
Abstract
Introduction:
It is challenging to diagnose diabetic renal papillary necrosis (RPN) radiologically due to the limitation in performing a contrast study in patients with compromised renal function. Endoscopic management by Double ‘J’ (DJ) stenting or percutaneous nephrostomy is the preferred treatment. The aim of our study was to analyze the role of retrograde intrarenal surgery (RIRS) in the management of RPN by retrieving necrosed papillae.
Methods:
This retrospective study included diabetic patients who presented with acute pyelonephritis or urosepsis at our institute. After evaluating with appropriate laboratory and radiological investigations, retrograde pyelography (RGP) and DJ stenting were performed in those who did not respond to intravenous antibiotic therapy. The RIRS was performed in patients who had filling defects in the pelvicaliceal system (PCS) on RGP after 3 weeks at the time of DJ stent removal. Patients with a minimum follow-up period of 6 months were included.
Results:
A total of 187 patients (81 female, 106 male) with diabetes with a mean age of 58.3 years were enrolled in this study. The mean serum creatinine was 2.7 mg/dL and mean estimated glomerular filtration rate was 32.8 mL/min/1.73 m2. One hundred twenty-six patients (67.3%) had hydroureteronephrosis (HUN), out of whom 74 (58.7%) had necrosed papillae in the PCS. In 61 (32.6%) patients, there was no HUN; however, 25 (41%) of these patients had necrosed papillae in PCS. Necrosed renal papillae were retrieved in 83 patients (46.1%) by RIRS. All the patients were followed up for a minimum period of 6 months; seven patients (3.8%) had recurrent pyelonephritis.
Conclusions:
The RIRS plays a significant role in the management of diabetic RPN. Retrieving necrosed papillae from the PCS after confirming their presence by RGP prevents ureteric obstruction, which leads to urosepsis, and presumptively prevents or delays future episodes of pyelonephritis.
Introduction
Diabetes mellitus (DM) is a chronic metabolic noncommunicable disease that has attained epidemic proportions globally. 1,2 Urinary tract infections (UTIs) are common in patients with diabetes, which further complicate to acute pyelonephritis, emphysematous pyelonephritis, and eventually renal abscess. A Danish study reported that patients with DM are three times more likely to be hospitalized with pyelonephritis than those without DM. 3
There has been an alarming increase in the number of patients with acute pyelonephritis and urosepsis with or without obstructive uropathy. Renal papillary necrosis (RPN) is a common cause of obstructive uropathy in patients with DM presenting with acute pyelonephritis. The etiology of RPN includes DM, analgesic abuse or overuse, sickle cell disease, pyelonephritis, renal vein thrombosis, tuberculosis, and obstructive uropathy. 4
The RPN is not a pathologic entity but is a descriptive term for “necrosis of the renal papillae,” which has various possible causes. The renal medulla and papillae are vulnerable to ischemic necrosis because of the peculiar arrangement of their blood supply and the hypertonic environment. 4 The RPN is a challenging entity to diagnose because ultrasound examination is not very sensitive, and contrast-based investigations such as contrast-enhanced CT and intravenous urography are often required. 5
However, there is a risk of diabetic nephropathy and a steady decline in the glomerular filtration rate (GFR) due to the use of contrast-based radiological procedures, leaving ureteroscopy as the only definitive modality in this group of patients. 5
The treatment of patients who present with signs of acute pyelonephritis or urosepsis and ureteric obstruction by endoscopic Double-J (DJ) stent placement to tide over the crisis of sepsis is a well-accepted modality. Once the patient improves symptomatically, routine practice is to remove the DJS and extract the papillae by cystoscopy and/or ureteroscopy, which results in a dramatic recovery. 4 However, there is no available literature on the role of retrograde intrarenal surgery (RIRS) in the management of RPN.
The aim of our study was to analyze the role of RIRS in the management of diabetic RPN by the retrieval of necrotic papillae from the pelvicaliceal system (PCS), confirmed by retrograde pyelography (RGP), after the patient recovers from the acute phase of pyelonephritis.
