
Abstract
In the last two decades, surgical techniques for intracorporeal urinary diversion have been developed with the aim of reducing surgical morbidity. Although increasing constantly, the numbers of urologists offering intracorporeal neobladder reconstruction remain limited due to the complex nature of the procedure. In this article, we aim to provide a detailed description of the surgical technique we currently use at our institution. This technique was initially developed and perfected at the Karolinska Institutet in Sweden starting in 2003. It is a reproducible surgical approach with standardized and well-defined surgical steps. We give a detailed description of the surgical steps and provide tips and tricks to address specific situations and to increase efficiency. We also review the indications, the preoperative considerations, equipment necessary, postoperative considerations, and clinical outcomes for this procedure. Finally, we provide an accompanying didactic surgical video. We believe that this standardized approach can be learned and reproduced safely by motivated robotic surgeons.
Featured Video
https://stream.cadmore.media/player/2df9a6f6-4405-4a3e-b921-8d28ad4cc627

Introduction
Radical cystectomy with bilateral pelvic lymph node dissection and urinary diversion is most commonly performed in the context of muscle invasive bladder cancer and high-risk non-muscle invasive bladder cancer.
Multiple urinary diversion options have been used following cystectomy including continent and incontinent cutaneous urinary diversions in addition to orthotopic neobladder. In recent years, there has been an increase in the use of intracorporeal urinary diversion in specialized centers with the aim of reducing surgical morbidity, but it remains only offered by a limited number of urologists due to the complex nature of the procedure. 1 Although different intracorporeal neobladder reconstruction techniques have been described, none has been clearly shown to be superior. 2,3 In this article and in the accompanying video (Supplementary Data S1), we aim to provide a detailed description of the surgical technique we currently use at our institution. This technique was initially developed and perfected at the Karolinska Institute in Sweden starting in 2003. It is a reproducible surgical approach with standardized and reproducible surgical steps.
Indications
Patient preference is a major factor in selecting candidates for intracorporeal neobladder reconstruction. Other important factors to consider include age, cognitive function, dexterity, comorbidities, presence of urethral disease, and previous intestinal surgeries. Severe hepatic dysfunction and short bowel syndrome are absolute contraindications to a neobladder. Although this has been challenged, positive intraoperative urethral frozen section is considered a contraindication by most authors. 4 –7 In the case of a urethral frozen section positive for carcinoma in situ, we resect the proximal part of the urethra robotically and follow-up with clinical surveillance of the urethra without performing an immediate radical urethrectomy. We do not routinely perform intraoperative ureteral frozen section.
Impaired renal function is a relative contraindication due to the risk of metabolic acidosis and electrolyte imbalance but no clear cutoff has been established. 8 –10 We consider patients with estimated glomerular filtration rate of 30 mL/min and above as potential candidates for neobladder reconstruction, especially if preoperative hydronephrosis is present and contributes to kidney dysfunction. 10 Previous pelvic radiation is not an absolute contraindication to a neobladder reconstruction as it has been shown that it can be performed safely and with similar functional outcome in highly selected patients. 11,12
Preoperative Preparation
Principles of enhanced recovery after surgery (ERAS) are applied in the preoperative period. 13 Although patients are instructed to limit fiber intake in the days leading up to surgery, no strict diet restrictions are imposed. The use of bowel preparation is not necessary. 13 –16 We suggest that a potential stoma site also be marked by a specialized nurse before surgery. The marked site would be used for stoma placement in the unlikely event that the neobladder reconstruction cannot be performed either due to technical limitations or positive urethral frozen section during the surgery. Premedication with 1 g of acetaminophen, 600 mg of gabapentin, and 600 mg of celecoxib is given before surgery and quadratus lumborum block with local anesthetic is performed after induction of anesthesia as part of our non-opioid protocol. 17 Patients should also receive appropriate antibiotic prophylaxis before skin incision. 18 After institutional review of local pathogens, our protocol includes administration of IV gentamycine, ampicillin-salbactam, and fluconazole before incision with the ampicillin-sulbactam being continued for 24 hours.
Patient Positioning
The patient is placed in supine position with arms tucked to the side. In female patients, placing the legs in a frogged-leg position can allow easier access to the vagina during the surgery. Alternatively, the patient can be placed in lithotomy position that also allows docking the robot between the legs. All pressure points are carefully padded. We use The Pink Pad® (Xodus Medical, New Kensington, PA, USA) to prevent the patient from moving when the table is place in steep Trendelenburg position. The surgical field, including the genital organs, is prepped and draped in a standard fashion and the table is brought to a 25°–30° Trendelenburg position. The robot can be brought from the left side of the patient (Xi system) or from between the legs (Xi or Si systems).
