
Abstract
Objective:
To perform a systematic review to assess the incidence of transient (<6 months) and persistent (>6 months) stress urinary incontinence (SUI), urge urinary incontinence (UUI), and mixed urinary incontinence (MUI) after transurethral surgeries for benign prostatic hyperplasia.
Materials and Methods:
A systematic literature search was performed using Embase, PubMed, and Web of Science. We included studies comparing monopolar (M)/bipolar (B) transurethral resection of the prostate (TURP) vs ablation vs enucleation procedures. Incidence of incontinence was assessed using Cochran-Mantel-Haenszel Method and reported as odds ratio (OR), 95% confidence interval (CI), and p-values. Statistical significance was set at p < 0.05
Evidence Synthesis:
Twenty-eight studies were included. Incidence of transient SUI was 4.6%, 6.0%, 3.0%, and 2.4% after ablation, enucleation, M-TURP, and B-TURP, respectively. Incidence of persistent SUI was 1.1% after ablation, 1.7% after enucleation and M-TURP, and 1.0% after B-TURP. Incidence of transient UUI was 2.0%, 7.3%, 4.4%, and 2.8% after ablation, enucleation, M-TURP, and B-TURP, respectively. Incidence of persistent UUI was 2.2% after M-TURP. The incidence of transient MUI was 5.1%, 0.8%, 5.4%, and 0.9% after ablation, enucleation, M-TURP, and B-TURP, respectively. Incidence of persistent MUI was 3.1% after ablation and 4.8% after M-TURP. Incidence of transient and persistent SUI and UUI did not differ after TURP vs enucleation. Incidence of transient (OR 3.32, 95% CI 0.41–26.65, p = 0.26) and persistent SUI (OR 4.79, 95% CI 0.52–43.89, p = 0.17) was not significantly higher after ablation. Incidence of transient UUI was not significantly higher after ablation (OR 2.62, 95% CI 0.04–166.01, p = 0.65), whereas persistent UUI did not differ. Incidence of transient MUI was significantly higher after enucleation (OR 3.26, 95% CI 1.51–7.05, p = 0.003). Incidence of transient and persistent MUI did not differ after TURP vs ablation.
Conclusions:
Ablation, enucleation, and TURP have an impact on all forms of incontinence, but this is transient in most cases with no difference between the groups, except for MUI, which was higher after enucleation vs M-TURP.
Introduction
Benign prostatic hyperplasia (BPH) is the most common cause of lower urinary tract symptoms in middle-aged and elderly men. 1 When pharmacological treatments fail or bladder outlet obstruction (BOO) complications occur, surgery is recommended. 2 Transurethral resection of the prostate (TURP) and open prostatectomy have been the reference standard for many years. In the last three decades, open prostatectomy has been almost abandoned and TURP has been challenged by new transurethral enucleation and ablation techniques, which have been demonstrated to be equally effective or even better, but with less morbidity even in large prostate volume. 3,4
However, urinary incontinence has always represented one of the worst complaints affecting patients' quality of life after BPH surgery and underwhelming the outcomes of the original surgery. 5 Han et al. identified 411,658 men with BPH and among those who had surgery, 12.5% were diagnosed with postoperative incontinence. 6 However, the range in reported incontinence rates after transurethral surgery is wide and correlated to different operative techniques, surgeon experience, different definitions of incontinence, and patient-specific factors. In addition, most studies did not report the type of incontinence or its duration. Therefore, it is of utmost importance to assess the incidence of each form of incontinence (i.e., stress, urge, and mixed) and its duration (i.e., transient or persistent) because treatments change according to the nature of urine leakage.
This review aims to assess the incidence of transient and persistent stress urinary incontinence (SUI), urge urinary incontinence (UUI), and mixed urinary incontinence (MUI) after transurethral surgeries for BPH.
Evidence Acquisition
Aim of the review
This study aimed to systematically review the incidence of urinary incontinence after transurethral treatment of BPH. The main outcome was to evaluate for differences in the incidence of incontinence among different transurethral procedures. Urinary incontinence was categorized according to the type of leakage in stress, urge, and mixed incontinence. The secondary outcome was to assess the difference in baseline prostate volume, surgical time, and resected/enucleated prostatic tissue.
Literature search
This study was performed according to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework. A broad literature search was performed on December 20, 2021, using EMBASE, PUBMED, and WEB OF SCIENCE. Medical Subject Heading (MeSH) terms and keywords were used as follows: (urinary incontinence OR stress urinary incontinence OR postoperative incontinence) AND (prostatic hyperplasia OR BPH OR benign prostatic enlargement) AND (Prostate resection or Prostate enucleation or Prostate vaporization or monopolar transurethral or bipolar transurethral or MTURP or BTURP or plasmakinetic or PKRP or PKEP or PKERP or TURis or photovaporization or PVP or PVEP or holmium or HoLEP or thulium or ThuLEP or ThuVEP or diode or DiLEP or BTUEP or MTUERP). No date limit was imposed. The search was restricted to English articles only. Animal and pediatric studies were also excluded. This review was registered in PROSPERO (receipt no. 308879).
