
Abstract
Robot-assisted microsurgery is a trending approach for the treatment of male infertility and chronic scrotal pain. The advantages seem to include increased optical magnification, improved surgical efficiency, absent tremor, and similar outcomes with standard methods. This chapter covers robotic microsurgical application and techniques for: robot-assisted vasectomy reversal with vasovasostomy and vasoepididymostomy, varicocelectomy, microsurgical testicular sperm extraction, and targeted denervation of the spermatic cord.
Featured Video
https://stream.cadmore.media/player/9a12c94d-82cc-4968-907d-920957050427

Introduction
Microscope was first introduced to the operating room (OR) in 1921 and revolutionized surgery of microscopic structures. 1 Since then, optical engineering and microsurgery have been in progress to the point of incorporation of robotic technology into common practice. Robotic assistance provides multiple advantages, including high-resolution three-dimensional (3D) optics, enhanced precision with elimination of tremor and as much as 5:1 motion scaling, improved surgeon ergonomics, and ability to control multiple instruments simultaneously without the need of a skilled assistant. These benefits have prompted the robotic microsurgical approach for treatment of male infertility and chronic scrotal pain, specifically, vasectomy reversal, subinguinal varicocelectomy, testicular sperm extraction, and targeted denervation of the spermatic cord. 2
In 2004 Kuang and coworkers performed the first robot-assisted andrological procedure with an ex vivo vasovasostomy on human vas specimens. 3 Following studies compared the robotic assisted vasovasostomy (RAVV) with microsurgical vasovasostomy and demonstrated superiority of robotic approach in terms of decreased operative time and sperm granuloma formation at the anastomosis site. 4 In 2004, Fleming confirmed excellent patency on two patients who underwent bilateral RAVV. 5 Corcione and associates described the first subinguinal robotic assisted varicocelectomy (RAVx) in 2008 with notably good outcomes. 6 After these remarkable results, area of utilization has expanded massively for robotic surgery in male infertility and chronic orchialgia (CO). 7,8
CO is an often underdiagnosed, but common clinical condition that is defined as testicular pain lasting >3 months. 9 The pain could be intermittent or constant in nature and involve unilateral or bilateral testicles. The condition is thought to affect over 100,000 men annually. 10 The pathophysiology of the pain can be idiopathic or caused by genitofemoral or ilioinguinal nerve irritation due to manipulation during vasectomy, hernia repair, sports injury, and abdominal injury. To this day, the exact sequel that leads to pain is not well understood for CO; one common perception is the “two hit theory” (Fig. 1). The theory suggests that there is a baseline inflammatory or genetic process that leads to wallerian degeneration (Fig. 2) of the peripheral nerves. This leads to hypersensitivity of the ilioinguinal and genitofemoral nerves, to which a second inciting event such as trauma will provoke neuropathic pain in the innervated areas.
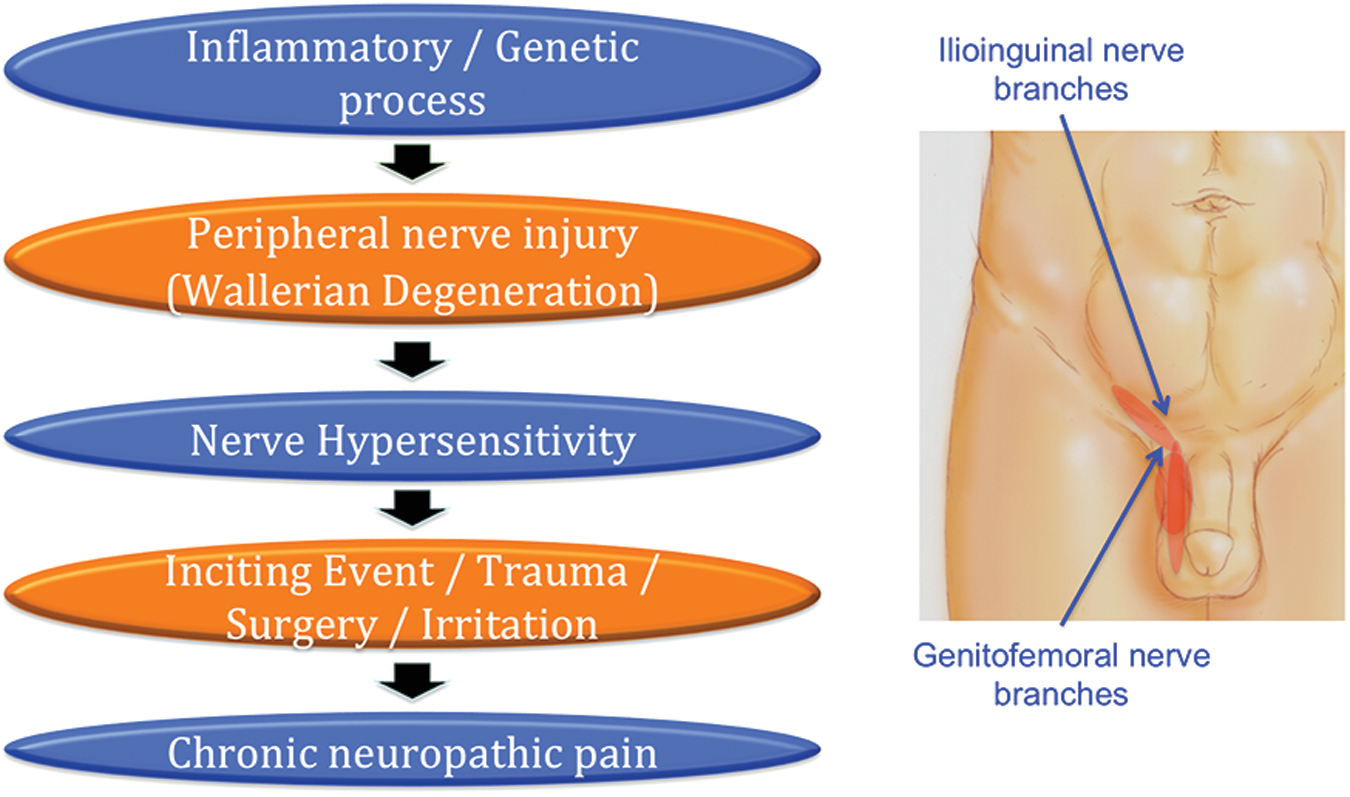
Two hit theory on cause of chronic orchialgia.
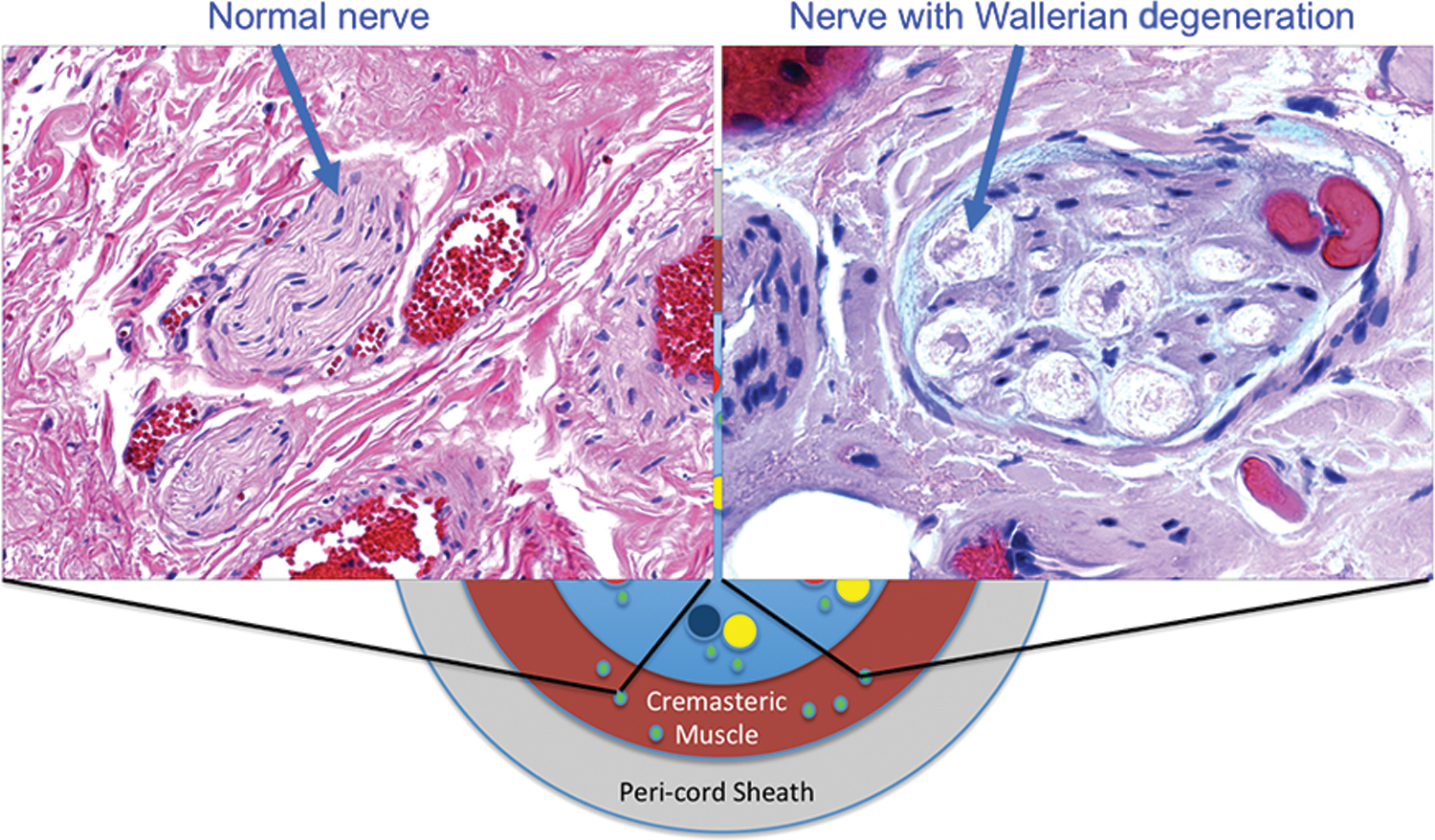
Nerve fiber with and without Wallerian degeneration on H&E staining.