Instrumentation
Robotic instruments required for intracorporeal neobladder reconstruction include the Monopolar Curved Scissors, Maryland Bipolar Forceps, Cardiere Forceps, Large Needle Driver, and the Grasping Retractor (Intuitive Surgical, Sunnyvale, CA, USA). We prefer to use the Cardiere Forceps as it has a lower grasping force than the Prograsp Forceps, thus reducing the risk of intestinal or mesenteric trauma during bowel manipulation. For suturing, only one robotic large needle driver is usually used in the right arm while the Maryland bipolar is used in the left arm. This configuration limits the number of instrument changes needed during the surgery, thus increasing efficiency while also decreasing the cost of the surgery.
We use the EndoGIA™ Ultra universal stapler (Medtronic, Dublin, Ireland) to perform the intestinal anastomosis. A total of four 60 mm and one 45 mm articulating reloads of Tri-Staple™ size Vascular/Medium are necessary.
Specialized suture necessary for the reconstruction include two 0–3 bidirectional barbed sutures 16 cm × 16 cm on RB1 needles (Stratafix™; Ethicon, Raritan, USA) and 4 to 5 single armed 6 inches 3-0 barbed sutures on CV23 needles (V-Loc™; Covidien, Dublin, Ireland).
Two 6F single J ureteral stents and a 20F or 22F two-way urethral catheter with large evacuation holes are also necessary to ensure adequate urine drainage.
For the reconstructive part of the surgery, the bedside assistant uses a long-tip suction, a fenestrated grasper, and laparoscopic needle driver. Electrocautery device such the LigaSure™ (Medtronic, Dublin, Ireland) and long laparoscopic clip applier are not specifically needed for intracorporeal neobladder reconstruction but are available as they are used for the extirpative part of the surgery.
Surgical Steps
Port placement