Selection criteria
The Patient Intervention Comparison Outcome Study type (PICOS) model was used to frame and answer the clinical question. Population: men with surgical indication for BPH; intervention: transurethral procedures; comparison: monopolar (M)-TURP/bipolar (B)-TURP; outcome: incidence of stress, urge, and mixed incontinence after surgery; and study type: randomized, prospective nonrandomized, and retrospective studies. Transurethral procedures were divided into two groups regardless of energy applied and according to the technique that was performed (enucleation and ablation). The enucleation group included Thulium fiber laser, Holmium laser, GreenLight Laser, Diode, Bipolar, and monopolar techniques. The ablation group included any laser vaporization technique, and bipolar/monopolar vaporization. The transurethral resection group consisted of monopolar and bipolar resection procedures. The incidence of urinary incontinence was categorized as transient (lasting ≤6 months) or persistent (lasting >6 months).
Study screening and selection
Two independent authors screened all retrieved records through Covidence Systematic Review Management®. A third author solved discrepancies. Studies were included based on PICOS eligibility criteria. Retrospective, prospective nonrandomized, and randomized studies were accepted. Studies not specifying the type of incontinence were excluded. Reviews, meeting abstracts, letters to the editor, case reports, and editorials were also excluded. The full text of the screened articles was selected if found relevant to the purpose of this study.
Statistical analysis
Baseline prostate volume, surgical time, and enucleated/resected prostatic tissue were pooled using the inverse variance of the mean difference (MD) with a random effect, 95% confidence interval (CI), and p-values. Incidence of stress, urge, and mixed incontinence was assessed using Cochran-Mantel-Haenszel Method with the random effect model and reported as odds ratio (OR), 95% CI, and p-values. Analyses were two tailed and the significance was set at p < 0.05 and a 95% CI. OR more than one indicates higher odds in the enucleation or ablation group. Study heterogeneity was assessed utilizing the I 2 value. Substantial heterogeneity was defined as an I 2 value >50%. Meta-analysis was performed using Review Manager (RevMan) 5.4 software by Cochrane Collaboration. The quality assessment of the included studies was performed using the Cochrane Risk of Bias tool, using RoB 2 for randomized studies and risk of bias in non-randomised studies of interventions (ROBINS-I) for nonrandomized ones.
Evidence Synthesis
The literature search retrieved 2660 articles. After removing 704 duplicated studies, 1956 studies were left for screening. Another 1852 articles were further excluded after the title and abstract screening because they were unrelated to the study purpose. The full texts of the remaining 104 studies were screened and 76 articles were further excluded. Finally, 28 studies were accepted and included for meta-analysis. Eighteen studies compared enucleation vs TURP (Table 1). 7 –24 Ten studies compared ablation vs TURP (Table 2). 25 –34 Supplementary Figure S1 shows the 2020 PRISMA flow diagram.
Characteristics of Included Studies Comparing Enucleation vs Transurethral Resection of the Prostate
BEP = bipolar enucleation of the prostate; BPH = Benign Prostatic Hyperplasia; B-TURP = bipolar TURP; DiLEP = diode laser enucleation of the prostate; HoLEP = holmium laser enucleation of the prostate; IPSS = International Prostatic Symptoms Score; LUTS = lower urinary tract symptoms; MEP = monopolar enucleation; M-TURP = monopolar TURP; PSA = prostate-specific antigen; PV = prostate volume; PVR = postvoiding urine residual; Qmax = Maximum flow rate; RCT = randomized clinical trial; TFL = thulium fiber laser; TURP = transurethral resection of the prostate.
Characteristics of Included Studies Comparing Ablation vs Transurethral Resection of the Prostate
B-VAP = bipolar vaporization of the prostate; GLL = Greenlight laser vaporization; ILC = interstitial laser coagulation; M-VAP = monopolar vaporization; PVP = photovaporization of the prostate.
Study quality assessment
Supplementary Figure S2 shows the details of quality assessment for retrospective and prospective nonrandomized studies. 8,9,14,15,24,31,32 One study showed a low overall risk of bias. Three studies showed a critical overall risk of bias. One study showed a high overall risk of bias and the remaining two studies had a moderate overall risk of bias. The most frequent reason for bias was attributable to the selection of patients, followed by confounding and measurement of the outcome.
Supplementary Figure S3 demonstrates the details of quality assessment for randomized studies. 7,10 –13,16 –23,25 –30,33,34 Ten studies showed a low overall risk of bias. Ten studies showed some concerns regarding the overall risk of bias and the remaining one had a high overall risk of bias. The most frequent reason for bias was bias from the randomized process that had no information in five studies, followed by bias owing to missing data.
Incidence of SUI
The pooled incidence of pure SUI in patients who underwent TURP, enucleation, and ablation is reported in Supplementary Figure S4. The incidence of transient SUI ranged from 0.8% to 30.0% (pooled rate 4.6%) in ablation, and it was 0.7% to 28.6% (pooled rate 6.0%), 0.6% to 25.0% (pooled rate 3.0%), and 0.7% to 16.0% (pooled rate 2.4%) in enucleation, M-TURP, and B-TURP, respectively.
