
Abstract
Purpose:
Digital ureteroscopes employ “chip-on-the-tip” technology that allows for significant improvement in image resolution. However, image distortion often occurs during laser lithotripsy owing to acoustic wave production. We sought to compare image distortion using different laser power settings and distances from the laser fiber tip to the scope for the Super Pulsed Thulium Fiber (SPTF) laser and high-power Holmium:YAG (Ho:YAG) laser.
Materials and Methods:
Ureteroscopy was simulated using a silicon kidney-ureter-bladder model fitted with a 12F/14F access sheath and the Lithovue™ (Boston Scientific), disposable digital flexible ureteroscope. At defined laser parameters (10, 20, 30 and 40 W, short pulse), a 200-μm laser fiber was slowly retracted toward the tip of the ureteroscope during laser activation. Image distortion was identified, and distance from the laser tip to the scope tip was determined. Data from the two lasers were compared utilizing t-tests.
Results:
After controlling for frequency, power, and laser mode, utilizing 1.0 J of energy was significantly associated with less feedback than 0.5 J (−0.091 mm, p ≤ 0.05). Increased power was associated with larger feedback distance (0.016 mm, p ≤ 0.05); however, increase in frequency did not have a significant effect (−0.001 mm, p = 0.39). The SPFT laser had significantly less feedback when compared with all Holmium laser modes.
Conclusions:
Increased total power results in image distortion occurring at greater distances from the tip of the ureteroscope during laser activation. Image distortion occurs further from the ureteroscope with Ho:YAG laser than with SPTF fibers at the same laser settings. In clinical practice, the tip of the laser fiber should be kept further away from the tip of the scope during ureteroscopy as the power increases as well as when utilizing the Ho:YAG system compared with the SPTF laser platform. The SPTF laser may have a better safety profile in terms of potential scope damage.
Introduction
Dr. Victor Marshall posed a question almost 60 years ago during the infancy of ureteroscopy, “Would it not be useful to be able to look down a flexible tube and see clearly out the other end while the tube was being bent in various directions?.” 1 Urological procedure has since seen significant advancements of ureteroscopy with the development of working channels, bidirectional active deflection, irrigation capabilities, new types of lasers (e.g., holmium:YAG laser [Ho:YAG], thulium fiber laser [TFL]) and the use of digital flexible ureteroscopes. 2
Digital ureteroscopes use “chip on the tip” technology that allows for superior image resolution compared with fiber optic images. 2,3 Although early digital ureteroscopes experienced significant image distortion owing to acoustic shockwaves produced during laser lithotripsy, the addition of shock absorbers at the microchip has decreased the image flickering. 4 However, image distortion continues to occur owing to the photoacoustic effect of the laser when activated near the tip of the ureteroscope.
Ho:YAG lasers have been long considered the gold standard for laser lithotripsy with TFL lithotripsy a novel, new technology. TFLs, which include the Super Pulsed Thulium Fiber™ (SPTF), have documented advantages over Ho:YAG, including an emission wavelength that more closely matches the water absorption peak resulting in more efficient and safer stone ablation at lower energy settings. 5,6 As the energy of the SPTF laser is absorbed by water ∼16,000 times more than that of the Ho:YAG laser at a distance of 1 mm, a reduction in photoacoustic feedback produced during laser activation is also expected. 7
The digital age of ureteroscopy has been entered, yet the spirit of Dr. Marshall's question remains. There is a clear need for further investigation at what point image distortion occurs while using Ho:YAG, the gold standard of laser lithotripsy, along with the promising technology of SPTF laser. In this study, we sought to compare the distortion of the SPTF laser with the high-power Ho:YAG laser while using variable laser settings and laser fiber tip distance from the scope's tip (“tip-to-chip” distance) with the LithoVue® flexible ureteroscope. We hypothesized that the SPTF laser would cause less image distortion than the Ho:YAG laser.
