
Abstract
Objective:
To evaluate using an inanimate model the thermal injury and laser efficiency on high frequency, high energy, and its combination in hands of junior and experienced urologists during holmium YAG (Ho:YAG) and Thulium fiber laser (TFL) lithotripsy.
Methods:
A Cyber: Ho 150 WTM and Fiber Dust TFL (Quanta System) with 200 μm core-diameter laser fibers (LF) were used in a saline in vitro ureteral model. Each participant (five junior and five experienced urologists) performed 32 sessions of 5-minute lasering (125 mm3 phantom BegoStones™), comparing four modes (3 J/5 Hz [1.5 W], 0.3 J/20 Hz [6 W], 1.2 J/5 Hz [6 W], and 1.2 J/20 Hz [24 W]). Transparent tip and cleaved LF, and digital and fiberoptic ureteroscopes were also compared. Ureteral damage was classified in a scale (0–5) according to the burns and holes seen in the ureteral model's surface.
Results:
High-power (HP) setting (24 W) was associated with higher delivered energy and higher ablation rates (ARs) in both lasers (p < 0.001). For the same power setting (6 W), there was no difference in delivered energy or stone ARs. Regardless the settings, a higher AR was observed with TFL than with Ho:YAG (0.5Δ mg/s ± 0.33 vs 0.39 Δmg/s ± 0.31, p = 0.002) laser. Higher mean AR was found with cleaved tip vs transparent tip (p = 0.03) in TFL. For both lasers, higher ureteral damage was observed in the 24 W group (p = 0.006) and in the junior urologists (p = 0.03). Between 6 W groups, different types of lesions were found and junior urologist have more lesions when high frequency was used, for both Ho:YAG (p = 0.05) and TFL (p = 0.04).
Conclusion:
More stone ARs and reduced operative time are observed in HP settings; however, more ureteral thermic-related damage is produced. When comparing the same power, higher energy or frequency does not modify the AR. Nonetheless, more ureteral thermic-related thermal damage is observed in high-frequency settings in unexperienced hands.
Introduction
Holmium YAG (Ho:YAG) is the current gold standard for laser lithotripsy. 1,2 Since its first use, several technological upgrades and more powerful and high-frequency lithotripters have been developed. 3 Recently, the Thulium fiber laser (TFL) was authorized and is now evaluated as a safe alternative to Ho:YAG. 2 Although there are multiple studies assessing the in vitro performance of those lasers on artificial stone models with high-power (HP) lasers, there is a paucity of data about lithotripsy efficiency and safety. 4,5
Intraoperative complications occur in less than 3% of cases. 6 The incidence of ureteral strictures after ureteroscopic lithotripsy is 0.7% (range, 0.30–23.81%). 7 Despite the low rate, this complication can be serious. One of the possible reasons behind ureteral strictures may be the thermal effect of lasers on the ureteral mucosa during lithotripsy, especially in case of HP settings. 8 –11 Nevertheless, ureteral thermic-related thermal damage of TFL and Ho:YAG with high frequency, high energy, or its combination during endocorporeal laser lithotripsy is not known.
The aim of this experiment was to evaluate in an inanimate model the direct thermal damage and laser efficiency of both lasers (Ho:YAG and TFL) using different settings in hands of junior and experienced urologists during lithotripsy. The secondary point was to compare digital and fiberoptic scopes and laser fibers (LF) with and without the transparent tip, to assess the most efficient and safest combination during lithotripsy.
Materials and Methods
Laser systems
A Cyber: Ho 150 WTM and Fiber Dust TFL generators (Quanta System Samarate, Lombardia, Italy) were used. The laser settings can be set identically between the two laser generators (pulse energy and frequency). The following settings: 0.3 J at 5 Hz, 0.3 J at 20 Hz, 1.2 J at 5 Hz, and 1.2 J at 20 Hz, were tested (Table 1), with short pulse width from manufacturer's laser console settings, and an optical fiber 200 μm was used in all the tests.