The incidence of persistent SUI ranged from 0.8% to 5.67% (pooled rate 1.1%) in ablation, and it was 0.7% to 4.3% (pooled rate 1.7%), 1.0% to 5.8% (pooled rate 1.7%), and 0.7% to 1.4% (pooled rate 1.0%) in enucleation, M-TURP, and B-TURP, respectively (Supplementary Fig. S5).
Incidence of UUI
The pooled incidence of pure UUI in patients who underwent TURP, enucleation, and ablation is reported in Supplementary Figure S6. The incidence of transient UUI ranged from 0.8% to 50.0% (pooled rate 2.0%) in ablation, and it was 0.6% to 48.1% (pooled rate 7.3%), 0.9% to 35.4% (pooled rate 4.4%), and 0.5% to 50.0% (pooled rate 2.8%) in enucleation, M-TURP, and B-TURP, respectively.
The incidence of persistent UUI ranged from 1.6% to 3.3% (pooled rate 2.2%) in M-TURP (Supplementary Fig. S7). No patient complained of persistent UUI in ablation, enucleation, and B-TURP.
Incidence of MUI
The pooled incidence of MUI in patients who underwent TURP, enucleation, and ablation is reported in Supplementary Figure S8. The incidence of transient MUI ranged from 1.6% to 8.2% (pooled rate 5.1%) in ablation, and it was 0.6% to 3.3% (pooled rate 0.8%), 1.6% to 13.8% (pooled rate 5.4%), and 0.4% to 5.8% (pooled rate 0.9%) in enucleation, M-TURP, and B-TURP, respectively.
The incidence of persistent MUI ranged from 0.8% to 7.1% (pooled rate 3.1%) in ablation, and it was 1.6% to 11.9% (pooled rate 4.8%) in M-TURP (Supplementary Fig. S9). No patient complained of persistent MUI in enucleation and B-TURP.
SUI: enucleation vs TURP
