: (COVID-19 OR Sars-Cov-2 OR pandemic OR coronavirus) AND (kidney stone OR urinary calculi OR urolithiasis OR urinary stone OR nephrolithiasis OR ureteral stone OR renal calculi OR renal stone OR ureteral calculi OR renal colic).
All studies comparing the presentation or management of urinary calculi before and during the pandemic. Exclusion criteria included conference abstracts, letters to editors, and studies where the impact of coronavirus pandemic is not assessed and any studies where urinary calculi is not evaluated.
Two reviewers (N.S. and D.N.K.) independently screened titles, abstracts, and analyzed full texts after retrieval of studies from the search, after removal of duplicates. Any unclear studies were screened by mutual agreement. Reasons for exclusion were noted. Data extracted included the study characteristics, design, aim of study, patient characteristics, number presenting to hospital, and number of patients admitted. The main outcomes evaluated were stone size, stone location, time from onset of symptoms to presentation, associated complications, and type of management. A meta-analysis was not performed because of the heterogeneity of the studies and their outcomes.
The risk of bias was assessed using The Nottingham Ottawa scale risk of bias tool for the observational tool, where studies were deemed as good, fair, or poor quality. 12
Results
A total of 299 records were identified from the systematic search, the results of which are summarized in Figure 1. After removal of duplicates, 231 studies were screened by title and abstract resulting in 30 studies for full text analysis. Of these, a total of 18 studies were included in the final analysis. These spanned 16 countries and 6 were multicenter studies (Table 1). Eight studies were excluded as no comparison was made between the pre-COVID-19 and COVID-19 era, whereas a further four were excluded as the presentation and management of urinary calculi was not evaluated.
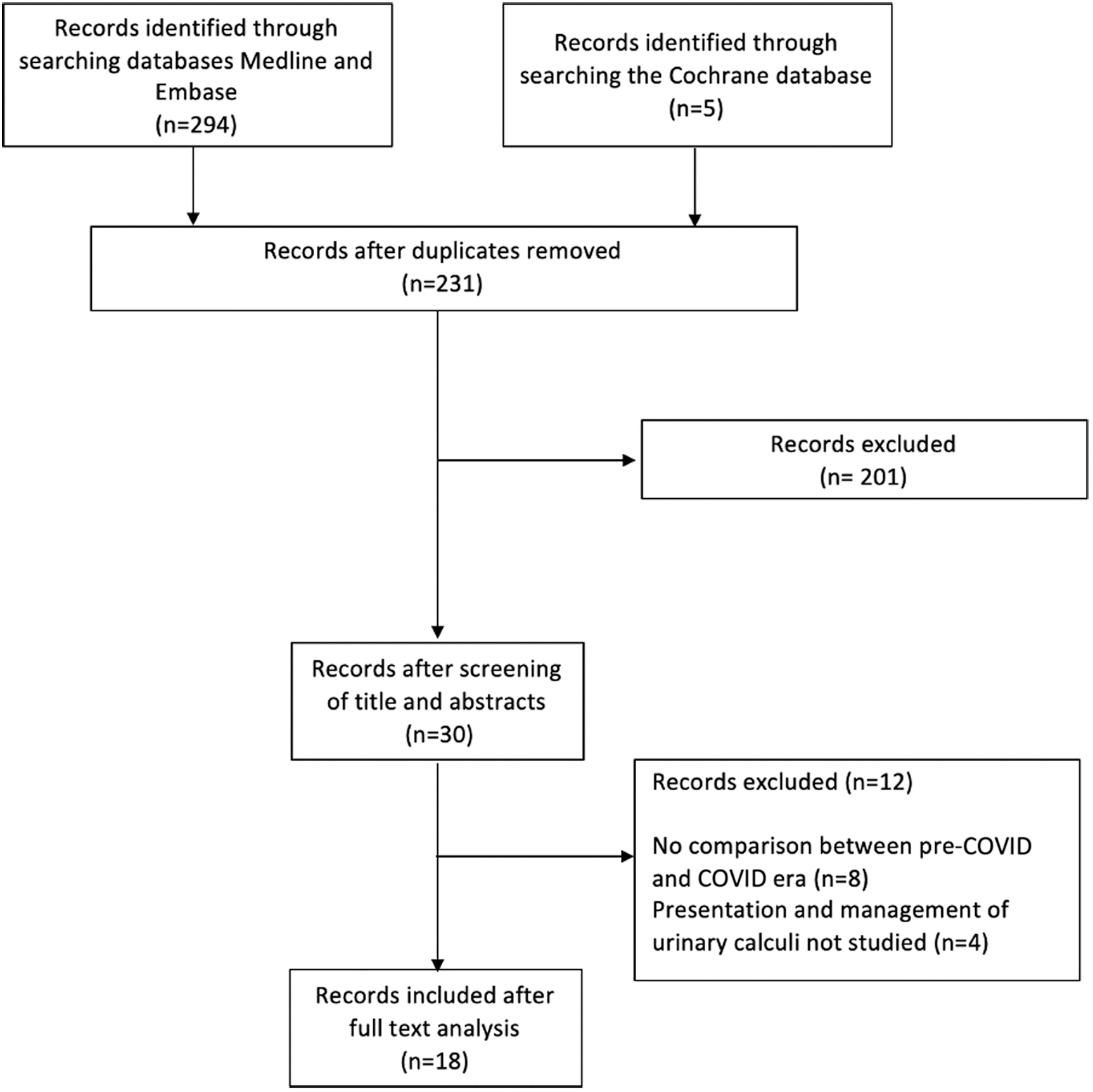
PRISMA flowchart. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Included Studies
ED = emergency department; KUB = kidney, ureter, and bladder radiograph; SARS = severe acute respiratory syndrome.
Thirteen studies in total evaluated presentation and admissions to hospitals and five explored associated complications. There were six articles that looked at stone size, whereas five considered stone location. Four studies looked at onset of symptoms to presentation, six on conservative management, three on emergency surgical intervention, and four studies on URS, PCNL, and SWL, respectively.
Presentations/admissions
Ten studies found a decrease in the number of patients presenting with urolithiasis, ranging from 21% to 70%. 13 –22 Three of these studies, although reporting reductions in number of patients presenting to hospital, found a similar proportion (11.9% pre-COVID-19 vs 10.7% during COVID-19) 14 or an increased proportion (18.1% and 20.9% pre-COVID-19 vs 34.6% and 38.8% during COVID-19, respectively) 13,15 of those presenting to hospital being admitted.
Three studies found a similar number of patients presenting before COVID-19 and during a period in the pandemic. One study found 343 patients to a urologic ED in a period in 2019, whereas 376 presented during the same period in the pandemic. 23 Another study found similar numbers presenting with urolithiasis in the 100 days before and after the start of the pandemic. 24