Experimental Setup Settings
Artificial kidney stones
We produced 12 mm3 cubes of stone phantom according to previously described techniques. 12 Matching Begostone Plus (Bego France®, Villeurbanne, France) powder with distilled water, we aimed to reproduce calcium-oxalate monohydrate stones. A « powder to water » ratio of 15: 3 was chosen, according to previous in vitro studies. 13 After confection, a drying period of 48 hours at 30°C was respected to minimize the heterogeneity. All stones had been weighed with a digital balance of 0.001 accuracy after the drying period.
Experimental setup
The custom experimental setting (Fig. 1) consisted in a ureteral model (polymer tube 17 cm length, closed on one side, 7 mm diameter), with an opaque tape on a tray with saline. A different stone phantom and ureteral model were used for each test; every effort was made to assure that the laser lithotripsy conditions were kept accurate and homogeneous for all the tests.
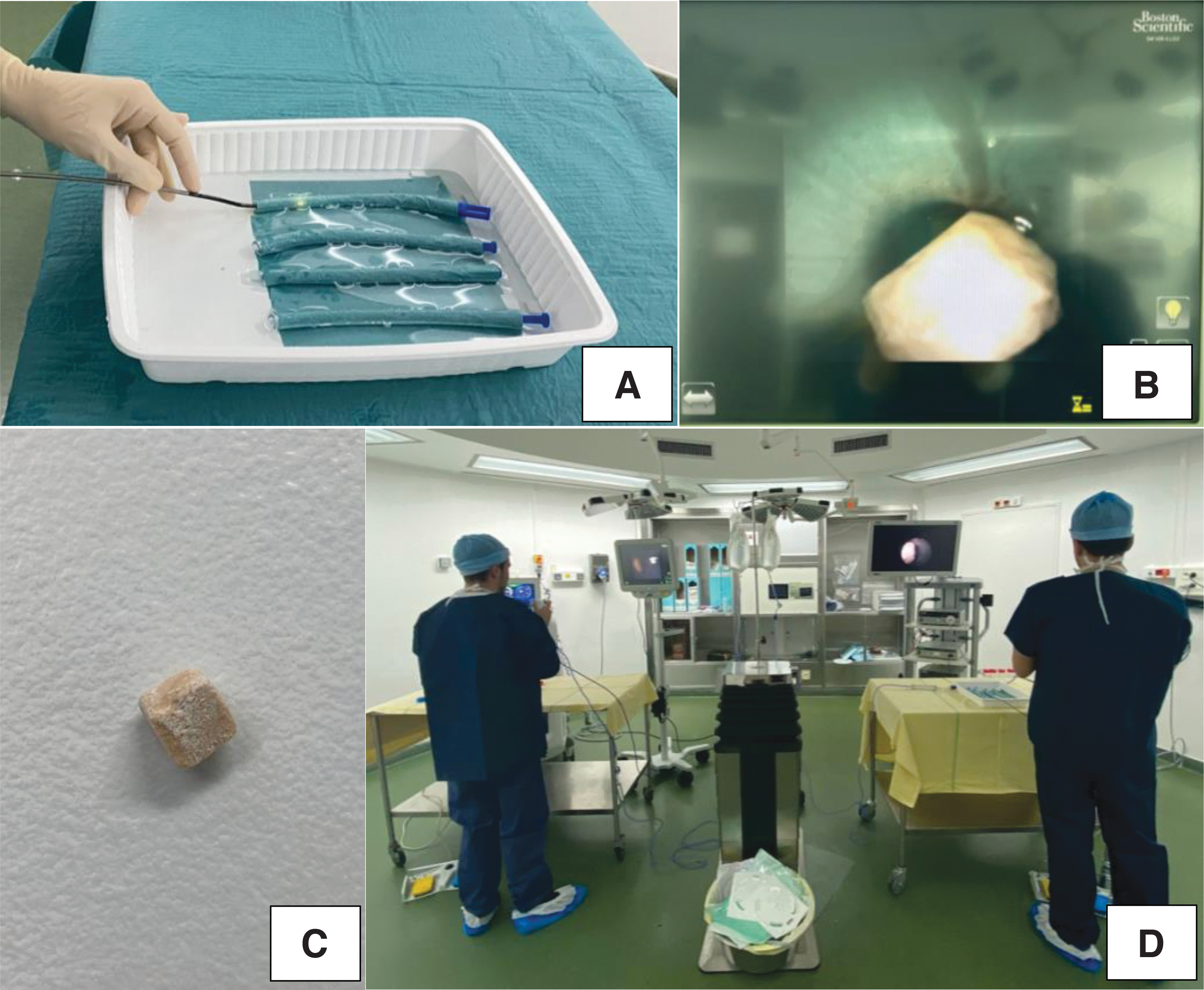
Experimental setup showing
Trials were conducted using an Olympus P5 (Olympus©, Japan) and a Lithovue (Boston Scientific©, Maple Grove, MN) as a fiber optic and digital flexible ureteroscope, respectively. Irrigation was ensured by a combination of a gravity irrigation at 40 cm H2O above the saline tray and a hand-assisted irrigation system providing on-demand forced irrigation to provide proper visibility (Fig. 1).