Meta-analysis for 14 studies (855 enucleation and 856 TURP cases) showed that the incidence of pure and transient stress incontinence did not differ between the two groups (OR 1.40, 95% CI 0.82–2.40, p = 0.22) (Fig. 1A). There was no significant heterogeneity among the studies (I 2 27%). Subanalysis confirmed that the incidence was similar between M-TURP and enucleation (OR 1.32, 95% CI 0.72–2.45, p = 0.37) and B-TURP and enucleation (OR 1.67, 95% CI 0.68–4.13, p = 0.27).
Meta-analysis of incidence of stress incontinence in studies comparing enucleation vs TURP. TURP = transurethral resection of the prostate. Color images are available online.
Meta-analysis for nine studies (234 enucleation and 224 TURP cases) showed that the incidence of pure and persistent stress incontinence did not differ between the two groups (OR 1.33, 95% CI 0.50–3.51, p = 0.57) (Fig. 1B). There was no significant heterogeneity among the studies (I 2 0%). Subanalysis confirmed that the incidence was similar between M-TURP and enucleation (OR 0.65, 95% CI 0.17–2.40, p = 0.51) and higher in the B-TURP, but the difference did not reach significance (OR 3.19, 95% CI 0.75–13.53, p = 0.12).
UUI: enucleation vs TURP
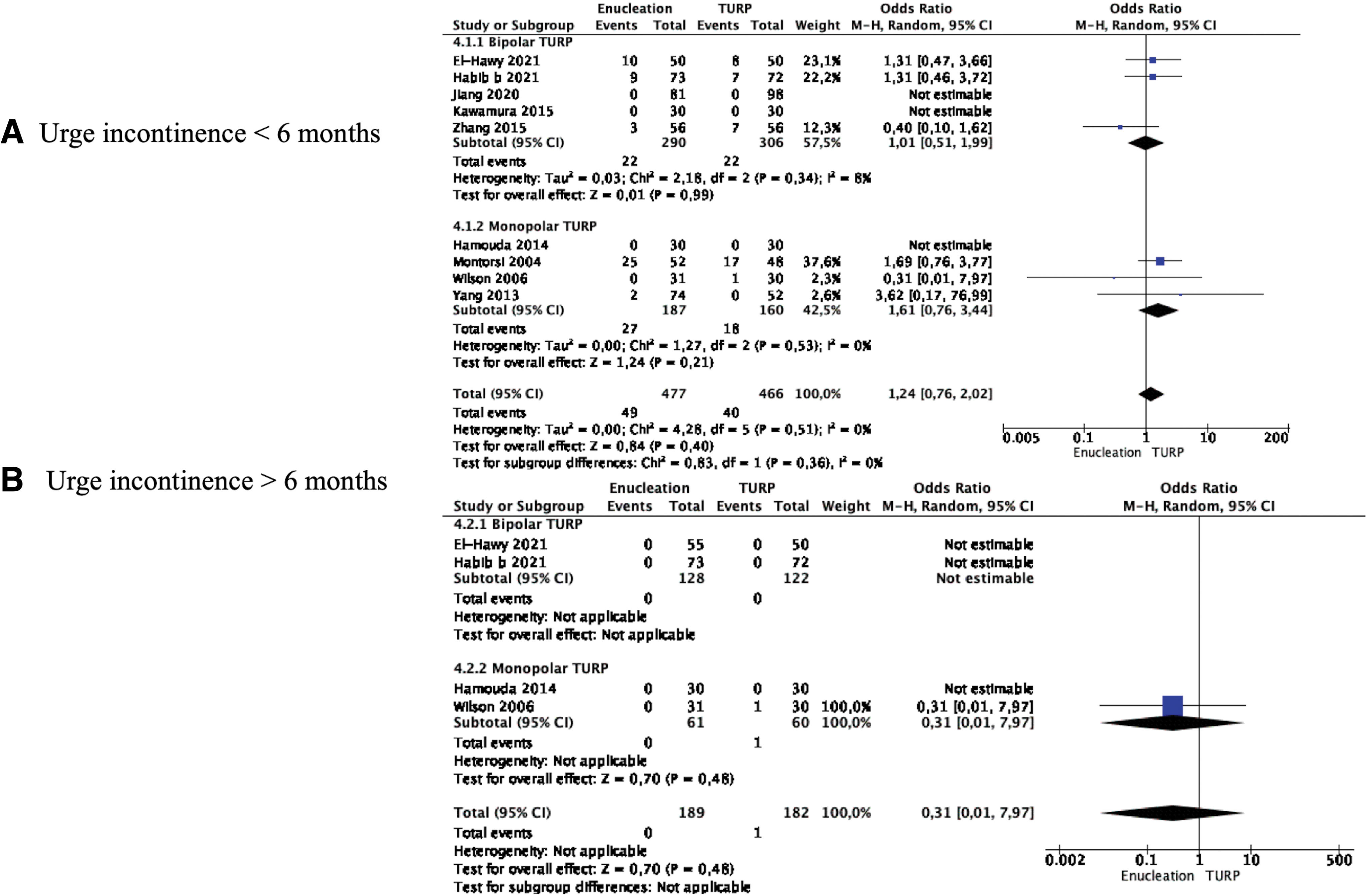
Meta-analysis for nine studies (477 enucleation and 466 TURP cases) showed that the incidence of pure and transient urge incontinence did not differ between the two groups (OR 1.24, 95% CI 0.76–2.02, p = 0.40) (Fig. 2A). There was no significant heterogeneity among the studies (I 2 0%). Subanalysis confirmed that the incidence was similar between M-TURP and enucleation (OR 1.61, 95% CI 0.76–3.44, p = 0.21) and B-TURP and enucleation (OR 1.01, 95% CI 0.51–1.99, p = 0.21).