Stone size
Four studies suggested increases in the size of stones. One of these studies reported kidney stone size increased from 5.1 mm prepandemic to 10.5 mm during the pandemic based on patient self-reported posts on social media platforms. 19 One study reported similar sizes of 11 mm prepandemic and 13 mm during the pandemic, in patients undergoing retrograde intrarenal surgery (RIRS). However, in those undergoing PCNL, stone size decreased from 23 to 16 mm during the pandemic. 25 Whereas the other two studies reported smaller increases of 5.3–5.4 mm and 6.13–6.48 mm pre- and during COVID-19, respectively. 18,23 One study reported a greater proportion of patients (63.2%) presenting with small stones <5 mm during the COVID-19 era compared with 44.7% prepandemic in the same duration of time. 14 Similarly, another study reported mean stone size of 4 mm during COVID-19 compared with 4.7 mm pre-COVID-19. 24
Stone location
Four studies found a trend of a higher proportion of distal ureteral stones during the pandemic. 14,18,23,24 One study observed 23% of patients undergoing RIRS and PCNL had accompanying ureteral stones in the COVID-19 period compared with 10.8% in the prepandemic period. 25
Associated complications
Two studies report higher general complication rates in the during COVID-19 period of 20.4% and 21.8% compared with 10.9% and 5.6% in the prepandemic period. 13,15
With regard to hydronephrosis, one study found that in patients undergoing PCNL and RIRS, a significantly higher proportion of patients did not have hydronephrosis during the prepandemic period when compared with the pandemic period (47.3% vs 23%; p = 0.01). 25 However, among those with hydronephrosis during the pandemic period, a higher proportion had mild hydronephrosis. Another two studies also found a similar trend toward a greater proportion having hydronephrosis in the pandemic period. 14,18
In terms of associated fever, two studies reported mixed results with one suggesting slightly increased proportion of those with fever in the COVID-19 period (13.6%) compared with pre-COVID-19 period (6.9%). 13 However, another study suggested increased numbers having associated fever in the prepandemic period (10.2% pre-COVID-19 vs 7.1% during COVID-19). 14
Two studies report higher rates of urinoma during the COVID-19 period, whereas one study reports a higher rate of AKI during the COVID-19 period. 14,15
Onset of symptoms to presentation
One study reported the mean delay in terms of onset of symptoms to the day of visit to the hospital was 4.1 days in COVID-19 era and 2.9 in the pre-COVID-19 period. 15 A second study reported 29 out of 35 patients felt they were late in receiving treatment. Sixty-two percent of these felt this was caused by fear of contracting COVID-19, whereas 21% said travel and isolation restrictions contributed to this. 18 However, in another study, from 34 patients, the median duration of pain before hospital presentation was 1 day in the COVID-19 period compared with 2 days pre-COVID-19. 24 Another study reported mean onset time for symptoms of 6.5 hours prepandemic and 5.4 hours during the COVID-19 period. 23
Conservative management