Materials and Methods
This study was approved by the University of Kansas Medical Center's Institutional Review Board. We utilized a silicon kidney-ureter-bladder model fitted with a 12F/14F ureteral access sheath as a laboratory model to simulate ureteroscopy. A 200-μm laser fiber for both the SPTF (Soltive™, Olympus®) and the Ho:YAG laser (P120-Lumenis™) was utilized using a disposable digital ureteroscope, Lithovue™ (Boston Scientific®). The following laser modes were investigated: Ho:YAG Short-Pulse (HoSP), Ho:YAG Moses Distance (HoMD), Ho:YAG Moses Contact (HoMC), and SPTF Short-Pulse. Settings were utilized at defined laser parameters (energy of 1.0 or 0.5 J and its corresponding Hz for total power of 10, 20, 30, and 40 W).
The ureteroscope was always positioned straight (no deflection), and the laser fiber was slowly retracted toward the scope's tip during laser activation by an experienced endourologist (W.M.). The laser was fired for a short time (≤3 seconds) while physiologic saline irrigation was running via gravitational inflow at 60 cm above the KUB model. No fiber burn-back was appreciated so no fiber stripping was required. This process was repeated with each laser at each specified laser setting. Endoscopic video was recorded during these procedures for all laser settings and fiber types. Image distortion was identified and defined as when horizontal lines appeared on the endoscopic video screen. The distance from the laser tip to the scope tip was determined via the endoscopic video image when distortion first occurred. Because the laser fiber exits the scope at an angle, the endoscopic video distance was determined by measuring the number of pixels of fiber exposed (Fig. 1). This was normalized to a curve that had previously been determined using known laser fiber distance measurements (Supplementary Figs. S1 and S2).
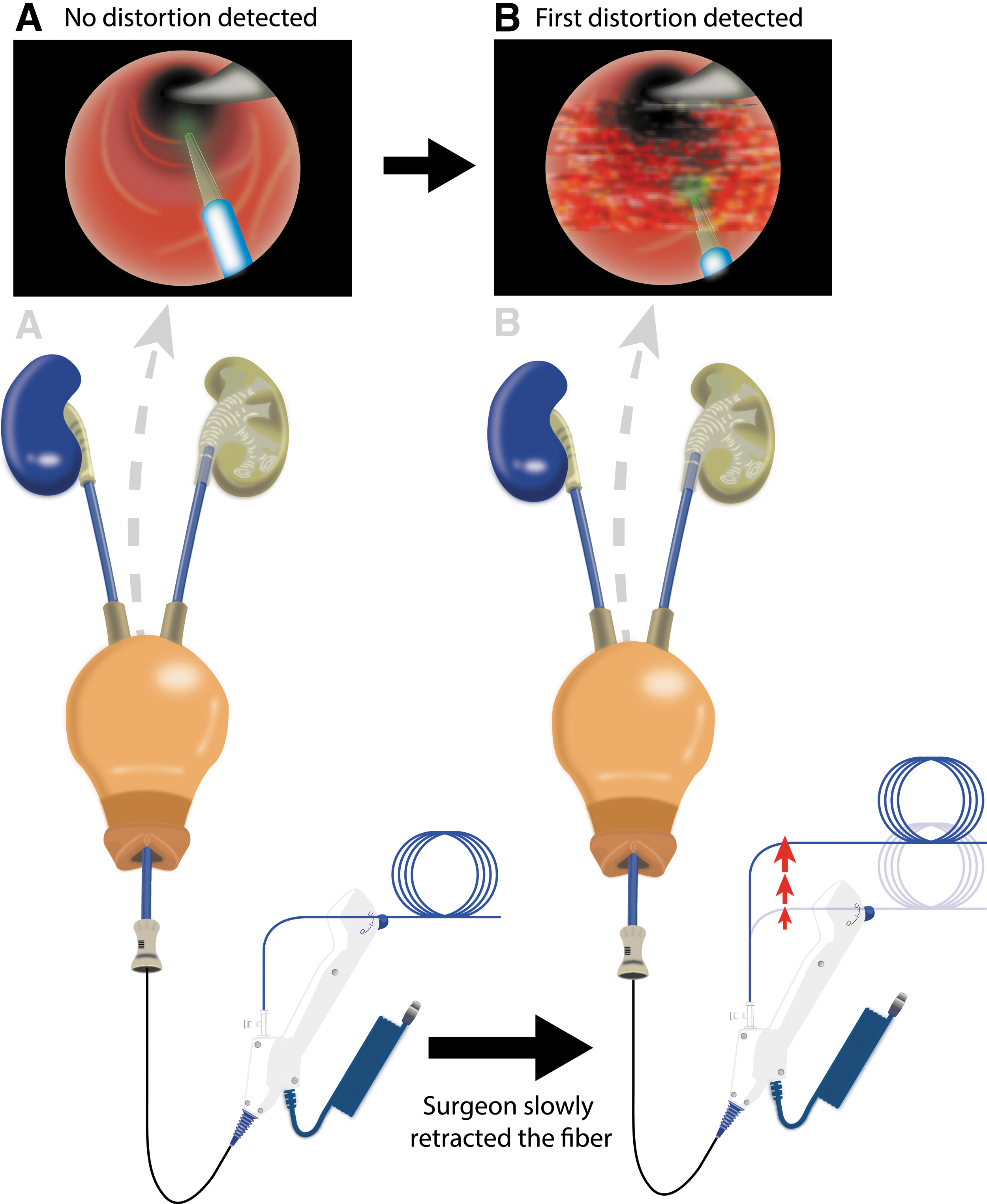
Image distortion and feedback distance measurements.
