
Abstract
Objective:
A noninferiority assessment of single-use digital flexible cystoscopy (FC) compared with standard reusable FC for bladder cancer surveillance, and investigation of lower urinary tract symptoms.
Patients and Methods:
Patients requiring FC who met inclusion criteria were randomly assigned to have their procedure performed using a single-use cystoscope (Ambu® aScope™ 4 Cysto System) or a standard reusable cystoscope (Olympus CYF-VH flexible video cystoscope). Primary outcomes were noninferiority of the single-use cystoscope, in terms of effective procedure completion rate, image quality, light quality, and maneuverability. Secondary objectives compared safety, operative, and perioperative time. The noninferiority margin was set at −10%.
Results:
One hundred one patients completed the study (n = 50 trial, n = 51 control). All primary outcomes demonstrated noninferiority of the single-use cystoscope, compared with standard reusable FC. Effective completion rate, image quality, light quality, and maneuverability between single-use and reusable cystoscopes were 100% and 98% (confidence interval [CI]: −0.059 to 0.019); 96% and 100% (CI: −0.014 to 0.092); 98% and 100% (CI: −0.018 to 0.058); and 98% and 100% (CI: −0.018 to 0.058). There was no difference in operation time (p = 0.415) or total theater use time (p = 0.441) between groups. Adverse event rates were 4.08% and 4.16% in the trial group and control groups, respectively.
Conclusion:
The single-use Ambu flexible cystoscope is noninferior to standard FC in terms of procedure completion and light quality, image quality, and maneuverability. Single-use flexible cystoscopes are an effective and safe alternative to reusable flexible cystoscopes and may act as a suitable alternative or adjunct in the urologist's armamentarium.
Introduction
Flexible cystoscopy (FC) is the cornerstone of investigation and surveillance of lower urinary tract pathologies. Present-day reusable flexible cystoscopes have advanced greatly from their earlier predecessors; they possess excellent lighting and optical specifications, coupled with precise and nimble maneuverability and have been shown to be reliable. 1 Despite this, reusable flexible cystoscopes present a number of downsides, which relate primarily to their high up-front costs, 2 and reliance on costly reprocessing and maintenance. The emergence of novel single-use flexible cystoscopes has introduced a potential alternative to reusable devices and may even serve as a more favorable option in some settings.
Head-to-head analyses of single-use and reusable flexible endoscopes for other indications, such as choledochoscopy 3 and ureteroscopy, 4 have shown comparable endpoints, with no significant inferiority with the use of disposable devices. This study assesses the single-use cystoscope (Ambu® aScope™ 4 Cysto System). Recent studies have suggested this novel device has comparable specifications, is well tolerated, and is more cost-efficient compared with single-use cystoscopes. 5,6 However, the practical utility of this device, in terms of image quality, light quality, and maneuverability, has not been determined in an appropriate randomized noninferiority study.