Materials and Methods
This study is a retrospective analysis of a prospectively maintained database of patients with diabetes who presented with acute pyelonephritis and urosepsis and eventually underwent RIRS for the retrieval of necrotic renal papillae between July 2016 and December 2020. Approval was obtained from the scientific committee and institutional review board. Informed consent was obtained from all the patients before the intervention.
Inclusion criteria
This study included patients with DM who presented with features of acute pyelonephritis (fever, chills, loin pain, and flank tenderness) and/or urosepsis. Patients who did not respond to conservative management and required RGP and DJS were included in the study.
Exclusion criteria
Patients with ureteric and renal stones, ureteric strictures, ureteric obstruction due to extrinsic compression, malignancies, or nondiabetic pyelonephritis; those with a history of analgesic abuse, sickle cell disease, chronic liver disease, or tuberculosis; those who underwent urinary diversion with percutaneous nephrostomy for hydronephrosis; and those who responded to the initial conservative management were excluded from the study.
Initial assessment and management
The patient's clinical data and laboratory investigations, including complete blood count, renal function tests, serum electrolytes, blood glucose levels, urine examination, and urine culture (Mid stream sample), were recorded. Radiological investigations, such as ultrasonography of the whole abdomen and noncontrast CT (NCCT) of the kidney, ureter, and bladder radiograph region, were analyzed for acute pyelonephritis and hydroureteronephrosis (HUN). The NCCT was preferred because most patients had an elevated serum creatinine level due to pyelonephritis with sepsis. The patients were treated with intravenous antibiotics, antipyretics, and analgesics, and they had adequate glycemic control.
Third-generation cephalosporin (cefoperazone) in combination with a beta-lactam inhibitor (sulbactum) were preferred according to the institute's antibiogram. Antibiotics were changed according to the urine culture report and the patient's clinical response. The urine culture sample collected was a midstream urine sample. The RGP with DJS placement was performed if the patient was not responsive to conservative management.
The presence or absence of HUN was not a determining factor for DJ stent placement. The RGP was performed by using a 5F ureteric catheter placed 2 to 3 cm beyond the ureteric orifice to delineate the PCS, after which a DJ stent was placed. The respective findings for RGP were recorded. The patients were reassessed for clinical improvement with antibiotics and laboratory monitoring. Renal replacement therapy was performed in the form of hemodialysis. Ultrasound of the whole abdomen was performed to identify renal abscess, and perinephric fluid collection was done after 1 week of follow-up.
RIRS procedure
All patients with filling defects in PCS on RGP, at the time of DJS removal after 3 weeks, underwent RIRS after repeating the urine culture and under appropriate antibiotic cover. All patients underwent laboratory tests, including complete blood tests, renal function tests, and blood glucose level assessment. Whole-abdomen ultrasound was performed to identify renal abscesses, and the perinephric fluid collection was done. Appropriate intravenous antibiotics were administered 1 hour before the procedure. The patients underwent RIRS under general anesthesia. After removal of the DJ stent, RGP was performed.
Patients with filling defects on RGP underwent an initial ureteroscopic assessment by using a semi-rigid ureteroscope (8F) to identify and retrieve necrotic papillae in the ureter. In patients with filling defects noted in the PCS not accessible by semi-rigid ureteroscopy, a ureteral access sheath (9F/11F) was placed, and a flexible ureteroscope was used to inspect the PCS for necrosed papillae. After the necrosed papillae were identified, they were retrieved by using a basket and submitted for histopathological examination and assessment for fungal elements.
In patients with large necrosed papillae, a percutaneous nephrostomy was performed for retrieval. Patients who underwent percutaneous nephrostomy for the retrieval of necrosed papillae were not excluded from this study. Necrosed papillae that were adherent to the calix were not retrieved. Ureteric and urethral catheters were placed when deemed necessary. The perioperative parameters and complications were also recorded. The patients were monitored during the postoperative period for fever, hypotension, and hypoglycemia for 24 to 48 hours. The patients were discharged with appropriate antibiotics.