Parekattil and colleagues reported multiple advantages of robotic assisted targeted microsurgical denervation of the spermatic cord (RTMDSC) for chronic groin and testicular pain in 2008. The technique involves denervation of specific nerves found to have abnormal axons (Wallerian degeneration) within the spermatic cord. 11 Three primary locations of these abnormal nerves are found to be at (highest to lowest): cremasteric nerve fibers, peri-vasal tissue and the vasal sheath, posterior lipomatous/posterior-arterial tissue.
In this chapter, we will feature the following procedures for the management of male infertility and CO: microsurgical RAVV, robotic assisted vasoepididymostomy (RAVE), robotic assisted varicocelectomy (RAVx), microdissection-testicular sperm extraction (micro-TESE), and RTMDSC.
Preoperative Preparation
Anticoagulant agents and supplements like vitamin E are generally ceased 5 to 7 days before the procedure. A broad-spectrum antibiotic is generally administered at least 30 minutes before the skin incision. Mechanical lower extremity compression stockings are used for deep venous thrombosis prophylaxis.
Operative Setup and Patient Positioning
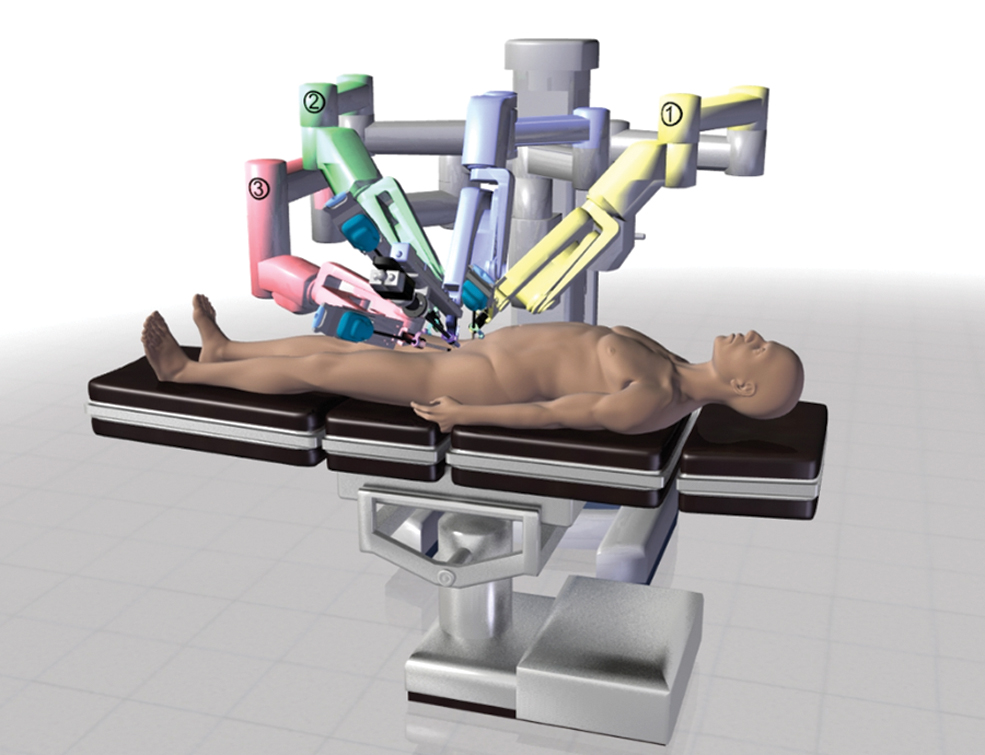
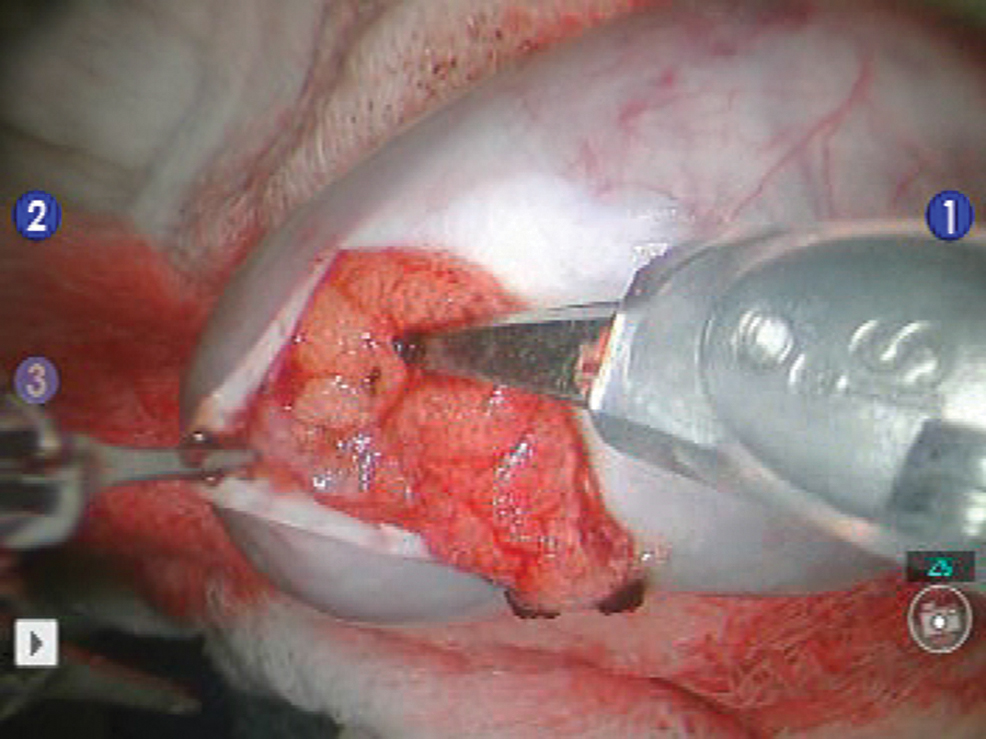
The patient is placed in a supine position, prepped, and draped in a standard surgical manner. Skin incisions are made and, with proper dissection, relevant operative tissues are exposed. The robot is docked to the right side of the patient and set up for the microsurgical portion of the case (Fig. 3). Figure 4 illustrates the proper trocar robotic arm placement. Trocars are loaded with the instruments. Instruments are advanced 4 to 5 cm beyond the tip of the trocar to optimize and stabilize the range of motion. A zero-degree camera lens is used to visualize the field.

General robotic position and setup for microsurgery cases.
Robotic arm and trocar placement for microsurgery cases.
Microsurgical Robotic Assisted Vasovasostomy (RAVV)
Indications
Indications for vasectomy reversal regardless of technique (RAVV or RAVE) fall into two categories: fertility and pain. 12 Fertility purposes may build upon a wide range of social and/or psychosexual rationale. Pain, on the other hand, is the consequence of a condition called postvasectomy pain syndrome (PVPS). Although the exact incidence of PVPS is unknown, estimates have ranged anywhere from 0.9% to 15%, and a recent meta-analysis found an overall incidence of 5%. 13 Vasectomy reversal still remains as an effective treatment modality for PVPS with improved quality of life outcome rates reported as high as 93%. 14
Technique
Initially, the proximal and distal ends of the vas deferens (underlying the previous vasectomy incision site) are palpated through the scrotal skin. With a towel clip, the distal vas is fixed into place (Fig. 5). A local anesthetic agent, typically marcaine or lidocaine, is administered into this area. A 1 to 2 cm vertical incision is made overlying the vas, beginning inferiorly from the previously placed towel clip (Fig. 6). Using a combination of fine electrocautery and sharp dissection, the distal and proximal ends of the vas are dissected free to allow a tension-free anastomosis. The proximal vas is carefully transected with a #11 blade, and fluid is milked through the new opening for further assessment. Intraoperative microscopic examination of the fluid is performed. If no sperm is present in this proximal fluid, surgical plan is converted to RAVE. If viable sperm is found, then RAVV is performed as planned. The adventitia of either end of the vasa is approximated together with a 3-0 Prolene suture to create a tension-free anastomosis and provide a stable anastomosis field while doing so.

Skin and vas over towel clip for robotic vasectomy reversal.

Skin incision for robotic vasectomy reversal.