Patients and Methods
Study design, ethics, and registration
Ethics were approved by local ethics committee (HREC/7491/VICBH-2021-266361 v1). A single-center open-label noninferiority trial with balanced randomization (1:1) was performed at University Hospital Geelong, Victoria, Australia in between September 2021 and January 2022. Study recruitment is shown in Figure 1. The sample size was calculated at 96 (48 in each group) according to the noninferiority sample size calculation; 7 applying a noninferiority limit of −10%, α = 0.05, power = 0.8, and assuming an equal score for each outcome parameter for both groups. Randomization was carried out using a computerized random numbers generator. 8
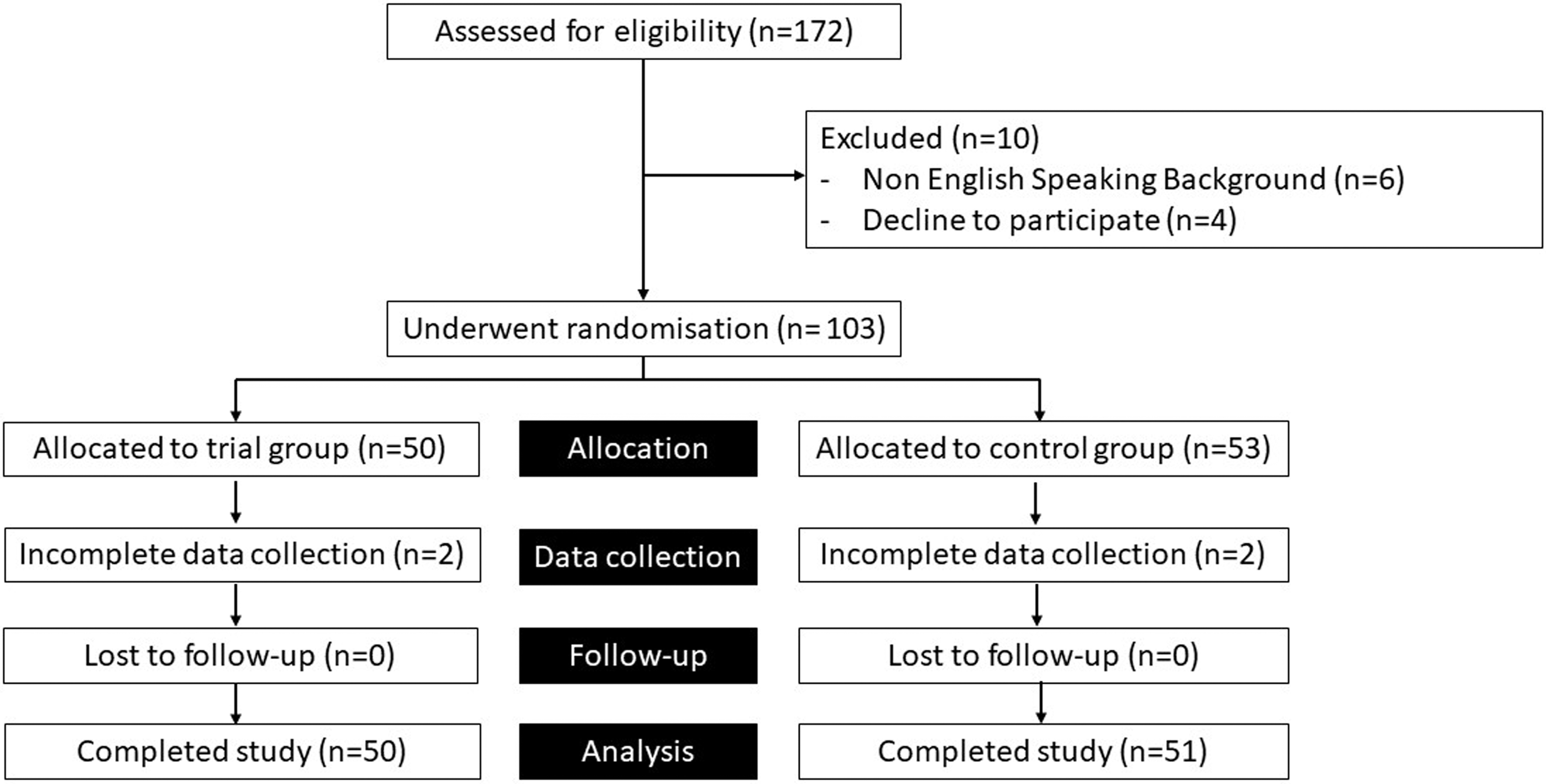
Flow diagram showing study recruitment.
Inclusion and exclusion criteria
Patient inclusion criteria
Men and women >18 years.
Patients capable of giving informed consent for themselves.
Patients with an adequate level of English to be able to read the trial handout.
Patients having an FC under local anesthetic for the investigation of lower urinary tract symptoms, including hematuria, or for surveillance of bladder cancer.