Participants were divided into two groups according to their skills (five junior and five experienced urologists with more than 100 URS per year). Each one performed 32 continuous lasering session (16 TFL and 16 Ho:YAG) of 5 minutes, with and without the transparent tip and with digital and fiberoptic ureteroscopes. All experiments were performed at room temperature (21°C).
Laser efficiency
Laser parameters were obtained from the laser. Data included laser settings, total energy (joules), and lasing time (seconds). Stone fragments were labeled and dried at room temperature (21°C). The stone ablation rate (AR) was calculated by dividing the weight difference (Artificial Stone Weight before the experiment [mg]−Artificial Stone Weight dried [mg]) with ablation time.
Assessment of ureteral lesions
Ureteral models were collected and labeled. Ureteral damage was classified in a scale (0–5) regarding burns and holes in its surface (Fig. 2). Plastic tubes were classified blinded according to the thermal impacts score by consensus between three authors (A.S.d.R., M.C., and M.K.). In Figure 3, there is the example of ureteral damage from a single surgeon.
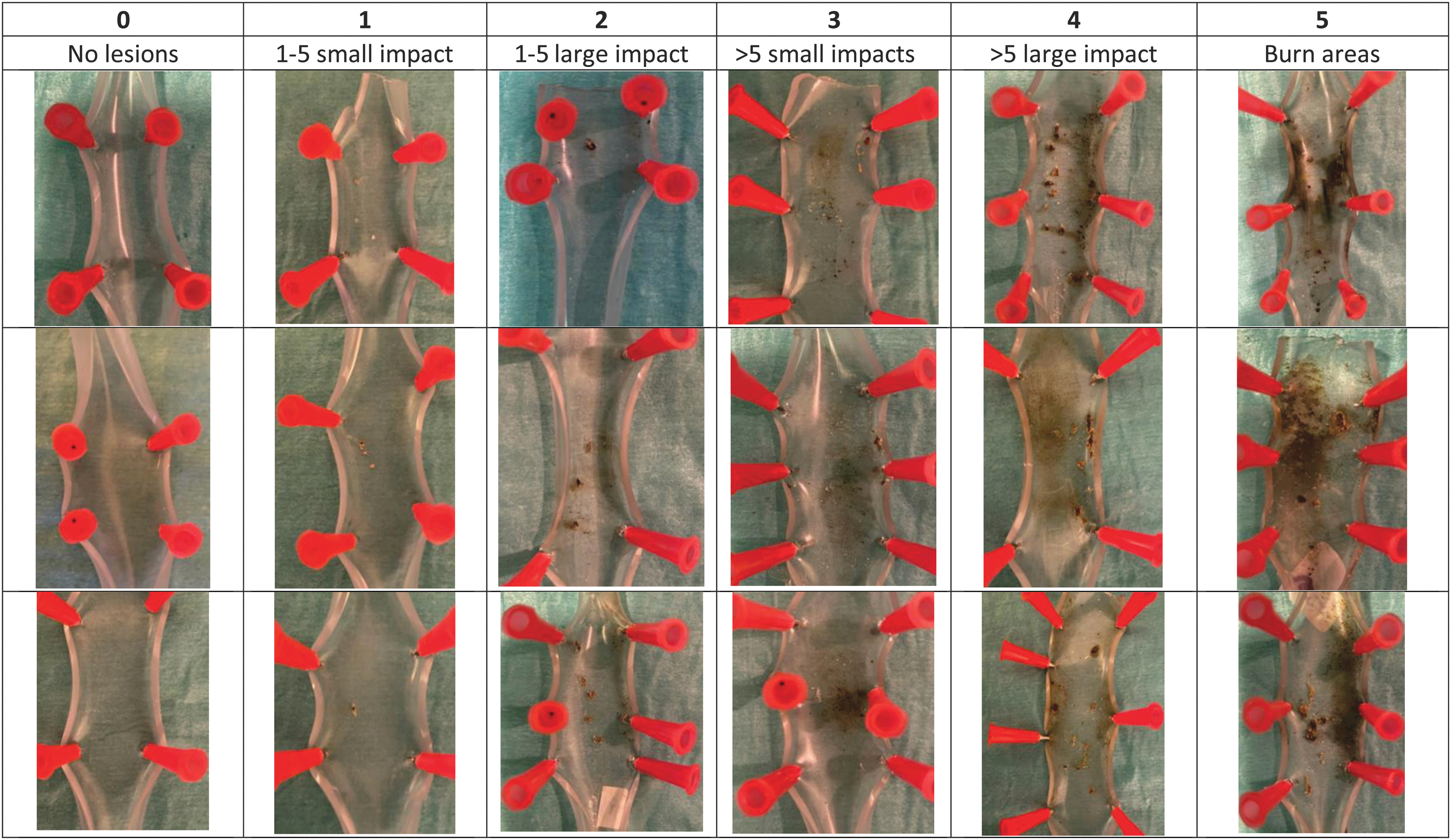
Ureteral damage classification. Score 0–5 according to burn and holes found in the plastics after lithotripsy. Color images are available online.