The robot is now positioned from the right side of the patient to perform the microsurgical vasovasostomy component of the procedure. Black diamond microforceps are loaded on both the right and left robotic arms. The micro-Potts scissors are inserted on the fourth robot arm. The zero-degree camera lens is introduced on the robot camera arm. The two ends of the vas are placed on a 1/4″ Penrose drain. The surgical assistant passes a 9-0 nylon suture that is secured in its inner packaging to the optical field. The suture is grasped using the black diamond right hand grasper and cut to about 2 inches length using the micro-Potts scissors. The 9-0 nylon suture is wielded and maneuvered using the black diamond forceps using both left and right arms as needle drivers. The posterior muscularis layer of the two ends of the vas is now approximated (Fig. 7). Two or three double-armed 10-0 nylon sutures are now placed inside-out to re-anastomose the posterior mucosal lumen of the vas (Fig. 8). Three double-armed 10-0 nylon sutures are used to close the anterior mucosal lumen of the vas (Fig. 9). Five to six 9-0 nylon sutures are used to approximate the anterior muscularis layer of the vas (Fig. 10). The same procedure is now conducted on the other side by repositioning the robotic arms. The Penrose drain is carefully removed. The anastomosis site is placed back into the scrotum, and the tissue and skin are closed with absorbable suture. Skin glue and steri strips are applied.
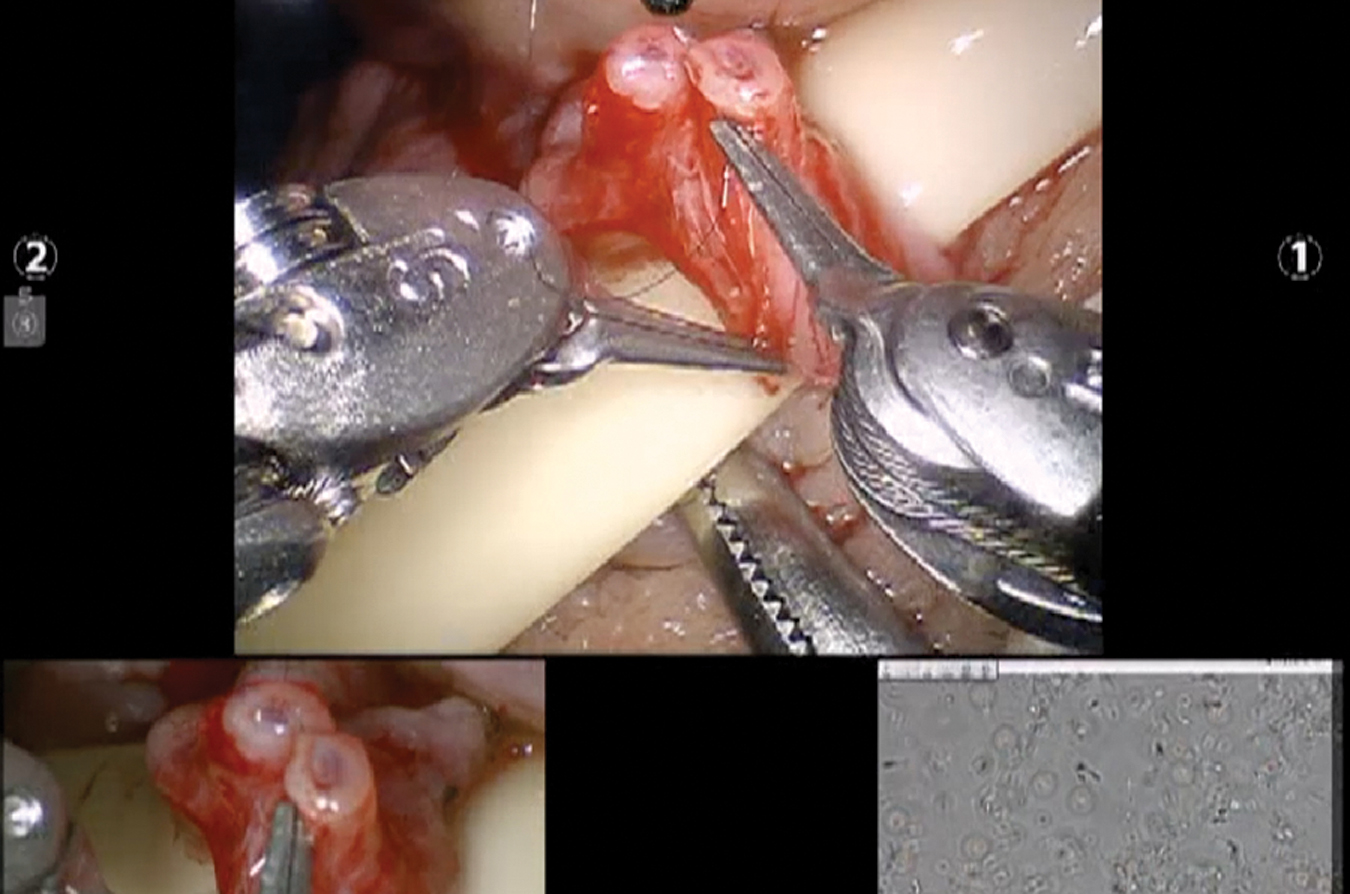
RAVV posterior muscular anastomosis. RAVV.
RAVV posterior luminal anastomosis.
RAVV anterior luminal anastomosis.
RAVV anterior muscular anastomosis.
Microsurgical Robotic Assisted Vasoepididymostomy (RAVE)
Technique
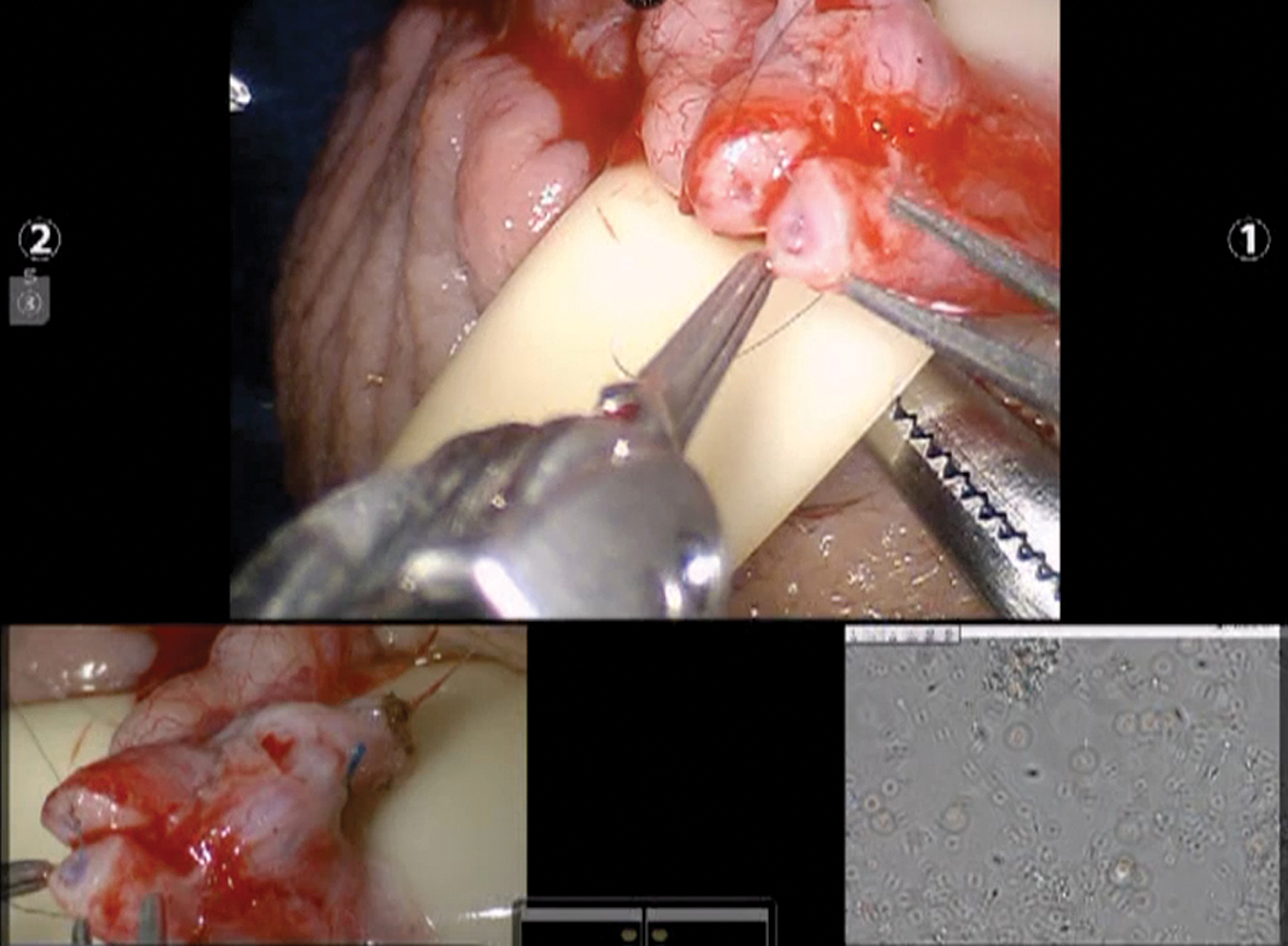
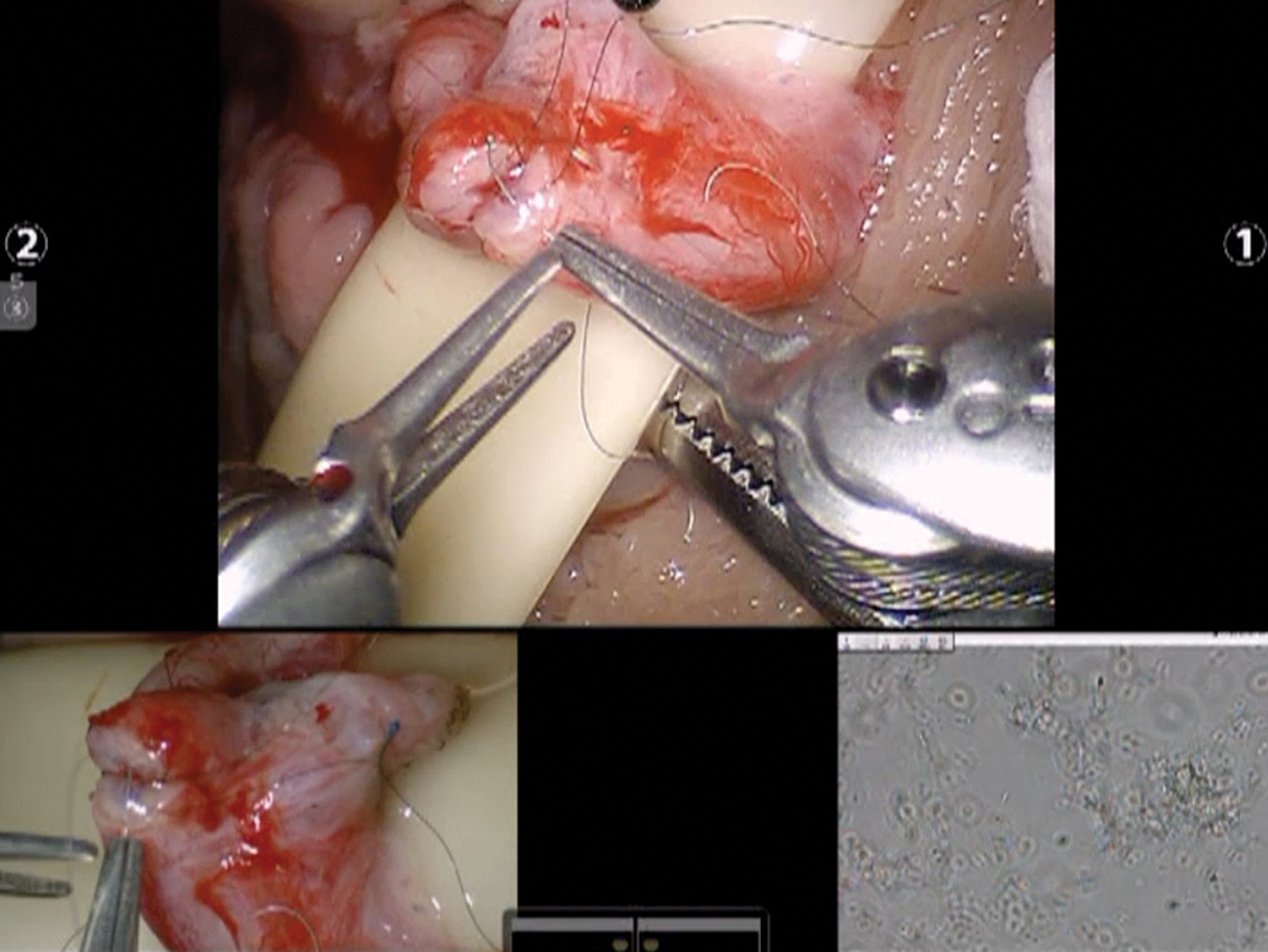