Operator inclusion criteria
Urologist or urology registrar who has performed >100 flexible cystoscopies using a standard reusable flexible cystoscope, and who has had an in-service introduction to the Ambu aScope 4 Cysto System and had subsequent experience with using the device before the study commencing. In total five operators met our inclusion criteria, one consultant urologist, and four urology registrars.
Surgical technique and follow-up protocol
All procedures were performed using local anesthesia only in an operating theater. Routine prophylactic antibiotics were not given. Patients were in the supine position, standard surgical prep and drape, and a surgical timeout were performed. Local anesthetic was introduced per urethra (2% lignocaine gel) before introduction of the flexible cystoscope. Complete examination of the urethra, prostate, and bladder were performed. Physiologic saline irrigation was used for the procedure.
Trial device
Ambu aScope 4 Cysto System (Ambu A/S, Ballerup, Denmark) is a disposable cystoscope that costs $280AUD per unit (Fig. 2), with a unit price of $7500AUD for the Ambu aView 2″ portable full HD screen, each manufactured in Penang, Malaysia. 9

Ambu® aScope™ 4 Cysto System. Color images are available online.
Outcome assessment
The following primary endpoints were assessed: effective completion of the FC procedure (Yes/No); confidence that image quality of cystoscope allowed accurate assessment of the entire urethra and bladder (Yes/No); adequate light quality to confidently perform procedure (Yes/No), adequate maneuverability to confidently assess entirety of the urethra, bladder, and bladder neck (Yes/No). Binary endpoints were used in an attempt to establish a more accurate determination of noninferiority in this study.
We deemed that using scaled endpoints may increase systematic bias, as scaled endpoints are likely to have poor test–retest reliability compared with binary endpoints in this setting. Secondary endpoints included comparison between procedure time to completion, patient journey from entry into operating theater to surgical sign-out. Further data collected included assessment of any delays during the patient journey from entry into operating theater to surgical sign-out (Fig. 3), with a description of the delay recorded. Patients were followed up through phone call a week later to assess for any adverse outcomes after the procedure.
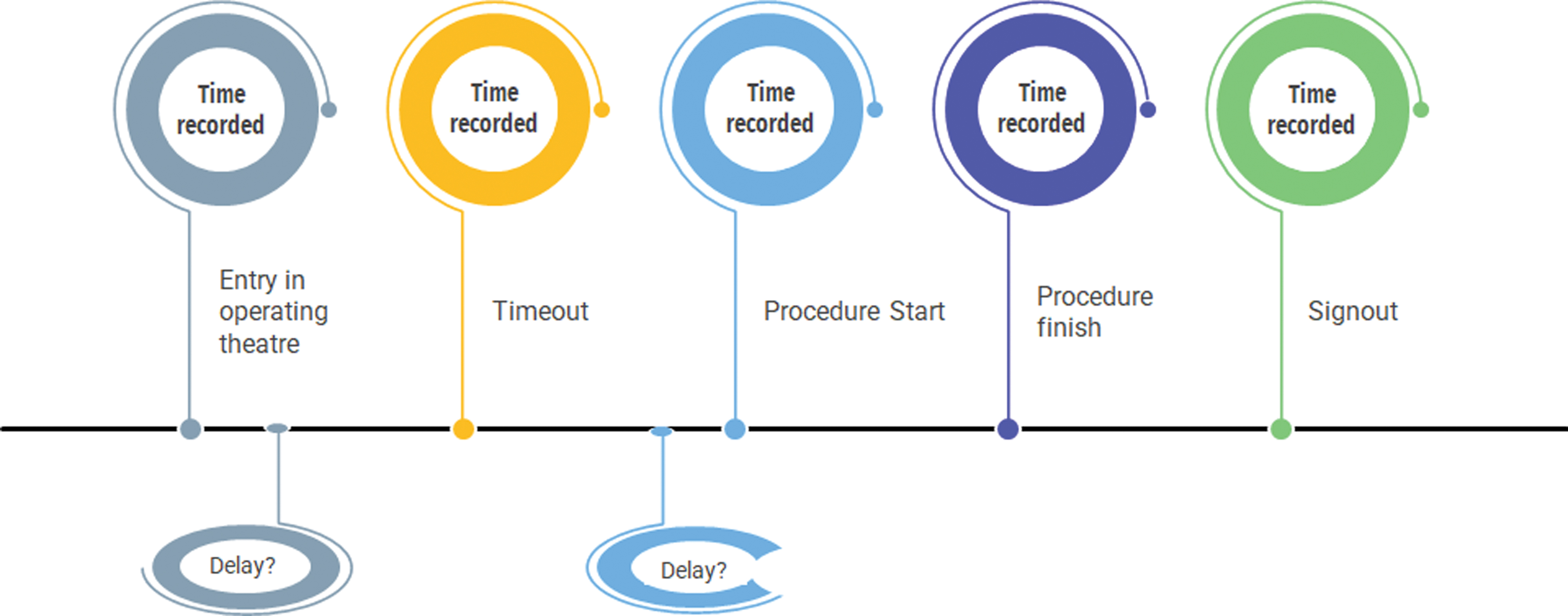