Four studies found an increased proportion offered conservative measures. One of these reported 86.1% and 81.6% in two periods in the pandemic era compared with 74.8% and 73.9% in two non-COVID-19 periods. 23 Another study found a statistically significant increase in conservative management in the COVID-19 period (55.3% vs 28.5%, p = 0.0001). 18 One found a similar trend with an increase from 12.5% to 26% in the COVID-19 period based on online social media posts from patients. 19 However, two studies found a decrease in the proportion managed conservatively reporting a trend of 81.9% and 54.1% in the pre-COVID-19 era compared with 66.7% and 45.5% during COVID-19, respectively. 14,15
Emergency surgical intervention
One study found a trend toward an increase in proportion stented with 12.8% in the COVID-19 period and 7.5% pre-COVID-19. 15 Whereas the other two studies found a lower proportion stented with 34.3% and 6.3% during COVID-19 compared with 43.9% and 8.8% pre-COVID-19. 14,18 With regard to nephrostomies, all three studies found a trend toward an increase in proportion nephrostomies during COVID-19 (3.85%, 1.8%, and 37.2% vs 3.13%, 1.1%, and 0.9%, respectively). 14,15,18 Another study found a 45.1% and 58.2% reduction in stenting and nephrostomy insertion, respectively.
However, this may include intervention for nonstone-related disease as well. 26 Two studies compared emergency lithotripsy and URS for stone patients presenting to ED. One found a trend toward a higher proportion undergoing emergency lithotripsy (16.67%) during COVID-19 compared with pre-COVID-19 (7.5%), 15 whereas the other found a slight reduction in those undergoing urgent URS (1.8% from 2.5% during COVID-19). 14 Anderson and colleagues found 30.4% undergoing radiologic/surgical intervention during COVID-19 and 31.8% pre-COVID-19. 24
URS, PCNL, and SWL
Two studies found a 38.5% and 98.5% reduction in SWL during COVID-19 period. 27,28 Another study reported 1.5% and 3.3% of stone patients presenting to the ED during two periods in the pandemic undergoing SWL, compared with 8% and 10% before COVID-19 in two periods before COVID-19. 23
With regard to PCNL, two studies quoted 94% and 100% reduction during the period in the pandemic. 26,27 Another study found only seven patients undergoing PCNL in a 6-month period within the pandemic compared with 23 in 6-month period before the pandemic. 25
Two studies reported 78% and 98.2% reduction in URS procedures during a period in the pandemic. 26,27 As did another study that reported a trend toward a lower proportion undergoing URS with 12.4% and 15.1% within two periods in the pandemic compared with 19.0% and 16.1% in two periods before COVID-19. 23 Finally, one study found a reduction in all procedures for nephrolithiasis from 126 procedures pre-COVID-19 to 83 in the same period during COVID-19. 29
Assessment of risk of bias
The Nottingham Ottawa scale was used to assess the risk of bias for each study. The assessment is summarized in Table 2. The assessment consisted of three different sections involving selection, comparability, and outcome. The studies were then categorized into good, fair, and poor quality based on the number of stars allocated in each section. Good quality articles had 3 or 4 stars in the selection domain, 1 or 2 stars in the comparability domain, and 2 or 3 stars in the outcome domain. Fair quality articles had 2 stars in the selection domain and 1 or 2 stars in the comparability domain and 2 or 3 stars in the outcome domain.