The RAVE procedure starts as described above in RAVV and proceeded when there is no sperm in the fluid from the proximal vas. The scrotal incision is extended 1 to 2 cm inferiorly. The testicle is delivered out, and the tunica is incised to expose the epididymis. The adventitia of the epididymis is incised proximal to the level of epididymal obstruction (blue/gray zone with dilated epididymal tubules). Adventitia of the vas is attached to the testicle with a 3-0 Prolene suture to create a tension-free anastomosis. The vas' adventitia is stripped off, and the isolated end of the vas is advanced toward the epididymal tubules. The robot is now brought to the field as above. Two 10-0 nylon double-armed suture needles are placed longitudinally, parallel to each other through a single epididymal tubule to expose the tubule (Fig. 11). This tubule is then incised longitudinally using the micro-Potts scissors between the two suture needles to create a lumen for the anastomosis (Fig. 12). The fluid is then collected and assessed under a separate phase contrast microscope for the presence of sperm.

RAVE exposed epididymal tubule. RAVE.
RAVE incision of epididymal tubule.
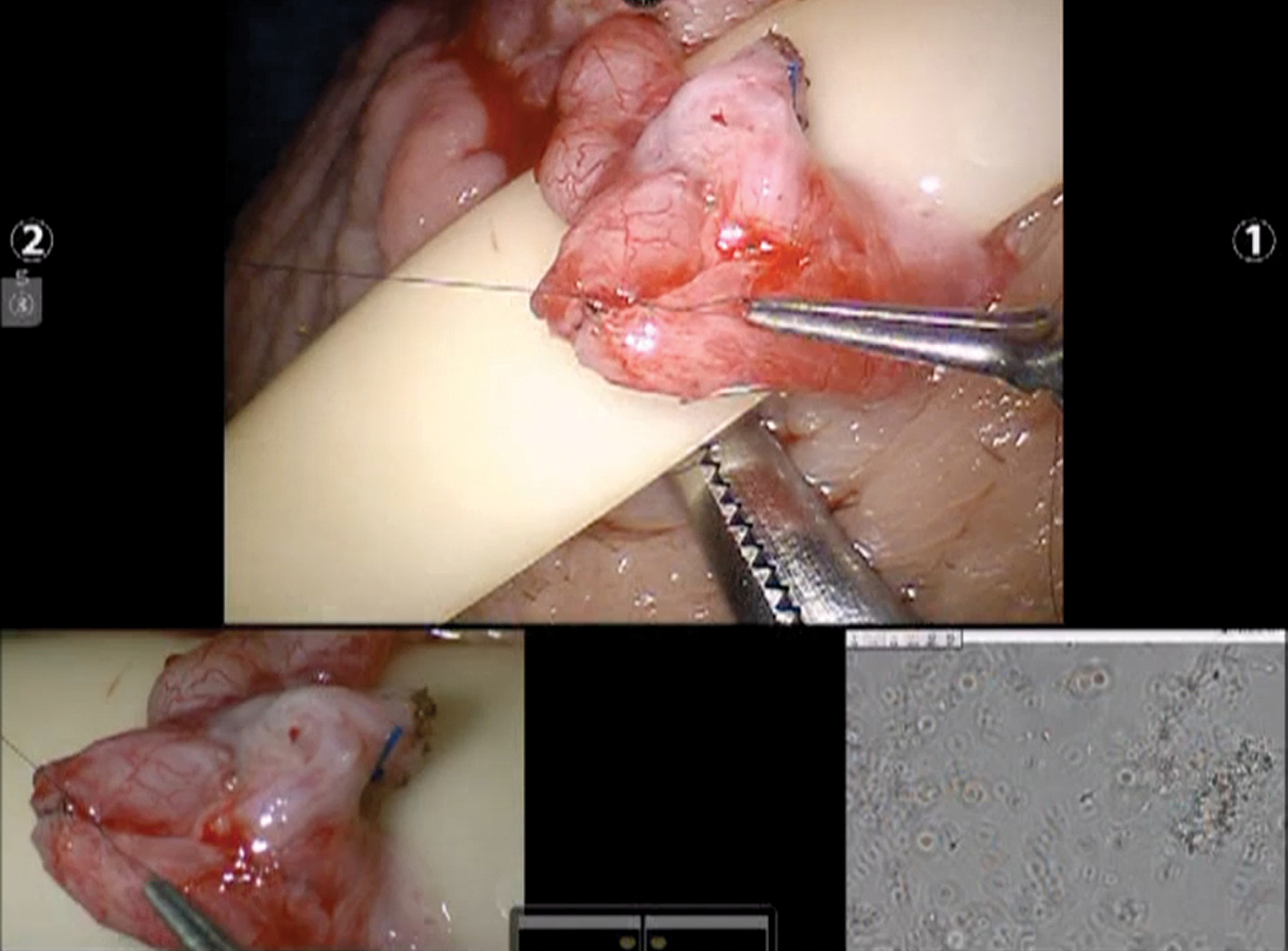
When sperm is confirmed, two double armed 10-0 nylon needles in the tubule are advanced all the way through and then all four of the needles are brought inside-out on the vas mucosal lumen to involute the epididymal tubule lumen into the vas lumen (Fig. 13). Five to six 9-0 nylon sutures are placed circumferentially to approximate the muscularis of the vas to the adventitia of the epididymal tubule (Fig. 14). The testicle and the site of anastomosis are carefully delivered back into the scrotum. The dartos layer and skin are closed; skin glue and steri strips are applied.

RAVE involution vasoepididymostomy.

RAVE vas muscularis to epididymal adventitia approximation.
Postoperative care
Postoperative care for RAVV-RAVE patients doesn't generally require hospitalization. Patients are advised to use ice packs throughout the surgery day and usually prescribed analgesics as needed. Wound care directives are given. Patients are asked to refrain from strenuous activity and sexual intercourse for about 3 weeks. General post-op evaluation is often done with an over the phone follow-up session. Sperm quality assessment may be initiated approximately after 3 months but it may take as much as 12 months for the values to get back to normal.