Timeline of patient journey. Time was recorded (minutes and seconds) at patient entry into the operating theater, surgical timeout preprocedure, procedure start (entry of cystoscope into meatus), procedure finish (cystoscope exit meatus), and surgical sign-out. Delays between entry into operating theater and before commencing procedure were recorded. Color images are available online.
Statistical analysis
Data were analyzed using STATA (Version 15.1) (StataCorp 2017. Stata Statistical Software: Release 15; StataCorp LLC, College Station, TX, USA). Primary and secondary outcomes were analyzed for all patients who underwent FC and completed 1 week follow-up. The Newcombe–Wilson confidence interval (CI) 10 for the difference between the two procedures was computed. Two-sided tests of proportions with the 95% CI of the difference in the completion rate, image quality, light quality, and maneuverability were calculated. Noninferiority was statistically determined if the lower limit of the CI did not breach the noninferiority margin of −10%.
Secondary outcomes were assessed using Fisher's exact test for categorical variables, using α = 0.05. Normality tests for the time variables were done using the Shapiro–Wilk test and when found not to be normally distributed, Mann–Whitney two sample test was used to assess differences between groups.
Results
Data were available for 50 patients in the single-use group and 51 in the reusable group. Almost all (n = 100, 99%) procedures were effectively completed. One procedure was unsuccessful because of a complicated stricture requiring dilation, this patient had been randomized to the reusable group. Minor adverse events included mild dysuria and hematuria. The rates of these events were similar between groups (4.08% and 4.16% in single-use and reusable groups, respectively). There were no postoperative urinary tract infections in either group.
Effective completion rate, image quality, light quality, and maneuverability between single-use and reusable cystoscopes were 100% and 98% (CI: −0.059 to 0.019); 96% and 100% (CI: −0.014 to 0.092); 98% and 100% (CI: −0.018 to 0.058); and 98% and 100% (CI: −0.018 to 0.058). The lower limit of the CI did not exceed the noninferiority margin for any primary outcome parameter, confirming noninferiority of the single-use cystoscope (Fig. 4). There was no difference in operation time (p = 0.415) or total theater use time (p = 0.441) between groups (Table 1).