Abdominal insufflation is obtained using the Veres needle and the initial robotic port is introduced in the midline 5 cm above the umbilicus (Fig. 1). The camera in introduced and the abdomen is inspected. The remaining ports are introduced under direct vision. The right and left robotic ports are each placed ∼6–7 cm lateral to the umbilicus. A 15 mm port is place two fingerbreadths above and medial to the left anterosuperior iliac spine and the fourth robotic trocar is introduced through it. This port is also used for the introduction of the specimen bag and for the endoscopic stapler. Finally, two 12 mm assistant ports are placed on each side of the right robotic arm.
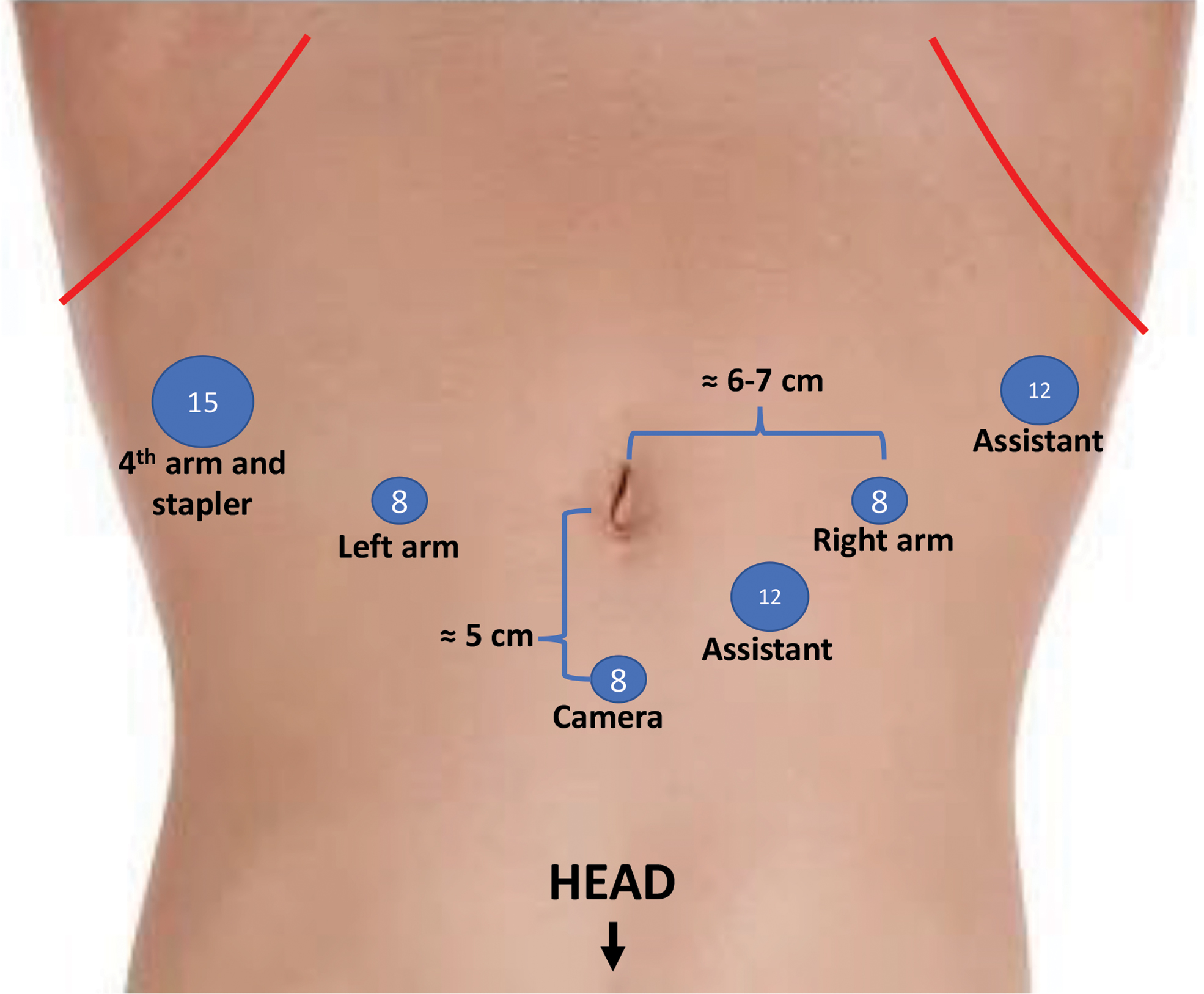
Port placement for robot-assisted radical cystectomy with intracorporeal neobladder reconstruction.
Urethral anastomosis
Once the extirpative portion of the surgery is completed, the left ureter is brought to the right side under the sigmoid mesentery in preparation for the ureteral anastomosis (Fig. 2A). Reducing the steepness of the Trendelenburg can be considered at this point to facilitate mobilization of the ileum toward the pelvis but is usually not necessary. Using the Grasping Retractor in the right arm and the Cardiere in the fourth arm, a segment of ileum 20–30 cm proximal to the ileocecal valve is brought down in the pelvis near the urethral stump and held in place by holding the mesentery with the Cardiere. Care is taken to limit direct grasping of the bowel with the Cardiere forceps to avoid trauma.
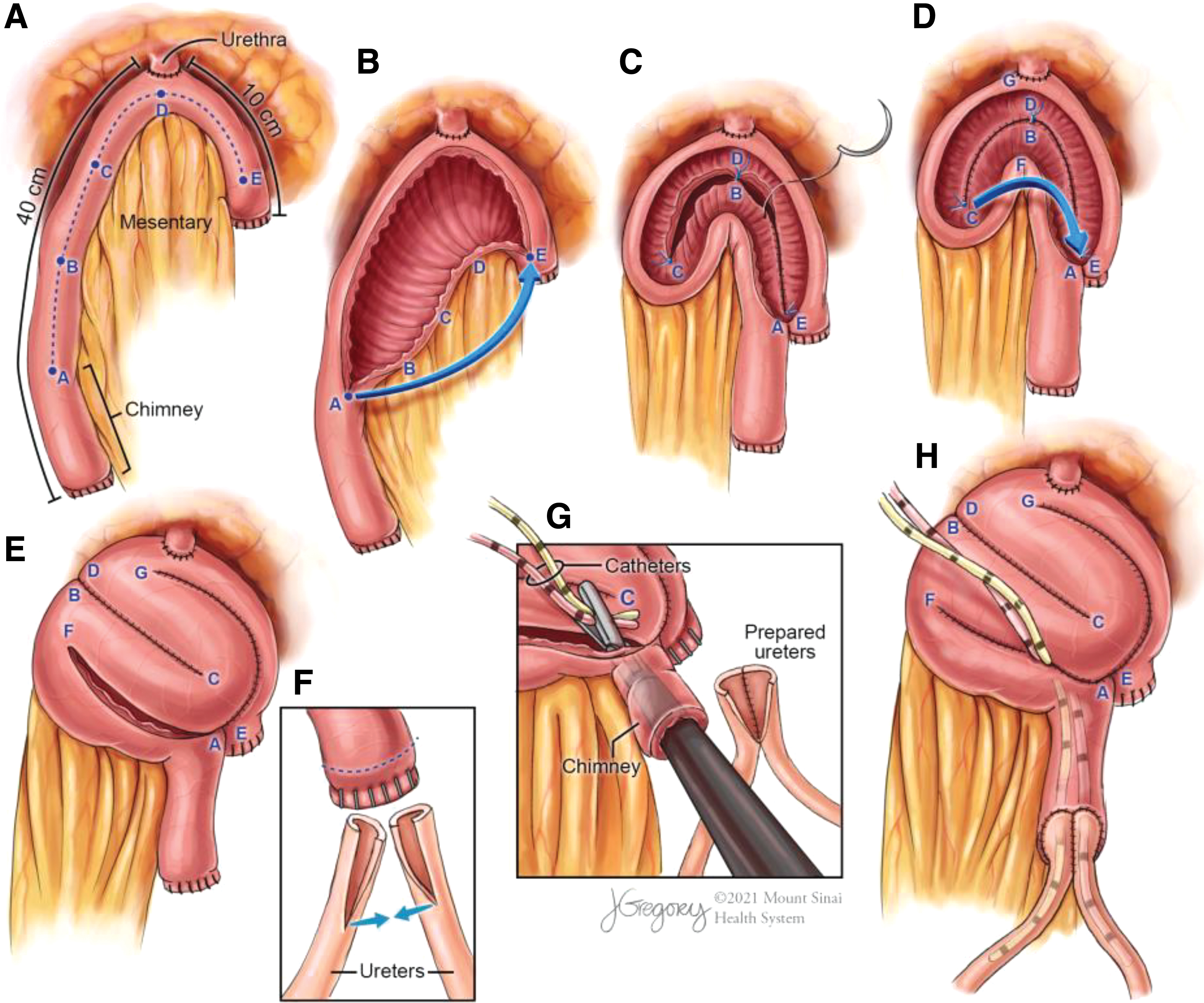
Surgical steps of intracorporeal neobladder reconstruction.
Using a double-armed 3-0 barbed suture, a modified Rocco stitch is performed to reapproximate Denonvillier's fascia, the rhabdosphincter posterior to the urethral and the posterior aspect of the ileum. 18 This posterior reconstruction brings the ileum in close proximity to the urethral stump and provides a strong posterior support to the urethroenteric anastomosis. A 1.5 cm incision is performed on the anterior aspect of the ileum at the intended site of anastomosis. Continuing with the same suture that was used for the posterior reconstruction, the urethroenteric anastomosis is completed in a running fashion using a Van Velthoven technique. 19