Risk of Bias Scores—Nottingham Ottawa Scale
Poor quality articles had 0 or 1 stars in the selection domain or 0 stars in the comparability domain and 0 or 1 stars in the outcome domain. A total of 12 articles had 4 stars allocated to its selection domain, 13 –15,17,21,23 –28,30 5 articles had 3 stars allocated, 16,18,20,22,29 and 1 article had only 1 star. 19 With regard to the comparability domain all 18 articles had only 1 star allocated. In the outcome domain 16 articles had 2 stars, 13 –18,21 –30 whereas 2 articles had only 1 star. 19,20 Overall, based on the categorization 16 articles are considered good quality, 12 –18,21 –30 and 2 articles are of poor quality. 17,29
Discussion
This systematic review aimed to assess the impact of the early COVID-19 pandemic on the presentation and management of urinary calculi. The study found that there was a negative impact in the presentation and management of urinary calculi across the globe. The impact across different aspects of presentation was variable and guided management accordingly, across different parts of the globe.
The number of patients presenting to hospital with urolithiasis generally declined with the onset of the pandemic. This was in keeping with what was observed in the United Kingdom where total number of attendances to EDs decreased over 2020–2021 as compared with the previous years. 31 A study in Iran showed a similar trend in the number of visits to the clinic by kidney stone patients with a decrease from 1625 before COVID-19 to 672 during COVID-19. 32 In a study at a major center, patients attending ED fell by 37% and another in Portugal reported a drop of 46.4% of patients visiting the urology ED. 33,34 This could be attributed to fear of contracting COVID-19 in hospitals. Furthermore, the pandemic saw an increase in the use of digital services. 35 It is possible that there was increased use of telephone consultations and digital services, which in effect lead to decreased visits to ED. In Italy, a study showed 45% of patients canceled their appointment, whereas 56% of the remaining patients underwent a telephone consultation. 36
Although the number of patients presenting to hospital decreased, some studies reported an increased proportion of patients requiring admissions. This could be explained by increased levels of associated complications, such as hydronephrosis, AKI, and urinoma, which some studies highlighted. It is possible this is again because of delayed presentation to hospital because of fear of COVID-19 transmission. Although there was decreased numbers presenting to hospital, there was mixed evidence in the literature with regard to the pandemic leading to delayed presentation.
On top of the fear of COVID-19, government-imposed travel restrictions and isolation rules may have contributed to delays to presentation as noted by some studies. However, the nature of renal colic and its associated severe pain that would prompt most patients to seek medical attention, which could explain why significant delays were not observed in all studies. There have been many factors that could have resulted in these changes. These include ease of access to the medical facilities, for investigations as well as management, the type of health care systems, and segregation protocols.
Potential delays to presentation could have an impact on associated complications. Although the majority of studies reported higher complication rates, there were still mixed results with regard to the impact of COVID-19 on associated complication rates. A few studies found increased rate of associated hydronephrosis during the pandemic period, whereas one study found cases were milder during the pandemic. Sepsis is a life-threatening complication that can be associated with urinary stones. One systematic review found that sepsis was the leading cause of mortality rate in patients with kidney stone disease. 37
However, the studies in our review once again highlighted mixed results with overall no major differences in rates of associated fevers or sepsis with the onset of COVID-19. This could be related to different factors. Patients with relatively complicated disease may be seeking medical help irrespective of the COVID-19 situation. Similarly, it might indicate selective and careful attention to this group of patients even during the pandemic across the globe in general. Data from subsequent phases of the COVID-19 waves would be helpful to cast more light on these issues.