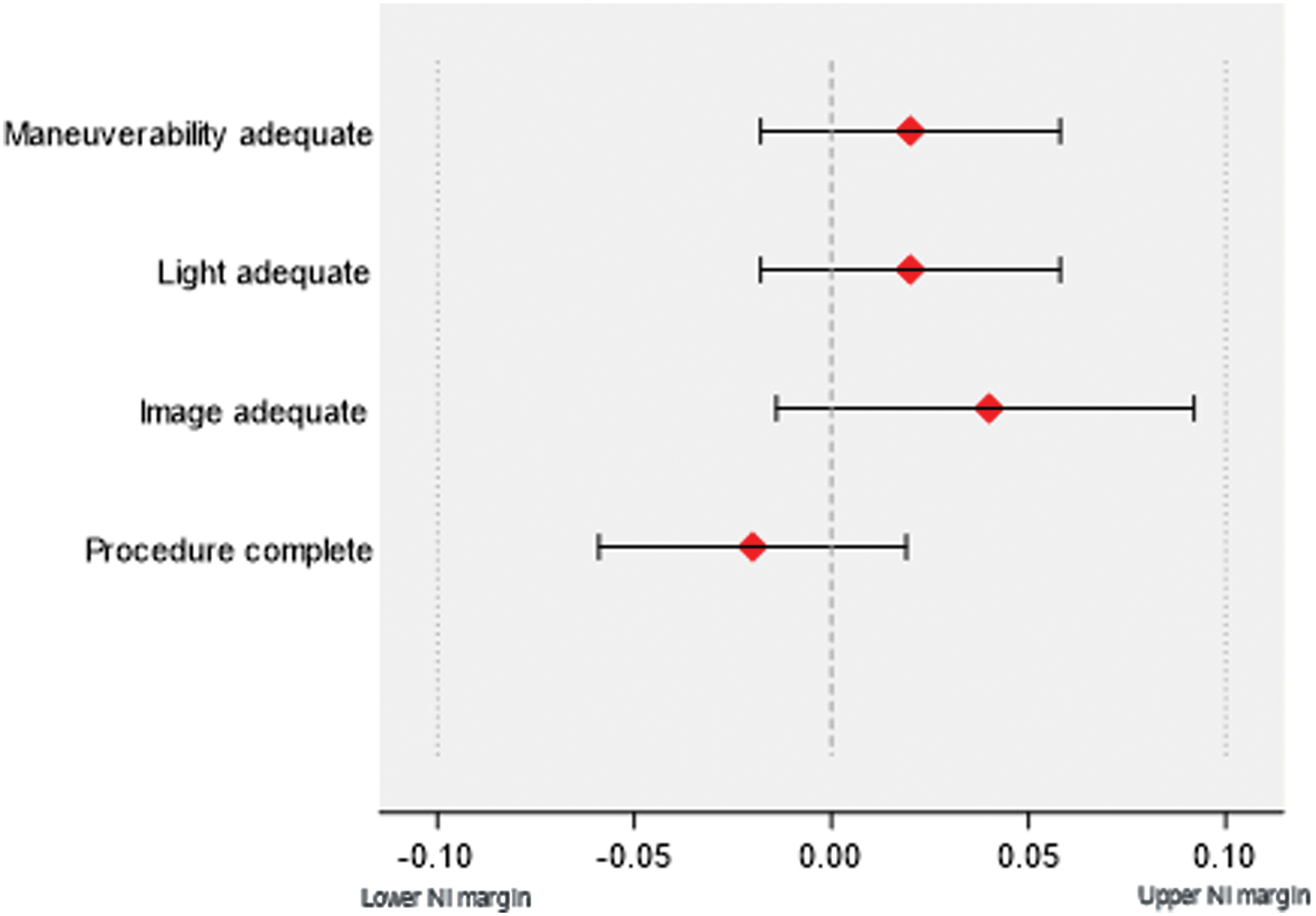
Primary outcomes. Single-use flexible cystoscope shown to be noninferior with CI more than −10% in each of the four assessed domains. CI = confidence interval. Color images are available online.
Comparing Single-Use and Reusable Cystoscopes
Operation time defined as entry into meatus until completion of procedure and exit from meatus. Total theater time defined as entry into operating theater until surgical sign-out. Median and CI (25% and 75%) are shown.
CI = confidence interval.
Discussion
Single-use flexible cystoscopes provide an alternative to reusable cystoscopes, and may provide advantages over reusable cystoscopes in some settings, as they are easily portable, sterile, and do not require reprocessing. Single-use flexible cystoscopes are becoming increasingly available, 11 and given their potential advantages over reusable cystoscopes, the uptake of these devices is likely to expand. 12 However, before this study the clinical utility of these devices had not yet been scrutinized in an appropriate clinical trial.