RAVV/RAVE outcome review
Kavoussi and coworkers in 2019 indicated RAVV to be not only as effective as microsurgical vasovasostomy but also quick to adept in terms of transition of the surgical approach from standard microsurgery to robotics. This single microsurgeon study pointed out that high-percentage patency rates can be achieved early in the process of transitioning, and it will take only 75 RAVV cases to optimize and plateau operative times, as well as the anastomosis times. 15 Another study by Marshall and associates suggested remarkable early results of a single layer anastomosis technique performed with the robot. Effective reversal was accomplished in 88% of the followed patients with an average sperm density of 31.0 million/mL and an average motility of 29% that are similar to standard microscopic vasovasostomy. 16 In our practice, between July 2007 and December 2020, 264 robot-assisted vasectomy reversals (162 bilateral RAVV, 102 RAVE) were performed by a single fellowship trained microsurgeon. Seventy-six of these patients had chronic scrotal pain after vasectomy, and the rest consented to the procedure for fertility purposes. Median patient age was 40 years, and median duration from vasectomy was 7 years for RAVV and 11 years for RAVE, respectively. Median OR setup duration was 20 minutes, and median robotic operation duration was 90 and 120 minutes for RAVV and RAVE, respectively. After 12 months median follow-up, patency rates (>1 million sperm/ejaculate) were 91% in the RAVV group and 60% in the RAVE group. Pain relief occurred in 68% of the patients who underwent RAVV or RAVE for chronic scrotal pain related to vasectomy. Table 1 demonstrates outcomes from other studies utilizing the microsurgical approach to our robotic approach.
Summary of Outcomes Compared with Other Studies on Microsurgical Vasovasostomy/Vasoepididymostomy
Outcomes from standard pure microsurgical approach.
To our knowledge this serial is the world's largest regarding robot-assisted microsurgical vasectomy reversal, and the procedure appears to be safe and feasible. We believe advantages like having a stable microsurgical platform, ergonomic controls for the surgeon, elimination of tremor, and magnified immersive 3D vision all contribute to meet the patency rates of experienced standard microsurgery centers. Further evaluation and longer follow-up are recommended to see its true potential and the cost–benefit ratio.
Microsurgical Robotic Assisted Varicocelectomy (RAVx)
Indications
Indications for varicocelectomy consist of subfertility-infertility, testicular hypotrophy, and varicocele associated pain. 17 Some recent studies also uncovered that varicocele repair might lead to improved conditions in certain situations like nonobstructive azoospermia, androgen deficiency, preassisted reproduction to increase conception chance, and elevated sperm DNA fragmentation/oxidative stress findings. 18 –20
Technique
A 1 to 2 cm subinguinal incision is made over the external inguinal ring. A tongue depressor is placed underneath the cord to keep the cord elevated and exposed well for the robot. The robot is brought in from the right of the patient. A zero-degree camera lens is used for optimal view. The black diamond micro forceps is loaded on the right robotic arm, the micro bipolar forceps on the left arm, and the curved monopolar scissors on the fourth arm. The anterior cremasteric sheath of the spermatic cord is incised to expose the cord structures.
The arteries are identified using real time micro-Doppler (Vascular Technology, Inc., Nashua, NH). All dilated veins are located, isolated, and tied on two ends using 3-0 silk (Fig. 15). Vein Mapper may be used to help identification of the veins (Fig. 16). Vessels are cut with curved monopolar scissors. The depressor is removed, and cord is placed back in place. Incision and the deep tissue and skin are closed.

Isolation and ligation of dilated vein.
Vein mapper assistance during robotic varicocelectomy.
Postoperative care
Typically, there is no hospitalization needed after RAVx. After the procedure, cold compress is suggested for one day, and compression shorts may be required for about a week. Patients are given wound care instructions, and non-NSAID painkillers are generally prescribed as needed. Patients may return to work in a few days in exception of jobs involving heavy lifting. Patients are followed up generally over the phone for post-op evaluation in about a week. RAVx for fertility cases should be scheduled an appointment within 3 to 4 months to assess sperm quality.
RAVx outcome review
From June 2008 to May 2019, 588 RAVx cases were performed in 489 patients. Indications for the procedure were the presence of a grade two or three varicocele and the following conditions: azoospermia in 48 patients, oligospermia in 100 patients, and chronic scrotal pain with or without oligospermia in 222 patients. The median duration per side was 20 minutes (10–80). Median follow-up was 13 months (1–75). Sixty-five percent of patients with oligospermia had a significant improvement in sperm count or motility, 15% (7 patients) with azoospermia converted to oligospermia, and 72% of the testicular pain cases had a significant reduction in pain (88% of these patients had targeted denervation of the spermatic cord in addition to varicocelectomy procedure). Two recurrences or persistence of clinical varicocele occurred, two patients developed a small postoperative hydrocele, and eight patients had postoperative scrotal hematomas (one required incision and drainage, rest treated conservatively). To our perception, the fourth robotic arm helped the surgeon to control one additional instrument during the cases without depending on the microsurgical assistant. It also allowed the surgeon to perform real-time intraoperative Doppler mapping of the testicular arteries while dissecting the veins with the other arms if needed.
McCullough and colleagues also reported significant increase in semen concentration (7.5 × 106 mL−1 pre-op vs 10.5 × 106mL−1 post-op; p < 0.003) in one of the biggest retrospective analyses conducted on 140 patients and 258 robot-assisted varicocelectomies. 21 The study also confirms similar outcomes in robotic approach with the traditional microscopic approach regarding increase in mean testosterone, increase in mean sperm concentration, and complication rates. Robotic varicocelectomy was associated with more cases resulting in treatment failure (9.7% vs 2.5% in traditional microsurgical approach). Table 2 compares outcomes between our subset of patients who were treated for infertility with RAVx vs a traditional microsurgical approach dataset.
Summary of Infertility Outcomes Compared with External Studies on Microsurgical Varicocelectomy
Outcomes from standard pure microsurgical approach.
RAVx appears to be a safe, feasible, and efficient procedure with comparable results to pure microsurgical varicocelectomy. The preliminary human results appear promising. Further evaluation and cost effectiveness studies are warranted.
Robotic Assisted Microdissection-Testicular Sperm Extraction (micro-TESE)
Technique
Over the scrotal median raphe, a vertical 4 to 5 cm incision is made. The incision is advanced deeper down to the tunica vaginalis, which is now incised to deliver the scrotum. The robot is positioned from the patient's right side in a similar manner to previous explanations. Black diamond micro forceps, micro-bipolar forceps, and Potts scissors are inserted in the right, left, and fourth robotic arms, respectively. After the testicle is isolated, a 2 to 3 cm transverse incision is made over the tunica to expose seminiferous tubules. The tunica of the testicle is everted to fully expose all the tubules in the testicle. The testicular lobules are carefully dissected through to find larger appearing seminiferous tubules (Fig. 17). Dilated tubules correspond to higher chance of sperm exploration. 22 These areas are sampled, and the specimens are examined immediately with phase contrast microscopy by a trained embryologist. More sampling is done until sufficient amount of sperm is collected, allowing assisted reproductive techniques to be attempted.
Exposure of larger seminiferous tubules.
In cases where no viable sperm is found, the testicle is more thoroughly evaluated. Dissection through deeper lobules of the testicle is conducted, and sampling from broader areas is performed. Adding another black diamond micro forceps in the fourth robotic arm can be helpful in deep dissection utilizing it as a retractor for the superficial structures as the surgeon is evaluating the deeper lobules. Once adequate sperm has been retrieved or adequate sampling has been performed, the tunical incisions are closed with 6-0 Prolene running suture. The testicle is released back into the tunica vaginalis cavity within the scrotum and closed in layers.
Postoperative care
As in previous cases, patients generally walk out the same day of the procedure. As needed, analgesics may be prescribed and cold compress can be suggested for a day. Follow-up should take place in a couple of days to discuss intraoperative sperm findings and about a week after for general post-op evaluation.
Robotic Assisted Targeted Microsurgical Denervation of Spermatic Cord
Indications
Indications for RTMDSC are limited to CO refractory to conservative treatment. Conservative treatments such as analgesics, anti-inflammatory agents, antidepressants, antibiotics, physical therapy, biofeedback, acupuncture, local nerve blocks, regional nerve blocks, and psychotherapy should be pursued as first line therapy. 23 The standard of care also suggests performing a spermatic cord block (SCB) to assess if there is any temporary relief in the pain before performing RTMDSC. Recent studies have proven correlation between the temporary response to SCB and long term response to RTMDSC with high positive and negative predictive values. 24
Technique
A 1 to 2 cm transverse subinguinal incision is made. The incision is extended deeper until the spermatic cord is reached. The cord is brought as much as the surface. Ilioinguinal and genitofemoral nerves are ligated by dissection and careful cauterization of posterior, medial, and lateral cord.
The robot is transported to the right side of the patient. A zero-degree camera lens is used. The right, the left, and the fourth robot arms are loaded with Black Diamond micro-forceps, Maryland bipolar grasper, and monopolar curved scissors, respectively (Fig. 18). If a flexible CO2 laser fiber (OmniGuide, Cambridge, MA) is used as the dissection tool, then the fourth arm is replaced with a Black Diamond micro-forceps to hold the FlexGuide laser (Fig. 19).