Meta-analysis of incidence of urge incontinence in studies comparing enucleation vs TURP. Color images are available online.
Meta-analysis for four studies (477 enucleation and 466 TURP cases) showed that the incidence of pure and persistent urge incontinence did not differ between the two groups (OR 0.31, 95% CI 0.01–7.97, p = 0.48); this difference was related to the effect of the M-TURP group (Fig. 2B).
MUI: enucleation vs TURP
Meta-analysis for five studies (369 enucleation and 385 TURP cases) showed that the incidence of transient mixed incontinence was significantly higher in the enucleation group compared with the TURP group (OR 3.26, 95% CI 1.51–7.05, p = 0.003) (Fig. 3). There was no significant heterogeneity among the studies (I 2 0%). Subanalysis showed that the incidence was significantly higher in the B-TURP compared with the enucleation group (OR 3.27, 95% CI 1.48–7.23, p = 0.003).
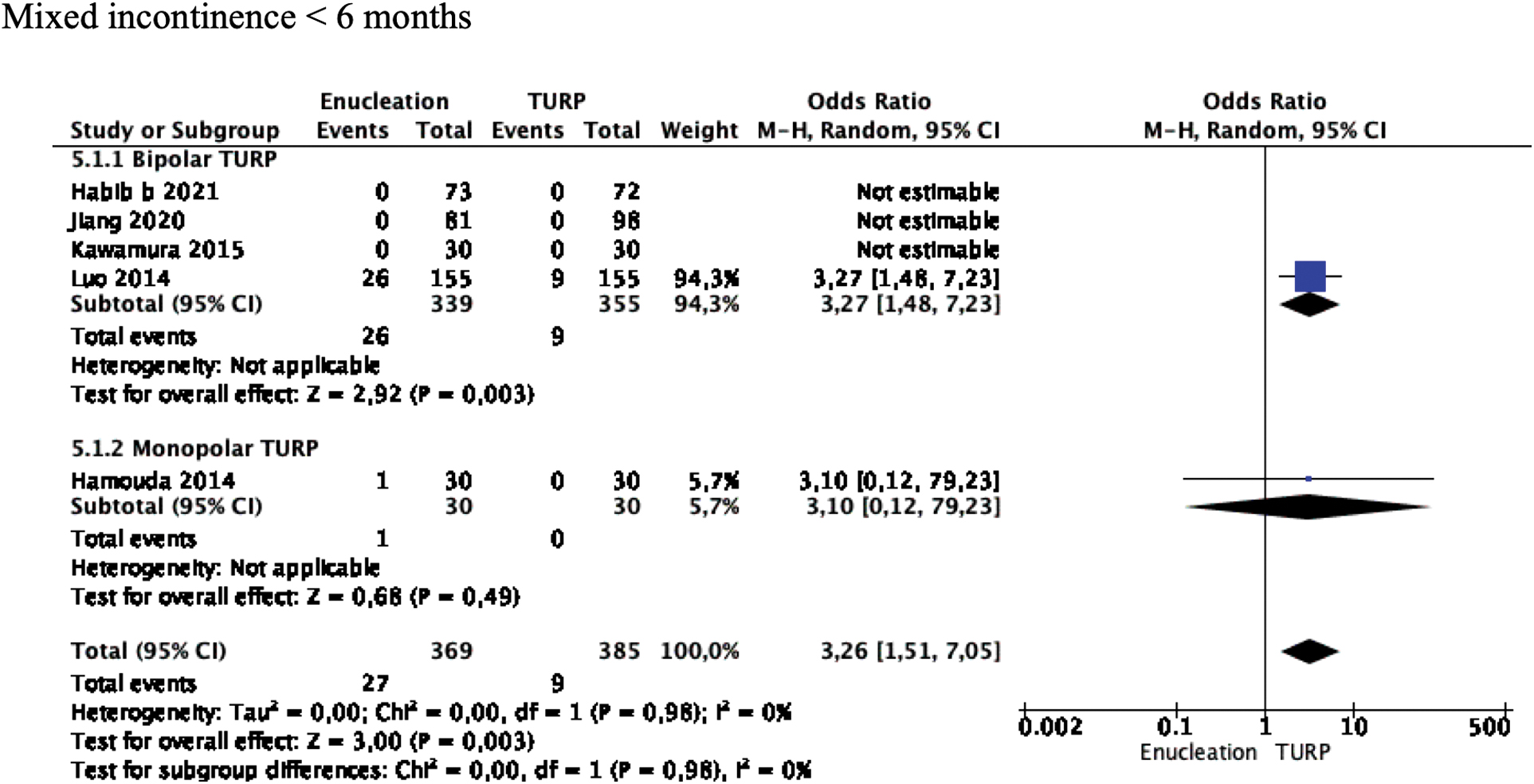
Meta-analysis of incidence of mixed incontinence in studies comparing enucleation vs TURP. Color images are available online.
No study reported cases of persistent mixed incontinence, making meta-analysis not feasible.
SUI: ablation vs TURP
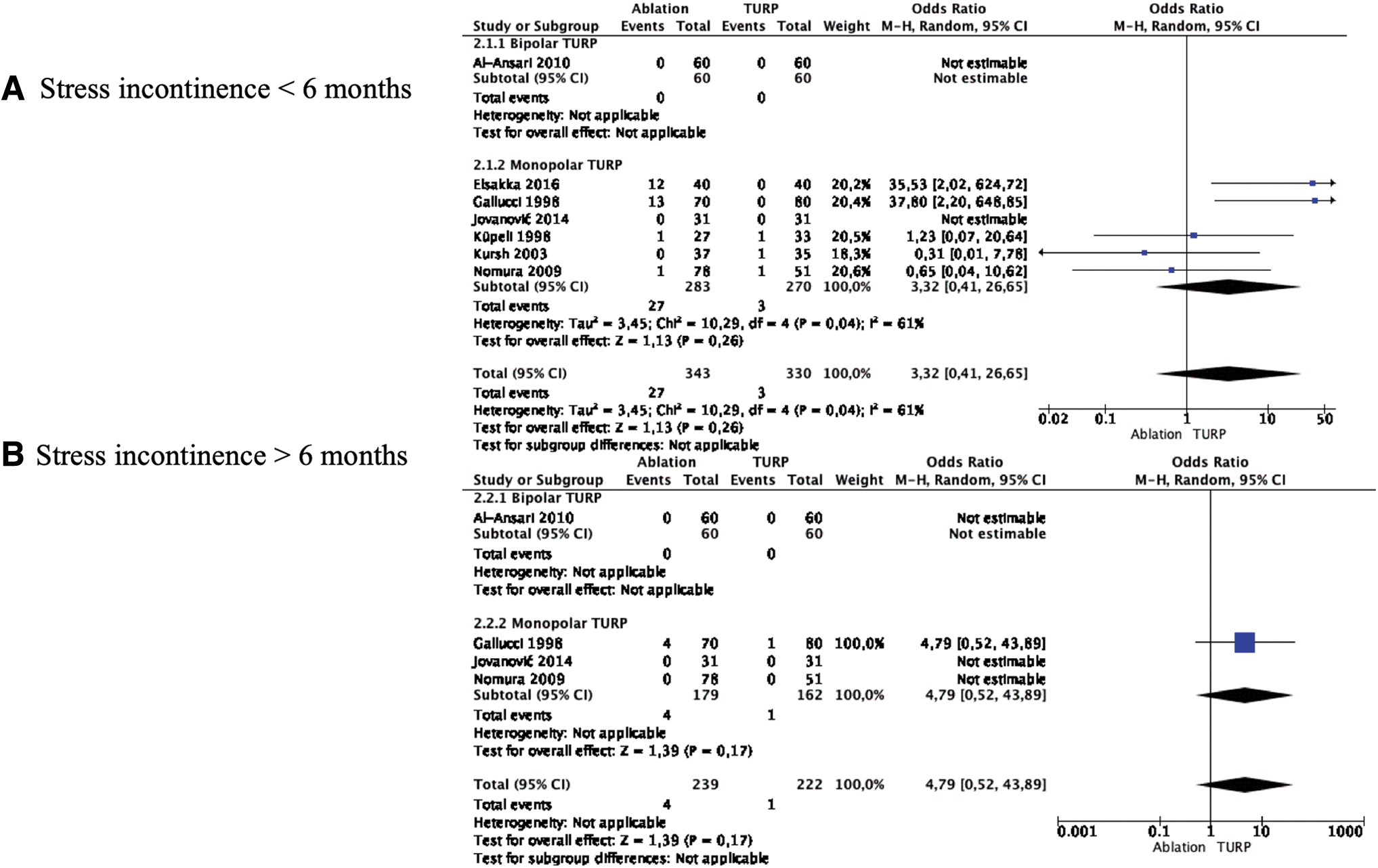
Meta-analysis for seven studies (343 ablation and 330 TURP cases) showed that the incidence of pure and transient stress incontinence was higher in the Ablation group, but the difference did not reach significance (OR 3.32, 95% CI 0.41–26.65, p = 0.26), and this difference was related to the effect of the M-TURP group (Fig. 4A). Heterogeneity among the studies was substantial (I 2 61%).