Statistical analysis
All experiments were repeated four times for each laser and each energy setting. The results were reported as distance means (mm) and compared utilizing the ANOVA with post hoc analysis (Tukey's test). As power and laser mode have an effect modification in the feedback distance, a multiple regression model was built based on that interaction (power and laser modes) with coefficient significance levels of 0.05. Because high-power Ho:YAG laser is the gold standard in laser lithotripsy, HoSP was treated as the reference level for comparison.
Results
The average tip-to-chip distances are given in Table 1, according to laser type and settings. A post hoc analysis demonstrated no difference when Ho:YAG categories were evaluated, but there was a statistically significant difference when SPTF was compared with Ho:YAG modalities for all laser settings.
HoMC = Ho:YAG Moses Contact; HoMD = Ho:YAG Moses Distance; HoSP = Ho:YAG Short-Pulse; SPTF = Super Pulsed Thulium Fiber.
Considering the relationship between the variables (J × Hz = W), a multiple regression model was utilized. Increased power (W) was associated with larger feedback distance (0.016 mm, p ≤ 0.05), that is, as power is increased, the laser must be kept further away from the ureteroscope to avoid image distortion. Isolated increases in frequency (Hz) did not have a significant effect (−0.001 mm, p = 0.39). After controlling for frequency, power, and laser mode, increased energy (1.0 J vs 0.5 J) was significantly associated with a shorter feedback distance (−0.091 mm, p ≤ 0.05) for all laser types and settings, that is, when compared within the same laser mode and at equal power levels, the laser tip can be placed closer to the ureteroscope when using 1.0 J and must be kept further away when using 0.5 J to avoid image distortion.
When comparing laser modes, there was a significant increase in the distance at which image distortion occurred when using HoMD (average of 0.141 mm, p < 0.05) when compared with HoSP, but there was no difference when using HoMC (−0.015 mm, p = 0.78). SPFT had significantly shorter distance to the tip of the laser fiber at time of feedback when compared with HoSP (average of −0.298 mm, p < 0.05) (Fig. 2).

Image distortion comparison by laser and mode. The HoSP mode was used as the reference to report the average distances in feedback. Note the significant differences in distance among the HoSP vs HoMD and SPTF. Oppositely, overall similar distances between HoSP and HoMC were verified. SPTF = Super Pulsed Thulium Fiber. Color images are available online.
When the interactions of power and laser mode were analyzed individually, there was no significant difference in the laser distance at which feedback was experienced with HoMD or HoMC compared with HoSP. However, SPTF showed significantly less increase in the distance as power increased (Fig. 3). For example, at a total power of 30 W, HoSP resulted in image distortion at a longer distance: 2.71 mm from the scope's tip compared with 2.30 mm for SPTF.