Follow-up
Data of patients who underwent RIRS at the time of DJ stent removal after 3 weeks were assessed. The number of patients with necrosed papillae in the PCS, along with a sub-category of patients with or without HUN, was also analyzed. Patients with a minimum follow-up of 6 months after RIRS were included in the study.
Statistical analysis
The clinical data are presented as mean ± standard deviation, and correlation was performed by analysis of variance (ANOVA). Categorical data are presented as percentages. A chi-square (χ 2 ) test was used to compare categorical variables in the study groups (male vs female). A comparison of groups with and without hydronephrosis was performed by using ANOVA (continuous variables) and χ 2 test (categorical variables). Outcomes after urinary diversion and flexible ureteroscopy (fURS) were determined by one-way ANOVA (Tukey post hoc analysis), and all statistical analyses were two-sided, with significance set at p < 0.05. All calculations were performed by using IBM SPSS Statistics version 27 (IBM, Armonk, NY).
Results
A total of 187 diabetic patients with pyelonephritis and/or urosepsis were enrolled in this study. All patients were initially treated conservatively according to the institutional protocol, and those who either did not respond or were worsening clinically within the next 48 hours were considered for RGP and DJ stent placement. All patients were then taken up for RIRS after 3 weeks. The clinical and investigative characteristics of the patients are outlined in Table 1. Of the 187 patients analyzed, 81 (43.3%) were female and 106 (56.7%) were male, with a mean age of 59 ± 10 years.
Patient Demographic Data
Data presented as mean ± standard deviation.
Data within the groups were corelated by chi-squared (χ 2 ) test for homogeneity of variance.
Data presented as n (%).
Data denote statistical significance (<0.05) when comparing means using ANOVA.
eGFR—eGFR rate calculated by chronic kidney disease Epidemiology Collaboration (CKD-EPI) formula
ANOVA, analysis of variance; eGFR, estimated glomerular filtration rate.
The mean serum creatinine value was 2.7 mg/dL, and the mean estimated GFR (eGFR) was 32.8 mL/min/1.73 m2. The mean glycosylated hemoglobin (HbA1c) was 8.8% ± 1.5% in males and 8.4% ± 1.2% in females. A total of 167 patients (89.3%) were already in stage 3 or beyond of chronic kidney disease. Moreover, 136 (72.7%) patients had a positive urine culture, and the most common organism found was Escherichia coli (in 52 patients and more common in females; Table 2). The radiological characteristics and data of retrieval of necrosed papillae after fURS are shown in Table 3.
Urine Culture and Isolated Organisms in the Study Cohort
Fifty-one (27.3%) had sterile urine cultures in the study cohort.
Data presented as n (%).
Data within the groups were corelated by chi-squared (χ 2 ) test with a statistical significance of <0.05.
Radiological Characteristics and Identification of Necrosed Papillae on Retrograde Intrarenal Surgery
Data presented as n (%).
Denotes statistical significance (<0.05) when comparing groups by chi-squared (χ 2 ) test.
Data presented as mean ± standard deviation.
Denotes statistical significance (<0.05) when comparing means using ANOVA.
A total of 126 (67.4%) patients had hydrouretronephrosis on initial evaluation, among whom 74 (58.7%) had necrosed papillae in the PCS. On the contrary, 25 (41%) of the 61 (32.6%) patients who did not have hydrouretronephrosis had filling defects in the PCS on RGP and necrosed papillae retrieved by RIRS. Four patients required percutaneous nephrostomy and extraction of the necrosed papillae. Table 4 shows the outcomes of the urinary diversion and RIRS. There was a significant improvement in total leukocyte counts, serum creatinine values, and eGFR values after urinary diversion (DJS placement) (p < 0.05), and at 6 months after RIRS (1.4 ± 0.7 mg/dL, p < 0.05), compared with the values before urinary diversion.