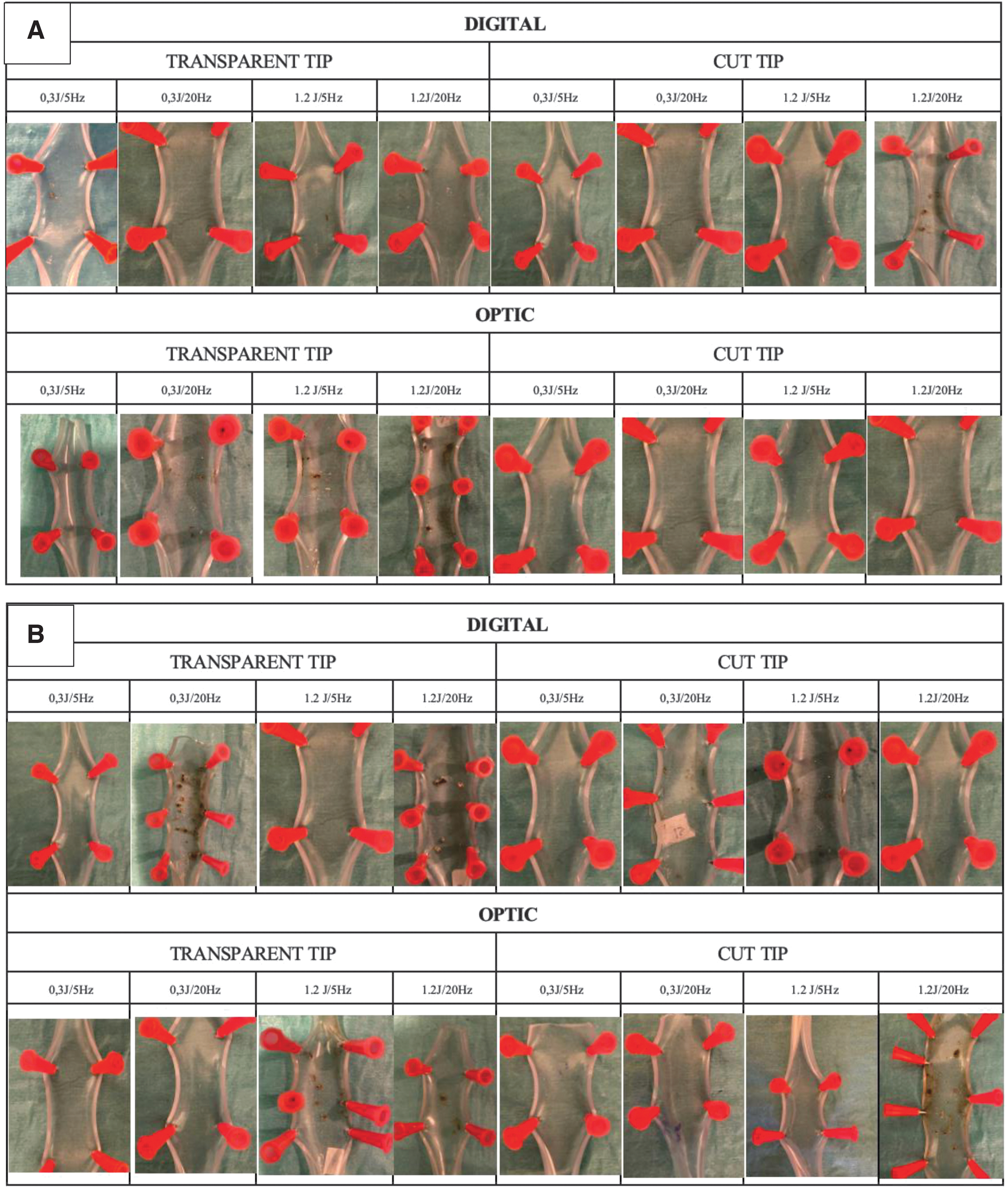
Ureteral damage results from a single surgeon with Ho:YAG
Statistical analysis
SPSS v25 software (IBM Statistics) was used for the statistical analysis. ARs of different laser settings and equipment were recorded and analyzed. For each cohort of laser generator, set of laser parameters, LF tip (transparent/cut), and flexible ureteroscope (optic/digital), 10 trials were performed. Results are presented as median with standard deviation. To assess laser efficiency, one-way analysis of variance (ANOVA) and T-student were used; for ureteral damage, Kruskal–Wallis test and Mann–Whitney U test were used. A p-value of 0.05 or less was considered significant.
Results
Laser efficiency
For both, Ho:YAG and TFL, there was no difference in overall mean total energy delivered between junior and senior urologists (for Ho:YAG p = 0.7; and for TFL p = 0.6) or in the overall mean total AR between junior and senior urologists (for Ho:YAG p = 0.7; and for TFL p = 0.6). Despite the laser source, there were marked differences according to the settings (p < 0.001); the HP (24 W) and the low-power (LP) (1.5 W) settings were associated with the higher and the lower delivered energy, respectively (Table 2).
Total Energy Delivered (KJ) by the Laser Fiber During 5 Minutes of Lithotripsy