Bowel resection and anastomosis
The fourth robotic arm is dedocked to allow the introduction of the endoscopic stapler through the left 15 mm port (Fig. 2A). Staple loads of 60 mm are applied perpendicular to the bowel to select a segment of ileum of ∼50 cm extending from 40 cm proximal to 10 cm distal to the urethroenteric anastomosis. Bowel continuity is obtained by performing a stapled side-to-side anastomosis. A 1 cm incision is made on the antimesenteric side of the two bowel segments to be anastomosed and the jaws of a 60 mm stapler are introduced in each hole and fired. A second load of 45 mm is introduced in a similar fashion to ensure a widely patent anastomosis. A 60 mm stapler load is then fired transversally to close the remaining openings.
Neobladder formation
The intestinal segment used for the neobladder reconstruction is detubularized on its antimesenteric border, leaving 10 cm of intact ileum proximally for the chimney (Fig. 2B). Three stay sutures are then placed to position the intestinal segment as depicted in Figure 2C. The adequate placement of these stay sutures is important as they will dictate the configuration of the neobladder. They also help in handling the intestinal segment to facilitate suturing. The posterior plate of the neobladder is closed with a 3-0 barbed suture in a running fashion (Fig. 2C).
The intestinal segment is folded as depicted in Figure 2D to create a spherical neobladder. The distal aspect of the anterior wall is then closed in a similar fashion while leaving the proximal part open (Fig. 2E). At this time, the final catheter is installed and the balloon is inflated under direct vision to ensure adequate positioning. A 20F or 22F catheter with large evacuation holes is used to provide optimal urine drainage.