Outcomes Following Urinary Diversion and Retrograde Intrarenal Surgery in the Study Cohort
Data presented as mean ± standard deviation.
Denotes statistical significance (<0.05) when comparing means using ANOVA (Tukey post hoc analysis).
RIRS = retrograde intrarenal surgery.
Discussion
Acute pyelonephritis is a bacterial infection that causes inflammation of the kidneys, and it is one of the most common kidney diseases. Pyelonephritis occurs as a complication of an ascending UTI, which spreads from the bladder to the kidney and then to the collecting system. The main cause of acute pyelonephritis is gram-negative bacteria, with the most common being E. coli. Other gram-negative bacteria that cause acute pyelonephritis include Proteus, Klebsiella, and Enterobacter. The first line of treatment in these patients is appropriate intravenous antibiotics as per urine culture sensitivity reports, analgesics, and antipyretics.
However, patients who do not respond to the first line of treatment with persisting fever, tachycardia, and flank tenderness require an endoscopic intervention in the form of DJS placement, which is a well-accepted modality. 6,7 It is recommended to perform DJS placement in pyelonephritis patients even in the absence of HUN, due to ureteric dyskinesia. Infection can cause decreased ureteric mobility by two mechanisms: bacterial toxins acting directly on the ureteric smooth muscle, and bacteria producing products acting on the ureteral peristalsis mechanism. 8
In patients who present with acute pyelonephritis and ureteric obstruction, semi-rigid ureteroscopy is a proven modality to relieve the obstruction by removing the sloughed-out necrosed papilla from the ureter. 9 However, there is no evidence in the literature regarding the role of RIRS in patients who undergo DJS placement during the acute phase of pyelonephritis, with or without HUN. Necrosed papilla, if present in the PCS (Fig. 1a), becomes the cause of an impending ureteric obstruction, leading to another episode of pyelonephritis/urosepsis. Hence, as a protocol at our institute, all diabetic pyelonephritis patients who require DJS placement undergo RGP, and if there is a filling defect, RIRS is performed after 3 weeks during DJS removal.
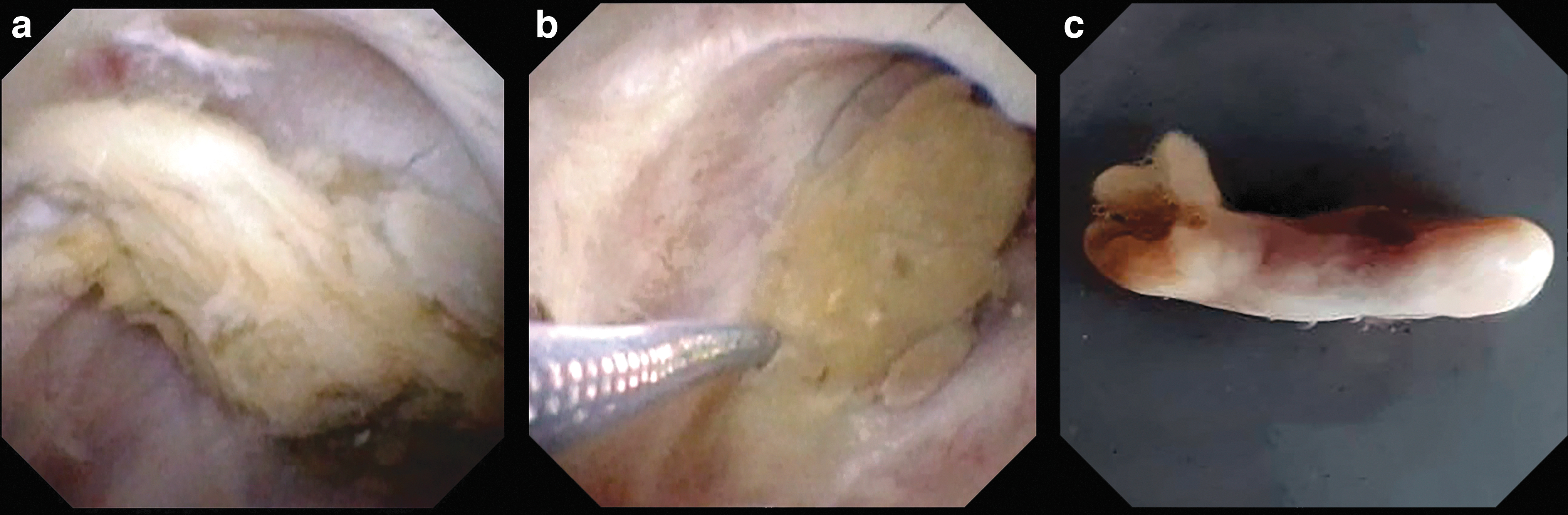
Patients with a DJS placed in situ when operated before 4 weeks have a similar rate of postoperative infection/sepsis compared with patients without stent placement; hence, the decision to perform RIRS at the end of 3 weeks is justified. 10 The ureter would be adequately dilated to accommodate a larger ureteric access sheath due to a low intrarenal pelvic pressure, faster operative time, and a larger access sheath allowing retrieval of the necrosed papillae with a basket (Fig. 1b).