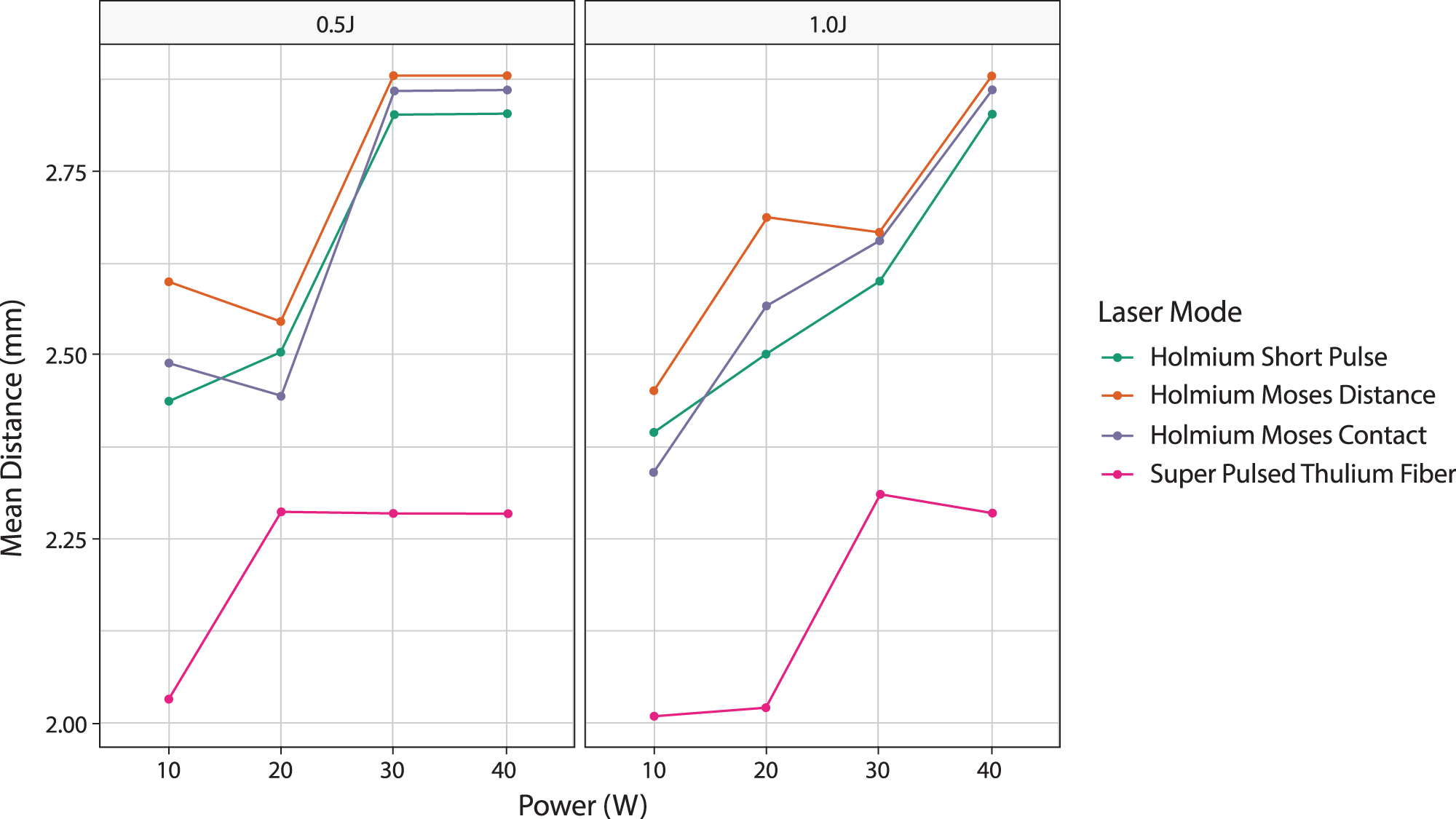
Comparison of laser and laser modes at 0.5 or 1.0 J and variable total power settings. Color images are available online.
Pairwise comparison between laser modes was performed after averaging over energy, frequency, and power (Fig. 4). Although significant differences for the Holmium laser group were found, in clinical or practical terms they become negligible. However, when we compared any Holmium modality to SPTF, more significant differences were seen.