Looking at the relation between stone size at presentation before and during the early pandemic, the results are variable. This probably indicates that the stone size alone might not influence the decision to seek advice or presentation to the hospital. It is the associated symptoms such as intensity of pain and possible sepsis that would influence this decision. Similarly, a higher proportion of patients presenting with distal ureteral stones might indicate increased propensity to present late when the symptoms might become more pronounced. Late presentation or delayed treatment might explain the findings of increased incidence of hydronephrosis, during pandemic, in patients undergoing PCNL or URS. Onset of symptoms to the presentation at the hospital was delayed during the pandemic, in many series, as expected.
Looking at the patterns of management of the stones, there was mixed results. Although two studies showed a decrease in proportion of patients managed conservatively, the majority of studies found an increased trend toward conservative management, in the hope of avoiding hospitalization and risk of COVID-19 complications.
Regarding emergency interventions to drain the kidney, some studies reported a trend toward increased rate of nephrostomy insertion for urolithiasis. Higher use of nephrostomy insertion suggests increased complicated stone disease as mentioned previously. However, a decrease in the number of stent insertions and urgent URS was also noted in some studies. Nephrostomy insertion, performed under local anesthesia, avoided the risk of general anesthesia and associated risks of COVID-19 transmission. It is unclear, in patients with indwelling ureteral stents, if there were delays in their subsequent definitive management of the stones and increased stent dwell time and stent-related symptoms and complications. However, few centers took a different approach regarding urgent stone management and focused on urgent invasive treatments of the stones to minimize further stone-related complications or the need for multiple hospital visits.
Furthermore, there was a reduction in the number of elective procedures such as URS, SWL, and PCNL. In one study, several hospitals in five different countries adapted to performing more nephrostomy and stent insertion and decreased PCNL and URS after 21 days from their first COVID-19 case. 38 Furthermore, a systematic review on guidelines for urologic practice in the COVID-19 pandemic found while obstructed or infected stones should be decompressed, management of nonobstructing renal or ureteral stones could be delayed. 39
The significant rise in hospital COVID-19 admissions and ICU beds meant the need to prioritize and reallocate resources to meet the demands. 40 In England and Wales, there was a 33.6% reduction in surgical activity in 2020 as a result of increased cancellations and reduced number of surgical procedures being carried out. 41 These issues will have implications for planning and allocation of the resources to clear the backlog of more elective treatments. The impact of this at the patient and societal level is unclear.
It is important to note there is variation in the management strategies between studies. This may be as a result of differences in practice between the various centers included in this review as the centers span different geographical areas. It could also be related to the differences in the patient demographics, resources available, and the infrastructure.
This systematic review has its limitations. Although care was taken to include all relevant studies, records may have been missed. Furthermore, all studies were evaluating early periods of the COVID-19 pandemic in 2020. Since then, there have been several phases within the pandemic with the emergence of new variants as well as geographical variations in case numbers and government restrictions.
The results of this review show the impact of the pandemic, and the patterns of management of stone disease, during the early phase of the pandemic. Further studies assessing the presentation and management of urolithiasis in more recent times would be useful in evaluating if there have been any further changes to the observed differences seen early on. These would be useful for the development of health care systems and future protocols to aid prompt management of patients with renal stones. The results would indicate the need to develop the strategies for better coordination and consistent approach to manage the renal stone disease. Similarly, this will continue to provide the opportunity to develop reliable systems for remote assessments and triage protocols. All of this would help risks of disease transmission as well as fears among the patients as well as the staff. This will help reduce unnecessary variations in the practice.
Conclusion
This systematic review has highlighted the impact of COVID-19 pandemic on urolithiasis. When compared with prepandemic periods, the onset of the pandemic has brought differences in the number of patients presenting to hospital, being admitted, complication rates as well as the management of urinary calculi, including surgical interventions. Although these effects were seen early on in the pandemic, the evolving nature of health care services response to the pandemic means further studies evaluating the current landscape of urolithiasis presentation and management are required.
Footnotes
Authors' Contributions
Conceptualization, database search, study selection, data extraction and analysis, writing (lead) initial draft of article and revisions by N.S. Database search, study selection, extraction and analysis, writing initial draft of article, and revisions by D.N.K. Conceptualization, design, and revisions of article by H.J.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.