Meta-analysis of incidence of stress incontinence in studies comparing ablation vs TURP. Color images are available online.
Meta-analysis for four studies (179 ablation and 162 TURP cases) showed that the incidence of pure and persistent stress incontinence was higher in the ablation group, but the difference did not reach significance, and this difference was related to the effect of the M-TURP group (OR 4.79, 95% CI 0.52–43.89, p = 0.17) (Fig. 4B).
UUI: ablation vs TURP
Meta-analysis for four studies (107 ablation and 136 TURP cases) showed that the incidence of pure and transient urge incontinence was higher in the ablation group, but the difference did not reach significance, and this difference was related to the effect of the M-TURP group (OR 2.62, 95% CI 0.04–166.01, p = 0.65) (Fig. 5A). Heterogeneity among the studies was significant (I 2 71%).
Meta-analysis of incidence of urge incontinence in studies comparing ablation vs TURP. Color images are available online.
Meta-analysis for four studies (111 ablation and 121 TURP cases) showed that the incidence of pure and persistent urge incontinence did not differ between the two groups (OR 0.22, 95% CI 0.01–4.72, p = 0.33) (Fig. 5B). Subanalysis showed no incidence of urge incontinence in the B-TURP group.
MUI: ablation vs TURP
Meta-analysis for two studies (399 ablation and 169 TURP cases) showed that the incidence of transient mixed incontinence did not differ between the two groups (OR 0.56, 95% CI 0.30–1.02, p = 0.06) (Fig. 6A). There was no study in the B-TURP group.

Meta-analysis of mixed incontinence in studies comparing ablation vs TURP. Color images are available online.
Meta-analysis for three studies (270 ablation and 157 TURP cases) showed that the incidence of persistent mixed incontinence did not differ between the two groups and this difference was related to the effect of the M-TURP group (OR 0.57, 95% CI 0.27–1.18, p = 0.13) (Fig. 6B).
Meta-analyses of baseline prostate volume and surgical time: ablation vs TURP
Meta-analysis from nine studies (974 ablation and 478 TURP cases) showed that the mean baseline prostate volume did not differ between the groups (MD 1.10 mL, 95% CI −2.42 to 5.22, p = 0.54). Study heterogeneity was substantial (I 2 91%) (Supplementary Fig. S10A)
Meta-analysis from eight studies (1025 ablation and 517 TURP cases) showed that there was a trend for a longer operative time in the ablation group, but the difference did not reach significance (MD 2.24 minutes, 95% CI −1.62 to 6.11, p = 0.26). Study heterogeneity was substantial (I 2 79%) (Supplementary Fig. S10B). Subgroup analysis showed a significantly shorter time in the B-TURP group compared with the ablation group (MD 11.16 minutes, 95% CI 5.52–16.81, p < 0.0001).
Meta-analyses of baseline prostate volume, surgical time, and enucleated/resected tissue: enucleation vs TURP
Meta-analysis from 18 studies (317 enucleation and 284 TURP cases) showed that the mean baseline prostate volume did not differ significantly between the groups (MD 37.54 mL, 95% CI −31.08 to 106.13, p = 0.26). Study heterogeneity was substantial (I 2 100%) (Supplementary Fig. S11A). Subgroup analysis confirmed no difference.
Meta-analysis from eight studies (1025 ablation and 517 TURP cases) showed that there was a trend for a shorter operative time in the TURP group, but the difference did not reach significance (MD 8.99 minutes, 95% CI −0.09 to 18.07, p = 0.05). Study heterogeneity was substantial (I 2 98%) (Supplementary Fig. S11B). Subgroup analysis showed a significantly shorter time in the M-TURP group compared with the enucleation group (MD 8.86 minutes, 95% CI 4.10–13.63, p < 0.0001).