Reusable flexible cystoscopes represent a significant economic burden for health care services, with significant costs associated with the purchase and maintenance of these devices. 2 Lower up-front costs ($280AUD per device) may make single-use devices more attainable in some settings, with some evidence to suggest that single-use cystoscopes are overall more cost-effective. 5
The sterilization process for reusable cystoscopes poses not only an economic burden, but also a potential source of nosocomial infection. The US Food and Drug Administration (FDA) has recently reported concerns about the effectiveness of reprocessing of reusable urologic endoscopes, and is investigating hundreds of medical device reports linking these devices to postprocedure infections. 13 Because of the internal complexity of reusable endoscopes generally they are not amenable to sterilization processes that involve soaking and, therefore, are susceptible to bacterial colonization of internal working elements and lumens. 14 Reusable flexible endoscopes are considered to possess the highest health care-related infection rates of any medical device. 15 Given the inherently low rates of infection associated with FC, however, a large study population would be required to demonstrate a reduced infection risk with single-use cystoscopes. There were no infections reported in either group in this study.
The requirement to reprocess reusable cystoscopes has the further potential to negatively impact efficient theater utilization, if it results in delays. 16 Our data captured seven episodes where procedures were delayed because of reprocessing of reusable equipment. These delays did not result in a statistical difference between the groups in this study, but may be an issue more pertinent to facilities that have fewer numbers of reusable cystoscopes, and are reliant on effective recycling and reprocessing of cystoscopes to enable efficient theater flow. Previous studies have shown that increased productivity has resulted from the adoption of single-use flexible cystoscopes 6,12 and there is evidence that the longevity of reusable flexible endoscopes can be extended when single-use devices are integrated into a service. 16
Furthermore, the sterilization process for reusable endoscopes is associated with a significant carbon footprint. This is important, as governments try to tackle climate change resulting from industrial emissions. Analysis of the carbon footprints associated with other flexible endoscopes, such as flexible ureteroscopes, has suggested that single-use devices are associated with comparable emissions. 17 Analysis of carbon footprints related to the two groups was outside the scope of this study, but will be assessed in a follow-up study.
Market readiness for single-use flexible cystoscopes has been demonstrated, with almost half of urologists surveyed being willing to make the change to single-use cystoscopy. 12 This study should serve to reassure practitioners that the utility of single-use flexible cystoscopes is comparable with standard reusable devices. The Ambu aScope 4 Cysto System is noninferior to the Olympus CYF-VH flexible video cystoscope regarding procedure completion and adequacy of light, image, and maneuverability. Single-use flexible cystoscopes are an effective and safe alternative to reusable flexible cystoscopes and may act as a suitable alternative or adjunct in the urologist's armamentarium.
Strengths of our investigation include its design as a prospective randomized control trial with binary primary outcomes to accurately assess noninferiority. This is of practical use for clinicians. Limitations include the data collection of timing. In retrospect it would have been better to capture data for all of patient journey from check-in to sign-out, as perhaps there were confounding factors that were not captured where a patient was unknowingly delayed entry into theater because of check-in issues that were not conveyed to surgical team.
Footnotes
Acknowledgment
Dr Stella May Gwini, biostatistician, Barwon Health, Geelong, Victoria, Australia.
Authors' Contributions
Data curation, formal analysis, investigation, project administration, visualization, and writing—original draft by A.H. Investigation and writing—original draft by A.W. Conceptualization, methodology, investigation, and writing—review and editing by D.O'K. Conceptualization, project administration, supervision, and writing—review and editing by R.G.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
An agreement was put in place that single-use cystoscopes would be purchased from Ambu by our hospital at a price equal to the calculated cost (of processing) per encounter for a reusable cystoscope. No additional funding was accepted from the manufacturer. They did not have any control or input into the operation of the study.