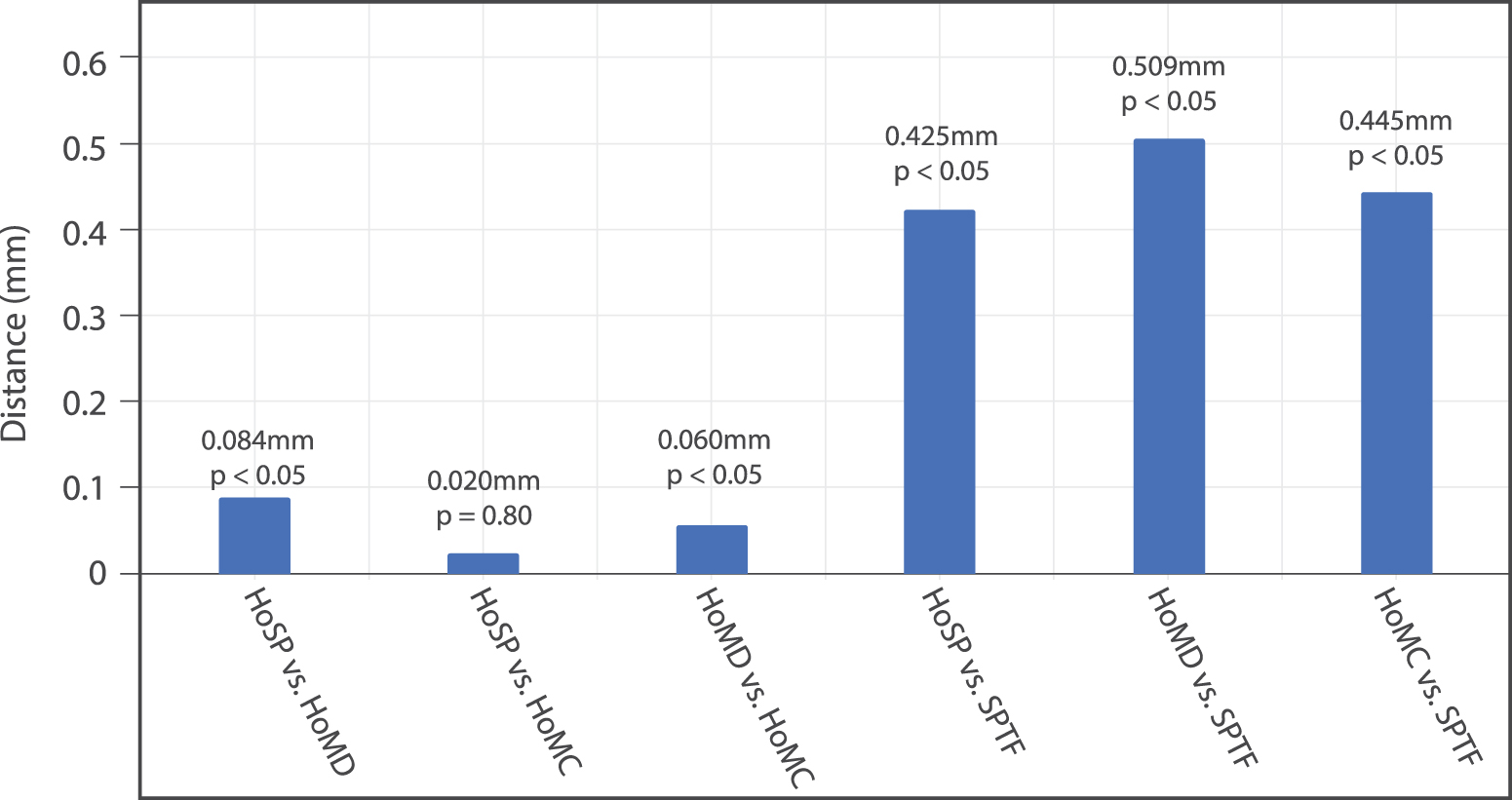
Pairwise comparison averaging difference in image distortion distance. Color images are available online.