Meta-analysis from 16 studies (1123 enucleation and 1104 TURP cases) showed that the mean weight of removed tissue was significantly higher in the enucleation group (MD 9.17 g, 95% CI 6.88–11.46, p < 0.00001). Study heterogeneity was substantial (I 2 82%) (Supplementary Fig. S11C). Subgroup analysis confirmed that the mean weight of resected tissue was significantly lower in B-TURP (MD 10.85 g, 95% CI 7.95–13.75, p < 0.00001) and M-TURP group (MD 5.40 g, 95% CI 2.71–8.08, p < 0.00001) compared with the enucleation group.
Discussion
Despite advancements in technology and refinements in surgical procedures, urinary incontinence is still a common and distressful event after BPH surgery. Given the large number of BPH surgery performed worldwide, and the emotional and financial burdens associated with urinary incontinence, gaining insight into its incidence after transurethral surgery is clinically significant for both surgeon and patient counseling. Urinary incontinence after BPH surgery can be caused by a persistent or new onset of bladder dysfunction (urge-incontinence), an abnormality of the bladder outlet attributable to injury of the sphincter mechanism (stress incontinence), or a combination of both (mixed incontinence). 35
To the best of our knowledge, our review was the first study that assessed the rate and difference in the incidence of all types of urinary incontinence in studies comparing TURP vs enucleation vs ablation (Supplementary Fig. S12). We showed that both pure transient and persistent stress incontinence had the highest rate after enucleation (6% and 1.7%, respectively) and the lowest after B-TURP (2.4% and 1.0%, respectively). However, the incidence did not differ significantly in studies comparing enucleation vs TURP within and after 6 months after surgery. Conversely, ablation had a higher incidence of transient and persistent stress incontinence compared with TURP, but the difference did not reach significance. The low rate of persistent stress incontinence after all procedures demonstrates that regaining continence is time related and most patients can recover their continence spontaneously within a few weeks.
This also proves that stress incontinence is not always correlated to damage of the external sphincter muscle as is commonly perceived. Continence in men is a complex mechanism and the activity of the external (striated) sphincter is not solely responsible for continence that is preserved even after inducing paralysis of the striated sphincter. 36 The muscular and elastic tissue in the distal third of the prostatic urethra may play a pivotal role in maintaining the continence and damage of this urethral segment may be accountable for stress incontinence after BPH surgery. 37 Indeed, Cheng et al. found in a randomized trial comparing B-TURP and Greenlight laser enucleation that capsular perforation and stress incontinence were higher, although not significantly, in the enucleation group and suggested that saving some of the urethral mucosa at the prostate apex helped avoid incontinence. 8
Potential risk factors for both capsular perforation and incontinence included large prostate volume, tissue weight enucleated, and surgeon's experience with longer operative times and suboptimal vision. 8,38 However, other authors found that capsular perforation was most common in small prostates where the dissection plane was more difficult to find because the plane between adenoma and the surgical capsule was less recognizable. 39 Therefore, great attention must be taken to avoid prostatic capsule perforation, particularly at the level of prostatic apex with appropriate use of the resectoscope beak and repeated orientation during enucleation.
Our analysis confirmed that the mean weight of removed tissue was significantly higher in the enucleation group. This results in the common finding of a larger prostatic fossa after enucleation caused by the more complete adenoma removal compared with TURP that was found to be significantly associated with persistent stress incontinence after holmium laser enucleation of the prostate (HoLEP). 40
In addition, a larger prostatic fossa can lead to the trapping of urine and easier leakage not only with stress maneuvers (loss of urethral resistance) but also after detrusor contractions correlated to the change in bladder response to filling as a consequence of altered feedback from the prostatic fossa. 41 This also explains why the pooled incidence of transient urge incontinence was higher in our analysis after enucleation compared with ablation and TURP. Indeed, it is usually difficult in clinical practice to correctly identify pure stress and pure urge incontinence that is mostly mixed in patients undergoing enucleation.
Another important argument in favor of the role of the distal prostatic urethra in maintaining continence after BPH surgery, particularly after enucleation, is the application of the early apical release technique. The latter consists in the preservation of the external sphincter mucosa avoiding it to unstick from the striated sphincter through a complete demarcation of the apex from the sphincter. 42,43 Compared to the traditional three-lobe technique, the early apical and en bloc approach showed a significantly lower incidence of transient stress incontinence (13.5% vs 4.5%, p = 0.03), but the difference was not significant at the 6-month follow-up (4.9% vs 2.3%). 44 In addition, sustained stretching and traction at the apex level to reach the capsule during anterior and lateral enucleation may damage the so-called musculus sphincter urethrae glaber that runs underneath the striated sphincter and close to the mucosa. 42
Indeed, the striated muscle fibers of the external sphincter intermingle with the smooth muscle fibers of the prostatic urethra and have been shown to be inseparable from each other. 45 This concept sustains the importance of preserving the muscular and elastic tissue of the distal third of the prostatic urethra in maintaining postoperative continence. The decrease of incontinence rates with the early apical release technique and other techniques that recognize the importance of protecting the sphincter mucosal lining can influence incontinence rates of enucleation in the future, making it a more attractive option.