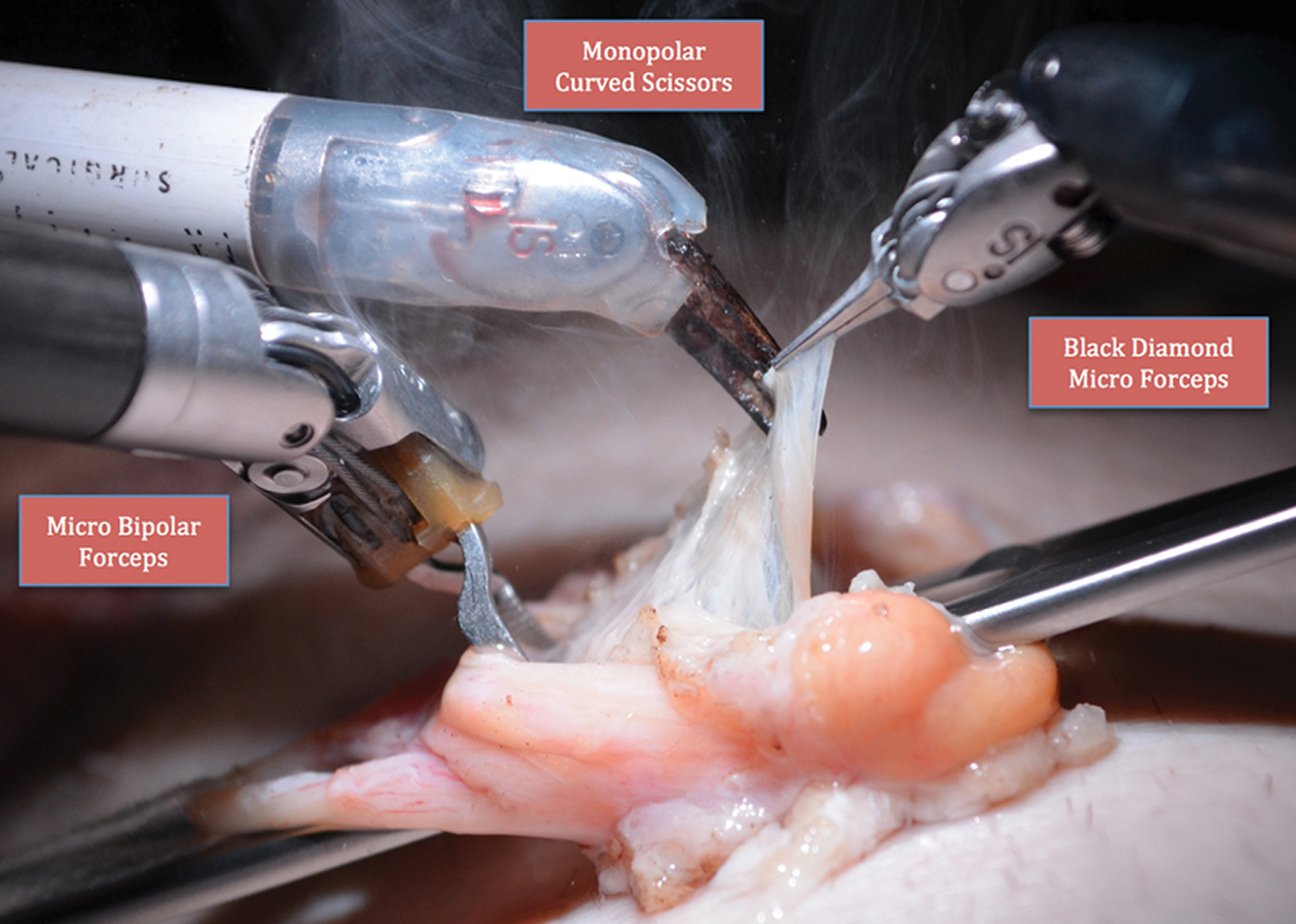
Standard robotic instrumentation for targeted denervation.
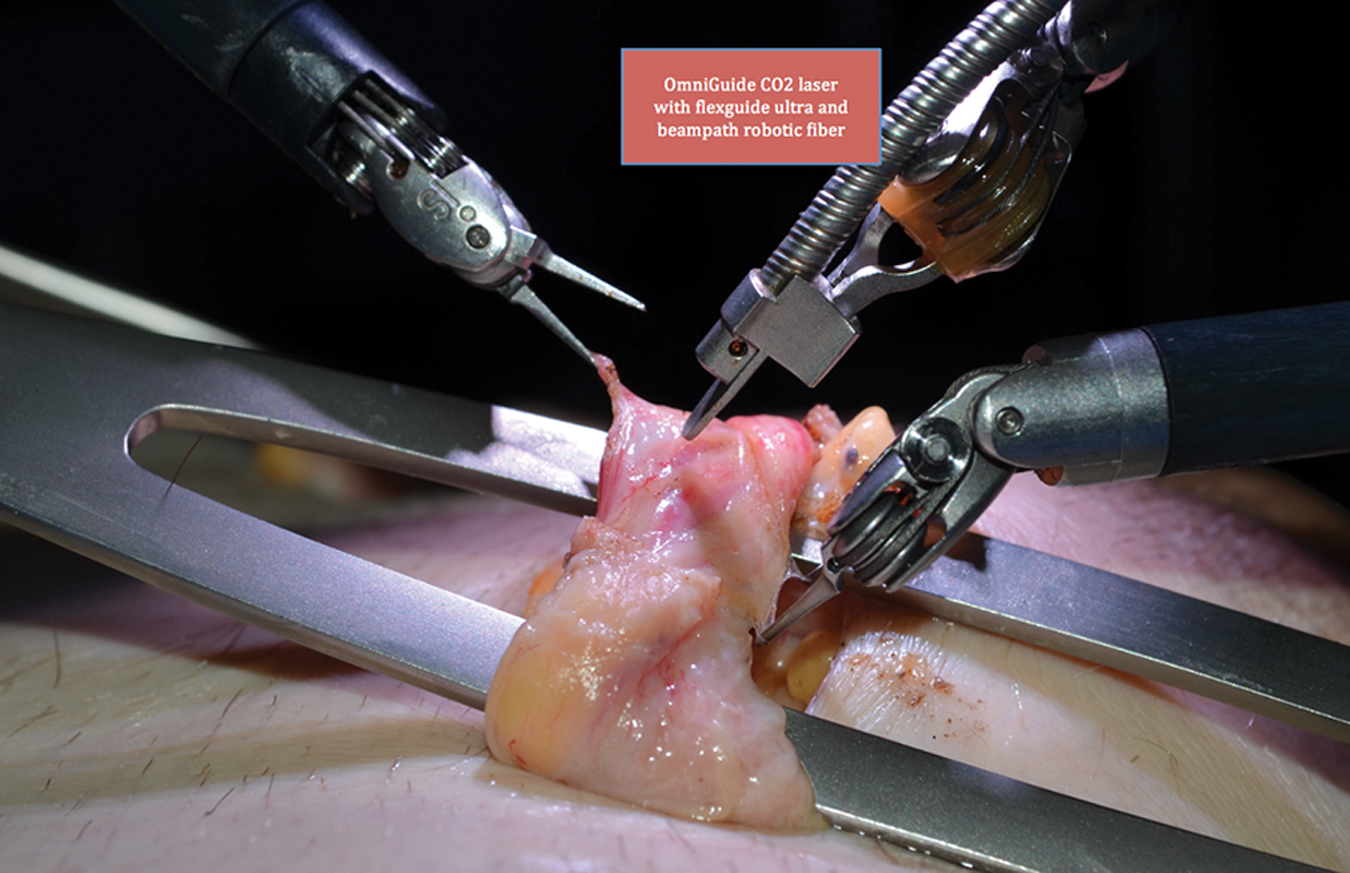
Flexible CO2 laser instrumentation during targeted denervation.