FO = fiberoptic; Ho:YAG = holmium YAG; SD = standard deviation; TFL = Thulium fiber laser; TT = transparent tip; TTC = transparent tip cut.
In parallel, differences were also found regarding AR (p < 0.001); the more delivered energy the more AR (Table 3). When comparing both laser generators, there was no difference in overall mean total energy delivered between Ho:YAG vs TFL (p = 0.2); nevertheless, a significantly higher mean AR was observed with TFL than with Ho:YAG (0.5Δ mg/s ± 0.33 vs 0.39 Δmg/s ± 0.3, p = 0.002).
Ablation Rate in Each Scenario by Holmium YAG and Thulium Fiber Laser Fiber, During 5 Minutes of Lithotripsy Time
On the other hand, when comparing the two groups with 6 W (0.3 J at 20 Hz vs 1.2 J at 5), there was no difference in delivered energy for Ho:YAG (p = 0.6) or TFL (p = 0.2, and concerning AR, no difference was found for both lasers (p = 0.8).
Although there was no difference in total joules when comparing the tips in all tests (p = 0.8), a significantly higher mean AR was found with cut tip with TFL in the senior group (0.29 Δmg/s ± 0.23 vs 0.44 Δmg/s ± 0.36, p = 0.03). Higher mean delivered energy was observed in digital ureteroscopes when compared to fiberoptic (2 J ± 1.5 vs 1.7 J ± 1.2, p = 0.04), but no significantly difference was found in AR (p = 0.5).