Recurrent pyelonephritis is a common symptom in patients with diabetes, and necrosed retained papillae in the PCS are the most important cause. The more serious complications of pyelonephritis include renal abscesses, RPN, and emphysematous pyelonephritis, which are encountered more frequently in patients with type 2 diabetes than in the general population. 11,12 With retained necrotic renal papillae in the PCS, the probability of the earlier mentioned complications is even higher, and they become a nidus for further episodes of pyelonephritis, fungal ball formation, and stone formation.
The increased risk of UTI among patients with diabetes coupled with the increase in the incidence of type 2 DM worldwide in recent years may impose a substantial burden on the medical costs. 13 This is even more relevant in South east Asia and especially in India, which has emerged as a diabetes capital and a large population with poor glycemic control (76.6%). 14 Hence, timely removal of necrosed renal papillae from the PCS in diabetic patients results in decreased further episodes of pyelonephritis and reduced medical costs. In our study, the incidence of recurrent pyelonephritis was 3.89% during the 6-month follow-up period.
The limitation of this study is its lack of control group and short follow-up period (6 months). A longer follow-up is essential to understand the advantages of performing RIRS and retrieving necrosed papillae compared with the rate of recurrent pyelonephritis and its eventual impact on eGFR. The RPN is a pathologic entity and a bilateral disease, and in this study, we only assessed the symptomatic renal unit. There is no literature available on this modality; hence, a prospective multicenter comparative study with a long-term follow-up is required for better understanding and development of appropriate guidelines for RIRS in RPN management.
Conclusion
We believe that RIRS plays a definite and significant role in the management of patients with diabetic RPN who present with pyelonephritis/urosepsis. Retrieving the necrotic papillae by using RIRS prevents the impending ureteric obstruction, leading to recurrent pyelonephritis and urosepsis. However, RPN is a recurrent disease; therefore, this modality does not cure the disease, but it only delays further episodes of pyelonephritis.
Footnotes
Authors' Contributions
D.R.—Writing, Conception, Design, Supervision, Analysis, and Literature review. G.S. and D.S.—Literature search and Data collection. S.G., B.E., and T.B.—Conception, Design, and Analysis. P.R.K. and M.C.—Conception, Design, Supervision, Analysis, and Critical review.
Acknowledgment
The authors appreciate the efforts and handwork of the team involved in assisting, extracting, collecting, and compiling the patient data.
Statement of Ethics
Informed written consent was obtained from all the patients. The scientific committee and institute review board of the Asian Institute of Nephrology and Urology has approved the study (Protocol No.: AINU 08/2019).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.