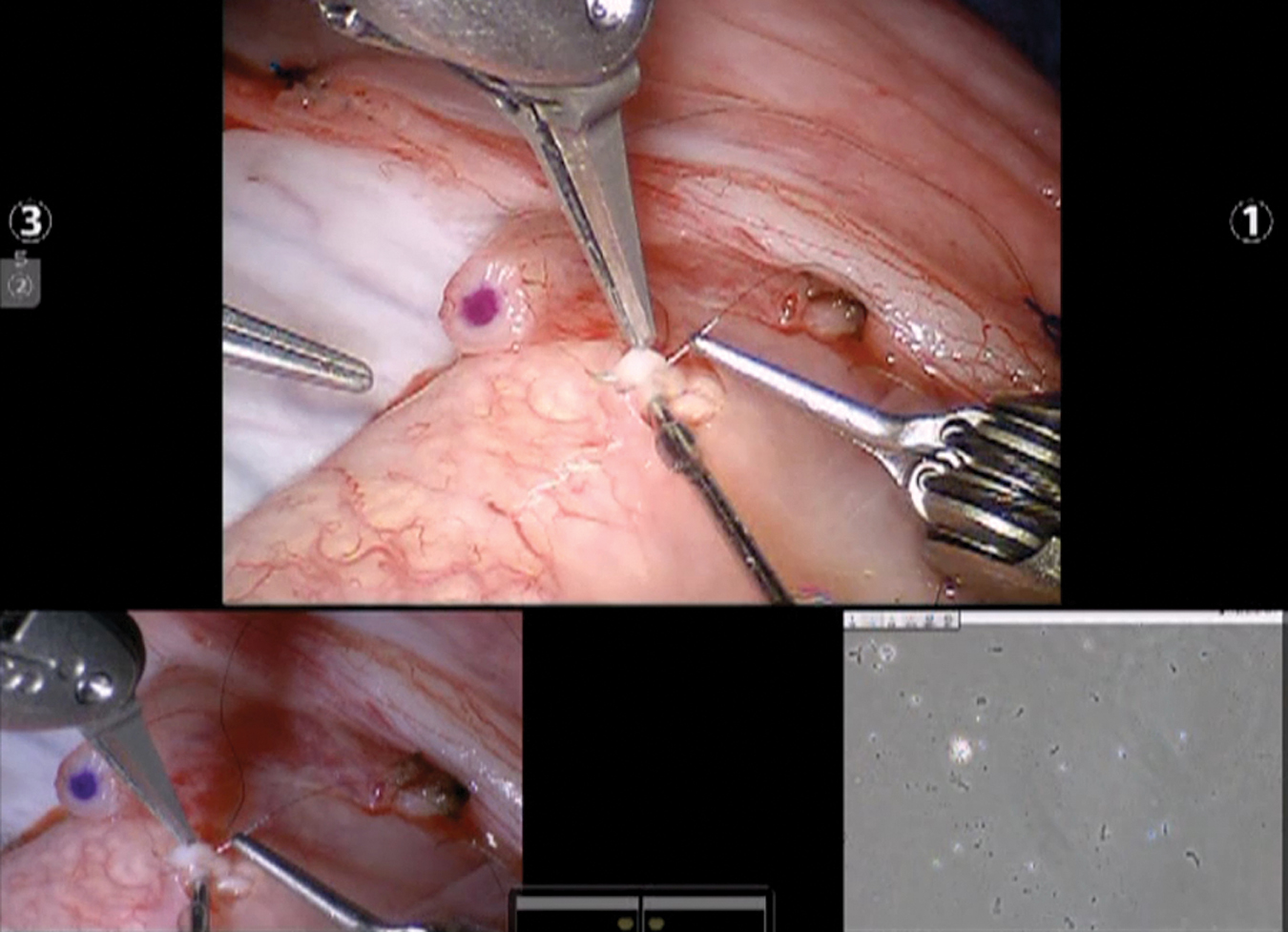
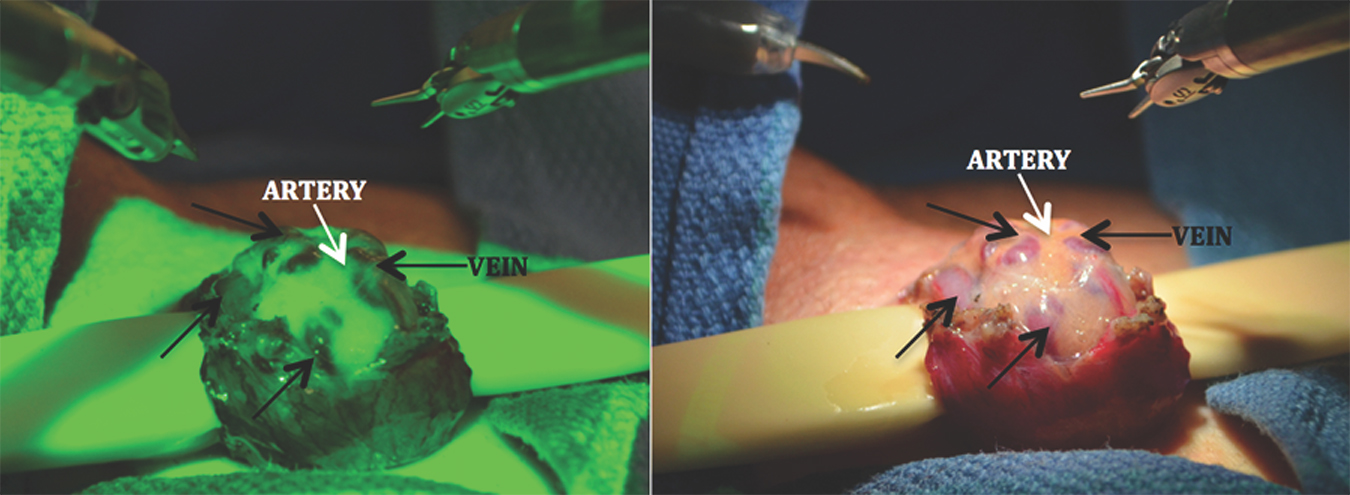
The anterior cremasteric muscle is cut. The presence of a testicular artery is confirmed (Fig. 20) with real time intraoperative micro-Doppler (Vascular Technology, Inc.). The posterior cremasteric fibers and posterior fat component are ablated. The vas is isolated, and generally the artery and vein to the vas are dissected away from the vas. The perivasal tissue is also ablated. Hydrodissection of the perivasal tissue is now performed (Fig. 21) using the ERBEJET2 hydrodissector (ERBE, Inc., Atlanta, GA) to ablate remaining nerves.
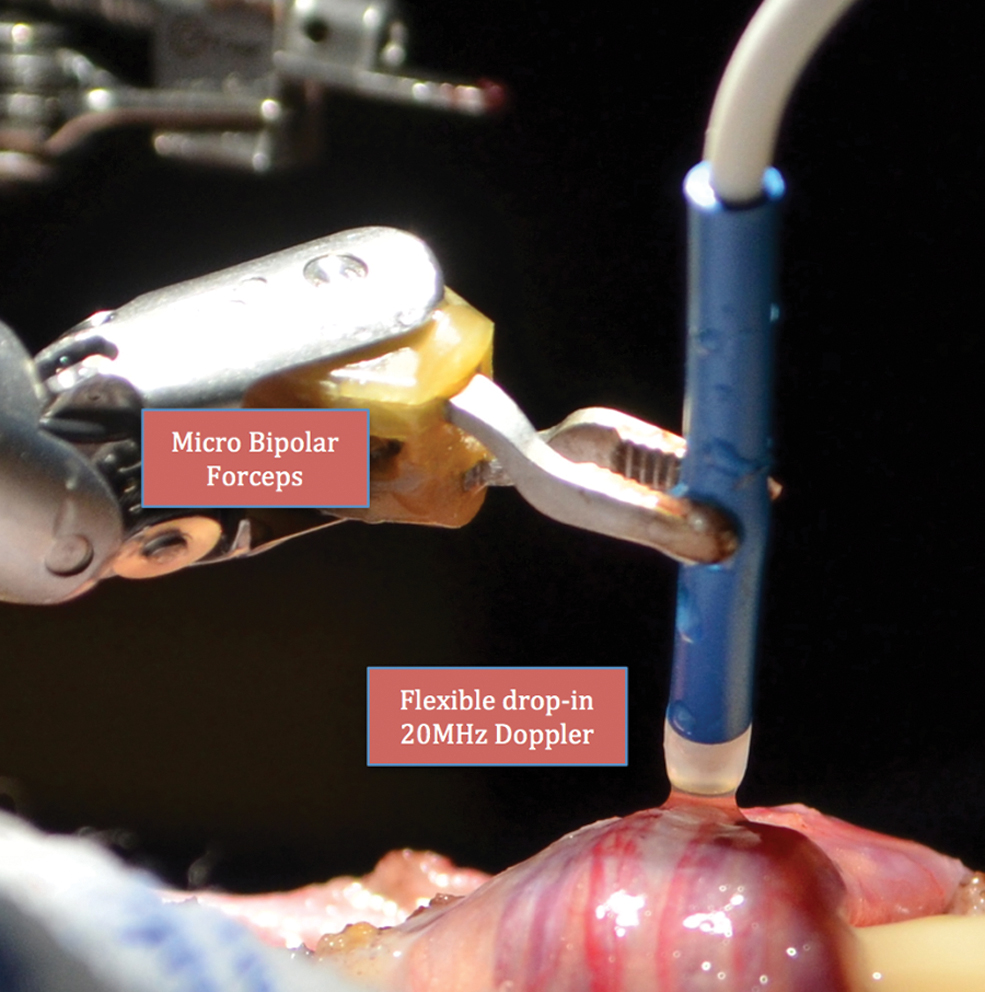
Confirmation of testicular artery using micro-Doppler.