Discussion
Despite the inarguable improvements in image quality, flexible digital ureteroscopes have some drawbacks such as higher fragility, higher maintenance costs, and greater image interference. 4 Since the spread of the “chip-on-the-tip” technology, the problem with image distortion during laser lithotripsy has become even more concerning. 8 The main culprit for this occurrence is thought to be the photoacoustic effect of pulsed lasers, especially when activated close to the tip of the scope. 2
Inside the endoscopic environment, any distortion of the displayed image can be harmful, potentially compromising visibility and procedure efficacy. 9 In terms of clinical outcomes, it may be responsible for an increase in operative time, procedure difficulty, and surgeons' perceived stress, ultimately resulting in decreased stone-free rates. From the perspective of patient safety and cost burden, it may contribute to iatrogenic injuries and laser fiber retraction leading to increasing scope breakage and frequency of maintenance and repairs. 10 –12
As accidental off-target energy is responsible for scope damage, image interference and noise production can indirectly measure the photoacoustic effect and energy misuse as a warning for imminent scope breakage. 11,13 The main goal of this study was to evaluate if different laser modalities impact image distortion. Our experiment showed the interaction between laser mode and power to be vital in terms of image interference. As a rule of thumb, the greater the power, the greater the distance between the laser fiber to the scope's chip to generate image distortion (i.e., the surgeon needs to keep the tip of the laser fiber further away from the scope's tip to prevent image distortion).
When comparing different settings of frequency and energy within the same power (e.g., 0.5 J and 20 Hz = 10 W vs 1.0 J and 10 Hz = 10 W), we demonstrated a potential benefit by choosing the combination of higher energy and lower frequency to limit image distortion. It is speculated that higher frequencies would increase the number of pulse vibrations that reach the scope, decreasing the efficacy of the shock absorber, resulting in more image interference. It is important to note that while our study does demonstrate decreased image distortion using higher energy and lower frequency settings, there is potential for increased risk of thermal injury with higher laser energy. 14 Both the SPTF and Ho:YAG systems are capable of producing a temperature rise in the ureter owing to laser firing. 15 Other in vitro studies have shown that adequate irrigation rates can help to maintain stable temperatures when higher energies are applied; however, the effects of these settings and irrigation rate in vivo require further exploration. 16
Specifically comparing laser platforms, the superiority of the SPTF over the Holmium group was evident. The SPTF's wave-length (1940 nm) results in a shorter optical penetration depth (OPD) of 0.077 mm compared with the Ho:YAG (2100 nm, OPD = 0.314 mm). The reduction in OPD means that, as the laser beam travels through the fluid, more energy is dissipated when utilizing the SPTF (energy reduced to ≤0.0001% over 1 mm) vs the Ho:YAG (energy reduced to 4% over 1 mm). 17,18 With less energy available to reach the chip-on-the-tip, the SPTF laser generates less image interference.
In addition, the SPTF showed a remarkable resistance in image flickering with power increases. No clinically significant discrepancies in feedback distances were noticed with increases in power with this laser platform, especially when utilizing lower energies (Fig. 3). Again, this is explained by the SPTF characteristic wavelength and shorter OPD. In contrast, the Ho:YAG group strictly followed the rule of “the greater the power, the greater the distance” as the increases in power resulted in further distances causing image distortion. The SPTF's resistance to image distortion during ureteroscopy, along with the lower tissue and water penetration depth and the lower chances of damaging nontargeted structures, 18 contributes to a safety profile favoring the SPTF for laser lithotripsy during flexible ureteroscopy. 17
One can argue that if the SPTF allows the tip of the laser fiber to work closer to the tip of the scope, it could also increase the chance of scope damage in the event of an accidental push of the fiber into the working channel of the scope. For example, this could occur during lithotripsy if the fiber were pushed against a stone inadvertently. Although thoughtful, future investigations are needed to conclude whether the SPTF is a potential factor in scope breakage.
Conclusions
Increased total power results in image distortion occurring at greater distances during laser lithotripsy with flexible ureteroscopy. In addition, image interference occurs at a greater distance with Ho:YAG than with SPTF at the same laser settings. This may contribute to improved intraoperative surgeon experience with the SPTF laser, causing less image distortion and potentially decreasing the chances of scope damage and injury to non-target structures.
Footnotes
Author Disclosure Statement
W.R.M. is a consultant for ForTec, Boston Scientific, and Olympus. D.A.D. is a consultant for Intuitive Surgical. D.A.N. is a consultant for Boston Scientific and Lumenis. All other authors have nothing to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.