Ureteral damage
Of the 320 analyzed ureteral models, 234 (73.1%) were lesions grade 0–1, there was no difference between laser generator (p = 0.9) (Table 4). Higher statistically significant ureteral damage was found in the junior urologist vs the experienced ones (p = 0.03); when analyzing per laser source, this difference was found in Ho:YAG (p = 0.006), but not in TFL (p = 0.07). Nevertheless, in TFL group, there are more low-grade lesions in senior group (62 vs 56) and less high-grade lesions (4 vs 7).
Thermal Injury Regarding Laser Settings (Scale 0–5)
Difference in grade of ureteral damage between junior urologists according to the setting group was observed in Ho:YAG (p = 0.006), but not in TFL (p = 0.07). Among senior urologists, differences were found for both, Ho:YAG (p = 0.04) and TFL (p = 0.03). Most of grade 4–5 lesions (64%) were found in HP laser settings and 95% of lesions in LP group were grade 0–1 (Table 4) for both lasers. There was no difference in a subgroup analysis between 6 W groups for Ho:YAG (p = 0.7) and TFL (p = 0.4).
However, for juniors, more lesions were found with 0.3 J/20 Hz than 1.2 J/5 Hz, for both Ho:YAG (p = 0.05) and TFL (p = 0.04). Moreover, there was a significant difference regarding type 2 and type 3 lesions; the 0.3 J/20 Hz had more grade 3 lesions (multiple small impacts), and the 1.2 J/5 Hz had more grade 2 lesions (less than five large impacts) in all tests (p = 0.04).
For all tests, there is no difference in ureteral damage between the transparent tip vs the cut tip (p = 0.9) or between fiberoptic scopes vs digital (p = 0.9).
Discussion
Laser efficiency
The experimental results highlight the essential aspects of Ho:YAG and TFL lithotripsy, including energy delivery, ARs, and safety. As expected, the AR increases as delivered energy increases, for both Ho:YAG and TFL. 14 –16 At first glance, this result implies that Ho:YAG and TFL ARs are enhanced by HP settings (24 W). However, there is no clear evidence that HP laser generators perform better than LP ones in terms of lithotripsy outcomes. A systematic review comparing high- and low-power laser lithotripsy found that HP laser lithotripsy appears to require shorter operative time, with similar stone-free and complication rates compared with LP traditional lithotripsy.
Nevertheless, when considering stone burden, this advantage seems to be lost, or at least not to be comparable with those observed in laboratory studies. 17 Regarding our results, the mean delivered energy increases four times, whereas the ARs only improve two times between LP and HP groups. Similar findings were reported by Mekayten et al where HP was able to reduce laser only time by a half compared with LP, despite the possibility of having as much as five times higher frequency and with an increased total amount of delivered energy. 18
This highlights the issue of laser efficiency in energy delivery. Although HP settings can have more stone AR and may reduce the operative time, there was no difference regarding laser efficiency between settings. Only TFL was more efficient compared to Ho:YAG. At the same energy and pulse frequency settings, the TFL device produces significantly lower retropulsion forces than the current Ho:YAG technology. 14,19 –21 This difference can be explained by different laser pulse shapes, different water absorption coefficients of laser, and different peak powers. 22
On the other hand, the equipment is essential to assure an adequate procedure. Although the superiority of digital scopes vs fiber optical scopes for laser lithotripsy is known, 23,24 a better laser efficiency was found with fiber optical scopes. In our experience, the digital scope was previously used, which might interfere with the vision quality, reducing the efficacy. In addition, cleaved tip was more efficient, only with TFL. This could be explained because of the quick consumption of the transparent tip with 1.2 J of pulsed energy in Ho:YAG. As described by Uzan et al, the degradation of the LF occurred for energy >1 J, regardless of the frequency, only in Ho:YAG laser, attributable to a burn back effect caused by a greater peak power for the short pulse durations. 25 However, because of the rising costs of flexible endoscopes, Ho:YAG fibers are also reliable fibers. 26
Ureteral damage
This study reports the in vitro consequences of thermal injury burn after direct contact of the laser emission on a ureteral model. According to our results, as delivered energy increases, thermal damage increases too. Those results were found for both, Ho:YAG and TFL. Thermal effects of Ho:YAG and TFL laser caused by the increase of temperature in irrigation fluids have already been well investigated. 11,17 However, in our study, irrigation was ensured by a combination of a gravity irrigation at 40 cmH2O above the saline tray and a hand-assisted irrigation system, so thermal impacts shown in ureteral models are not caused by the rise of temperature in the irrigation medium, but to an accidental thermal lasering lesion (except grade 5 lesions, which were attributable to lasering inside an air bubble). To our knowledge, this is the first time that the direct laser thermal effect is studied for both lasers.