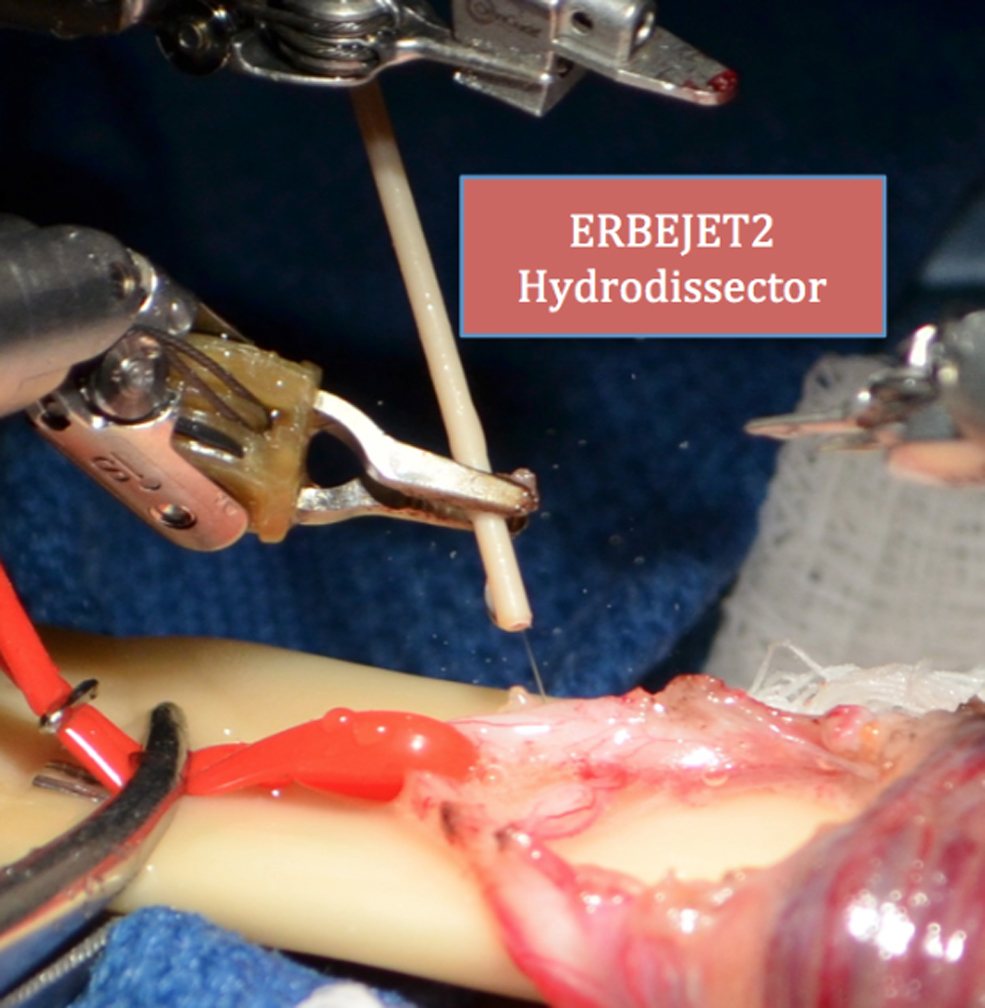
Hydrodissection of residual nerve fibers on perivasal tissue.
The cord is wrapped with Axoguard (Axogen, Inc., Gainesville, FL) bio-inert wrap to prevent neuroma formation by securing the ligated nerve ends. The wrap is loosely sutured around the vas using 6-0 Prolene interrupted sutures (Fig. 22). The robot is undocked. The cord is carefully placed back into its anatomical place; the incision and the deep tissue and skin are closed.
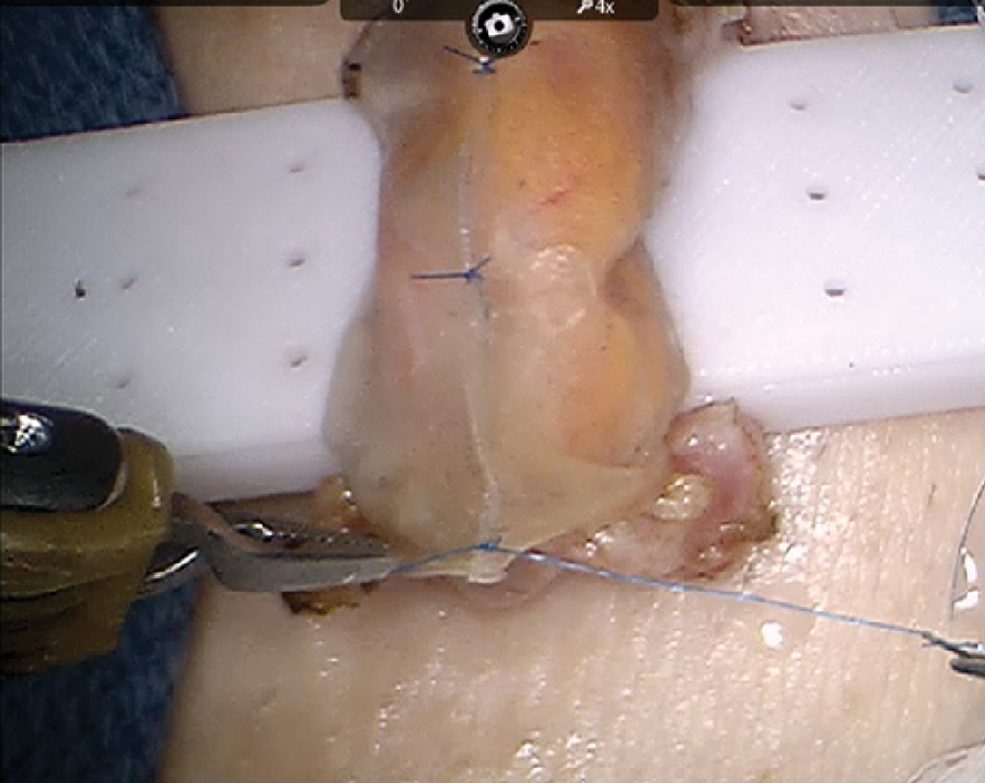
Secured Axoguard around spermatic cord.
Postoperative care
Typically, there is no hospitalization needed after RTMDSC. After the procedure, ice pack compression three to four times daily and compression shorts for about 2 weeks may be required. Patients are asked to refrain from sexual activity for 2 weeks and are given wound care instructions plus as needed painkillers. Patients usually return to work in a week. Patients are followed up usually in a week over the phone and after 3 to 4 weeks preferably in the office for pain evaluation.
RTMDSC outcome review
Between October 2008 and March 2020, 1356 RTMDSC procedures on 1195 patients have been performed. The pain was assessed utilizing a standardized validated pain assessment tool; PIQ-6 (QualityMetric, Inc., Lincoln, RI). Pain scores and physical examination were performed preoperatively and then postoperatively at 1, 3, 6, 9, and 12 months. At 70 months median follow-up (1–113 months) 84% of the patients had a significant decrease in their pain (43% complete response and additional 41% greater than 50% reduction in their pain score) by 6 months post-op. The procedure failed to provide any pain relief in 205 patients (15%). Median operative duration was 20 minutes (10–150). Complications included: 42 hematomas, 26 wound infections, 13 wound dehiscence, 6 pain relocations to leg, 2 anejaculation cases, and 4 seromas 2 of which required incision and drainage. Two testicular arteries and one vasal injury were repaired intraoperatively with robot-assisted microsurgical techniques without any further sequel. One patient had testicular artery injury that was repaired intraoperatively but developed testicular infarction and required orchiectomy postoperatively.
The 4th robotic arm allowed the surgeon to control one additional instrument (micro Doppler or hydrodissector) leading to less reliance on the microsurgical assistant. As far as we know, this is currently the world's largest RTMDSC serial and appears to be safe and feasible with promising results. Further follow-up and further evaluation are warranted.
Conclusion
The use of robotic assistance is rapidly expanding in many fields that perform microsurgery. Implementing this technology in male infertility and chronic scrotal pain has only proved promising results to this date possibly as a result of the provided advantages, including a stable microsurgical platform, ergonomic control of microsurgical instruments, elimination of tremor and magnified 3D vision with cockpit-view, and less reliance on a surgical assistant. As techniques evolve, robot-assisted microsurgery can provide endless opportunities for more efficient and less morbid procedures. It is important to acknowledge that robotic system is more expensive than traditional microsurgical systems. The whole system costs about 1.5 to 2 million USD plus additional annual maintenance fees of 110,000 to 150,000 USD and instrument costs that are ∼3000 to 4000 USD per case. 25 Furthermore, disposable instrumentation for the robotic cases adds roughly about 6000 to 7000 USD per case. It is still obscure whether the robotic platforms are cost effective in the long term for hospital systems. It is believed that the robotic platforms improve the efficiency of the surgeons after a certain number of cases, especially in complex surgical procedures. 26 There are also studies suggesting that long-term use of robotic platforms improves the cost utility. 27 We believe that at least 100 cases per year are needed in a hospital system for the robotic system to start becoming cost effective. Standard microsurgical microscope systems, on the other hand, cost about 350,000 to 500,000 USD with a 50,000 USD per year maintenance fee. Microsurgical surgery sets in this setting are also cheaper and cost about 5000 to 10,000 USD and are reusable with proper sterilization. In contrast, additional costs might be encountered during the standard microsurgical procedures where certain tools that are not included in the sets are needed. To our understanding, these situations are easier to manage with robotic platforms since these tools are more accessible and compatible with robotic console arms. Finally, there is the issue of insurance coverage for the robot. It is mostly covered under the facility fees of hospital systems since there is no specific code for robotics. This also raises the situation of robotic cases being almost exclusively done at hospitals throughout the United States unless the cost is self-paid. In light of all these considerations, clearly, there is a need for further assessments regarding the true cost–benefit ratio of the robots. Hopefully, this technology will only be of better use for our patients' care.
Footnotes
Acknowledgments
The authors thank “LOVO” for allowing them to narrate their video descriptions with the voices from
Authors' Contributions
O.E.: Formal analysis, Data curation, Writing-Original draft, Writing-Reviewing and Editing. A.G.: Visualization, Writing-Original draft, Supervision. S.J.P.: Investigation, Project administration, Supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.