The importance of the distal urethra is also evident during ablation, where care should be taken to produce an adequate working channel and avoid vaporizing/ablating anterior tissue near the verumontanum because a deep penetration into the tissue layer of the external sphincter may produce stress incontinence, particularly using high-intensity system lasers. 46 Moreover, attention should also be taken to the apex, where the power should be lowered, and leaving a small flap of apical tissue might help avoid stress incontinence, particularly in the elderly. 47
Regarding urge incontinence, our study revealed that ablation had the lowest rate of transient urge incontinence (2.0%), whereas enucleation had the highest (7.3%). Moreover, urge incontinence is mostly transient. Indeed, persistent urge-incontinence was only reported in M-TURP, even if some grade of persistent urgency might be present after ablation because the rate of persistent mixed incontinence was 3.1% in our study. De novo or persistent bladder dysfunctions, such as detrusor overactivity, impaired or absent detrusor contractility, and low bladder compliance, are considered the main factors correlated to postoperative urge incontinence. The high incidence of urge incontinence after enucleation can be explained by several pathophysiological mechanisms.
Prostatic fossa healing reaction, urinary tract infection, thermal/electrocautery injury of the prostatic capsule by excessive energy, bladder wall damage, and detrusor overactivity caused by long-lasting BOO are the most quoted causes of postoperative urge incontinence. 5,48 Bleeding during surgery and longer operative time usually give an unclear vision, which may increase the risk of misfiring during TURP and false dissection during enucleation with an increasing risk of electrocautery/thermal damage. This might explain why M-TURP was found to be the only procedure associated with persistent pure urge incontinence in our analysis.
Notably, we also found that the incidence of urge incontinence did not differ between TURP vs ablation vs enucleation, even if there was a trend for a higher incidence of transient incontinence after ablation compared to TURP. This finding is in line with the concept of structural and functional change of the detrusor muscle attributable to BOO and the persistence of urgency after BOO relief. BOO showed a neurotrophic effect on the detrusor muscle with hypertrophy of bladder neurons, which can facilitate the micturition reflex. 49 In addition, BOO can also produce damage to the urothelium with a consequent increase of epithelial cell permeability to mediators that contribute to increased bladder afferent activity. 50
Age-related detrusor dysfunction and BOO have a synergistic effect on the bladder producing increased glycolysis and production of free radicals with subsequent free-radical damage and decreased antioxidant defenses, and concomitant increased extracellular collagen/elastin deposition, increased work demand, and increased energy use. 51 These effects convert into detrusor overactivity, diminished bladder capacity, and compliance. Therefore, these modifications might require time to restore, at least in part, the bladder function after BOO relief. Finally, bladder mucosa injury during morcellation was found to be significantly associated with de-novo urge incontinence after HoLEP, suggesting that hemostasis and continuous irrigation of fluid during morcellation are a crucial part of the procedure to keep the view clear and avoid bladder damage. 52
This study is not devoid of limitations. First, the learning curve of involved surgeons was not commonly reported and this might have biased the rate of incontinence, but a truly unbiased comparison among procedures is well-nigh impossible. Second, preoperative and/or postoperative urodynamics was not routinely performed by most of the included studies and the role of preoperative bladder dysfunctions in the incidence of postoperative incontinence was not assessed. Third, our results might not reflect the actual incidence of urinary incontinence in patients with large and very large size prostate because open and robotic simple prostatectomy were not included, even if many studies comparing enucleation vs TURP included patients with medium-large size prostate volume. Fourth, the evaluation of the influence of preoperative incontinence on postoperative continence was not feasible because these data were not available in 23 studies.
However, two studies reported that some patients regained their continence after surgery, demonstrating that bladder outlet relief probably settled preoperative urgency. 13,34 Finally, no data were reported on the predominant type of incontinence in studies reporting mixed incontinence and an actual incidence of urge and stress incontinence after ablation and M-TURP cannot be calculated.
Conclusion
In this study, we compared transurethral enucleation and ablation procedures against TURP to estimate the incidence of urinary incontinence after surgery. We found that all forms of transurethral interventions have a transient effect on the different types of incontinence with M-TURP causing persistent UUI. There was no correlation between incontinence with operative duration and prostate volume, despite the enucleation cohort having a significantly higher resected total weight. Our findings can help guide urologists in counseling their patients on the expected incontinence outcomes based on the surgical intervention offered.
Footnotes
Authors' Contributions
Conception and design: D.C. Acquisition of data: D.C., E.R., A.F., M.M., M.L.W., J.Y.-C.T., G.M.P., M.G., M.P.P., and V.G. Statistics: D.C. Drafting of the article: D.C., E.R., A.F., M.M., M.L.W., G.M.P., M.G., M.P.P., and V.G. Critical revision for important intellectual content: F.G.-S., A.B.G., and J.Y.-C.T. All authors participated in article writing, review, and approval of the final version of the article for submission.
Author Disclosure Statement
F.G.-S. is a consultant for Quanta system and Lumenis. The remaining authors declare no conflict of interests.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Figure S9
Supplementary Figure S10
Supplementary Figure S11
Supplementary Figure S12
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.