Ureteroileal anastomosis
The ureteroileal anastomosis is performed using Wallace technique. 20 Clips with 5 cm strings are placed at the distal end of the ureters at the time of the initial dissection to facilitate manipulation and exposure. The strings from both ureters are clipped together, grasped with the fourth robotic arm, and pulled upward in preparation for the anastomosis. Both ureters are widely spatulated and their medial edges are sutured in a running fashion with a 5-0 resorbable monofilament suture (Fig. 2F, G). The mesentery is dissected off the proximal end of the chimney at ∼5–10 mm to expose the serosa and ensure good visualization for ureteroenteric anastomosis. The staple line on the proximal end of the chimney is removed and the excess mucosa is excised to facilitate anastomosis (Fig. 2F). A guidewire is introduced transcutaneously in the suprapubic region through a 14 gauge angiocatheter. Using the needle driver, the right robotic arm is passed through the chimney to grasp the guidewire and allow proper tension to introduce a single J stent on the guidewire. The stent is grasped with the needle driver, brought through the chimney (Fig. 2G), and placed in one of the ureters. This step is repeated for the second ureter.
The ureteroenteric anastomosis is performed using a 3-0 double-armed barbed suture. The anastomosis is started on the lateral side of the left ureter and the first four passes are parachuted to facilitate visualization. For neobladder, we prefer to start the anastomosis on the left ureter because this part will become harder to visualize as the anastomosis progresses. The anastomosis is then carried on circumferentially after resecting the excess ureter distally and sending it for final margin evaluation.
The proximal part of the anterior neobladder is then closed with a running barbed suture (Fig. 2H). Care is taken to encircle and immobilize each stent individually to limit the risk for the stents to be inadvertently pulled out. The stents are also secured to the skin.
The final step is to perform a leak test by injecting ∼100 mL of saline in the neobladder and inspecting for the presence of leak. We do not routinely leave a surgical drain.
Postoperative Care
We favor the use of non-steroidal anti-inflammatory, acetaminophen, gabapentin, and local analgesic in the management of postoperative pain to limit the use opioids. 17 Postoperatively, the principles of the ERAS pathway are implemented. 13 Early ambulation is encouraged and clear liquid diet is resumed on the first postoperative day. We do not routinely leave a nasogastric tube after the surgery. During the hospital stay, the ureteral stents and the bladder catheter are flushed at least twice a day to prevent clogging and ensure optimal drainage. The ureteral stents are left in place for 7–10 days and the bladder catheter is removed after ∼3 weeks.
Troubleshooting
A significant issue that may be encountered during intracorporeal neobladder reconstruction is the impossibility to bring the distal ileum down in the pelvis to perform the urethral anastomosis. This problem most often occurs in patients with increased intraabdominal fat. When faced with this situation, multiple steps can be taken to bring the intestine downs to the urethra.
One way to gain some length is to do the incision for the urethral anastomosis closer to the anterior mesenteric border of the ileum. When the ileum is detubularized, this will unroll the intestine thus reducing the tension on the anastomosis. Superficial incision of the peritoneum overlaying the mesentery may also allow to gain additional mobility. Another technique is to dissect the mesentery off the ileum on a few millimeters on each side of the intended urethroenteric anastomosis to allow passage of two vessel loops around the ileum. These vessel loops can then be used to pull down the ileum toward the urethra.
In our experience, using a combination of those techniques, we have always been able to perform a satisfactory urethroenteric anastomosis. We have not had to convert to open surgery or to an ileal conduit because of an impossibility to bring the ileum down to the urethra.
Alternate Techniques
Most of the literature on intracorporeal neobladder reconstruction is based on Studer type neobladder technique such as the one described in this article. 3 Other published approaches include the Hautmann “W” pouch, 21,22 “Y”-pouch, 23,24 and PADUA pouch. 25 These different approaches are reasonable options as they respect the fundamental surgical principle of using detubularized ileum to construct a low-pressure reservoir. 2 In their recent review of published literature on intracorporeal neobladder techniques, Otaola-Arca et al concluded that no single technique had been clearly shown to be superior. 3
Clinical Outcomes
We have previously published detailed surgical outcomes of this technique. 26,27 High grade complications occur in ∼30% and 15% of patients from 0 to 30 days and from 31 to 90 days postoperatively respectively. At 12 months, up to 89% and 76% of male patients achieve daytime and nighttime continence. Female daytime and nighttime continence is 66%–70% and 66%–80% respectively. 26,27 Table 1 presents results from major series of intracorporeal Studer neobladder reconstruction.
Operative Outcomes of Intracorporeal Studer Neobladder Reconstruction
At 6 months.
At 9 months.
Conclusion
Intracorporeal neobladder reconstruction after cystectomy has been developed with the objective of reducing perioperative morbidity. By following the standardized surgical steps of the Karolinska technique, we believe that this approach can be learned and reproduced safely by motivated robotic surgeons.
Footnotes
Funding Information
No funding was received for this work.
Supplementary Material
Supplementary Data S1
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.