When comparing expertise, as expected, more high-grade lesions were found in trainees' urologist. However, when analyzing per laser generator, differences were only found with Ho:YAG. The TFL has been reported to offer a better endoscopic view during lithotripsy. 3 The reduced retropulsion and consequent reduced medium turbulence could possibly be responsible for this, as less fragments and dust particles are swirled up, thereby reducing the “snow storm” effect that is characteristic of Ho:YAG lithotripsy. In addition, by producing less retropulsion, the TFL is also more readily operated by less experienced users, reducing the learning curve and the need to constantly adapt to a persistently changing stone position. 3
For both 6 W groups, as expected, there is no difference regarding delivered energy or ARs. However, multiple small impacts and few large impacts were found in 0.3 J at 20 Hz and 1.2 J at 5 Hz, respectively. The clinical impact of those different lesions is unknown. Nevertheless, we can presume hypothetically that a single large impact could be attributable to a burst of energy direct to the wall; on the contrary, higher frequencies can stochastically cause a higher number of fragments hitting the walls; this repeated microtraumatism could increase the risk of damage producing these multiple and small superficial lesions. Also, the higher the motility of stones and fragments, the lower the quality of endoscopic view. 4 In addition, considering skills, more lesions were found with high frequency in the junior urologist group, increasing the risk of ureteral damage.
Strengths and limitations
A particular strength of the study is that we determined real-life effectivity and safety. Nevertheless, the first limitation was an incomplete simulation of actual laser lithotripsy conditions in a urinary tract; convection and blood circulation play major roles in preventing thermal injury to tissues. 17,27 In addition, we do not know the clinical outcomes of those lesions. However, the aim of our study was to compare different settings and the impacts obtained. Stone phantoms were used rather than human stones. We required samples of approximately uniform mass, geometry, and composition, which could not be achieved practically with human stones.
The third limitation involved BegoStones immediately absorbing water through cracks and pores from the water, which would have influenced the results of dehydrated phantoms in water. It should also be mentioned that the so-called dry phantoms in our study had not been desiccated. However, we have a control stone that was submerged into the saline tray without lithotripsy treatment, and we stored in similar conditions; when its weight was the same as before the experiment, we assumed that the rest were dried too.
Besides adequate irrigation to reduce heat production, since the introduction of HP lasers, power should be considered more than ever as the most important adjustable parameter during laser lithotripsy. 28 A strategy of low pulse power to create tiny debris may produce slow lithotripsy, but may not seem as inefficient when weighed against time spent because of retropulsion and less thermal impacts.
Conclusions
If the ARs increase in the same way as the delivered energy, increasing the laser settings (pulse energy, pulse rate, and total power) exposes to a higher risk of ureteral damage. Same power settings produce different thermal lesions according to the pulse energy and rate. In unexperienced hands, high pulse rate settings produce more damage than high pulse energy. The clinical impact of these findings remains unknown, but this in vitro study highlights the importance of working at low power-low pulse rate to treat ureteral stones.
Footnotes
Authors' Contributions
A.S.d.R.: data collection and article writing. M.C.: data analysis and article writing. M.K.: data management. F.P.: article editing. A.P.: data collection. O.T.: project development and article editing.
Author Disclosure Statement
A.S.d.R., M.C., M.K., F.P., and A.P. have nothing to disclose. O.T. is a consultant for Boston Scientific, Coloplast, EMS, IPG, Quanta and Rocamed, but has no specific conflicts relevant to this work.
Funding Information
No funding was received for this article.