
Abstract
Objective:
To evaluate perioperative parameters, clinical outcomes, and the learning curve of holmium laser enucleation of the prostate (HoLEP) in surgeons with experience in thulium laser enucleation of the prostate (ThuLEP).
Materials and Methods:
The learning curves for HoLEP of the first 50 consecutive patients of two surgeons experienced in ThuLEP were analyzed. In addition, demographic parameters, clinical outcomes, and adverse events (AEs) were evaluated.
Results:
Mean operation time was 70.9 ± 29.7 minutes (standard deviation) (Surgeon 1) and 74.4 ± 35.4 minutes (Surgeon 2), the mean enucleation efficiency was 1.5 ± 0.6 g/min (Surgeon 1) and 1.5 ± 0.7 g/min (Surgeon 2). The hemoglobin loss was 0.9 ± 0.8 and 0.8 ± 0.8 g/dL. For both surgeons, there was a significant learning curve in enucleation efficiency within the first 50 cases (Surgeon 1: p = 0.034, Surgeon 2: p = 0.006, both: p = 0.0003, Spearman's ρ = 0.351). Both surgeons started with an enucleation efficiency of around 1 g/min in their first 10 cases. No significant correlation between hemoglobin loss and experience could be found (p = 0.823, ρ = 0.025). While there was no significant learning curve for morcellation efficiency (p = 0.785, ρ = 0.028), a significant progress was found for one of the two surgeons regarding laser energy efficiency (p = 0.014). The overall incidence of all grade treatment-related AEs was low at 10.0%, and extremely low for significant complications with Clavien-Dindo Grade >II at 1%.
Conclusions:
In our analysis, switching to HoLEP is uncomplicated and safe for experienced ThuLEP surgeons. The enucleation efficiency was high from the beginning, but a learning curve was present for both surgeons. No learning curve was noticeable in hemoglobin loss and the incidence of complications, both of which were low throughout the study.
Introduction
Holmium laser enucleation of the prostate (HoLEP) has come to be a standard procedure in the surgical management of benign prostatic obstruction (BPO). 1 Its use in the surgical therapy of BPO was first described in 1995; the holmium:yttrium-aluminium garnet (Ho:YAG) laser with a wavelength of 2.140 nm is a pulsed solid-state laser, and it showed promising results from the beginning. 2 BPO treatment modalities are evolving rapidly, and HoLEP has become indispensable among them. 3 Short-term results demonstrate minimal morbidity, making HoLEP safe for patients with significant comorbidities and for prostates of any size. 4 Long-term results show durable deobstruction, and few patients require subsequent procedures. 4
Despite these advantages, access to suitable laser equipment and the longer learning curve are the reasons why this technique is vastly underutilized. 5 The performance of HoLEP requires experience and appropriate endoscopic skills. The most important factor for the occurrence of complications seems to be the surgeon's experience. 6 Several studies have investigated the learning curve of HoLEP 7 –9 ; the caseload for a surgeon to safely carry out the procedure with satisfactory efficiency and outcomes can be estimated at 50 cases, requiring careful case selection. 10
Another surgical option in the management of BPO is thulium laser enucleation of the prostate (ThuLEP). 11 The Thu:YAG laser transmits energy as a continuous wave with a wavelength close to 2.0 nm, and its use in the surgical therapy of BPO was first described in 2010. 12 The cutting ability of ThuLEP may be beneficial in some situations, as anatomical enucleation is not necessarily required. On the contrary, HoLEP is generally considered to be more anatomic, as the mechanical energy of the laser follows the path of least resistance between the adenoma and the surgical capsule. A recent meta-analysis found no significant differences in perioperative or functional parameters comparing ThuLEP and HoLEP and concluded that the choice of the laser should be based on surgeon experience and availability. 13
Diode laser enucleation of the prostate (DiLEP) and GreenLight laser enucleation of the prostate (GreenLEP) have been introduced more recently. 14 A meta-analysis showed no differences in the amount of resected prostatic tissue, major and minor complications and postoperative catheterization time between HoLEP and DiLEP. 15 Results after GreenLEP also seem to be similar to those of HoLEP. 16 In general, the principle of endoscopic enucleation seems to be more important than the energy source used. 17
To our knowledge, it has not yet been evaluated whether surgeons who are well acquainted with ThuLEP can easily and safely switch to HoLEP without special training. Furthermore, it is unclear if there is a learning curve for these surgeons as well. Therefore, the aim of this study is to evaluate the perioperative parameters and treatment-related complications as well as assessing the learning curve of HoLEP for two surgeons who were well experienced in ThuLEP but had not received special training before switching lasers.
Patients and Methods
Study population and data collection
After Institutional Ethics Review Board approval (Nr. 2022–805), patient data were collected from the hospitals database, using the Operation and Procedure Codes for HoLEP. HoLEP procedures were implemented at our tertiary referral center in January 2021. The first 50 consecutive patients of two surgeons who operated HoLEP between January 2021 and January 2022 were enrolled in the study. Both surgeons were well experienced in endoscopic procedures such as transurethral resections of the prostate (TUR-P) and ThuLEP. Surgeon 1 (J.H.) had previously performed >100 TUR-P and >50 ThuLEP and Surgeon 2 (J.v.H.) >100 TUR-P and >100 ThuLEP procedures. Neither surgeon had received any specific training before starting with HoLEP. We evaluated the learning curve of both surgeons.
Parameters
The following preoperative parameters were retrospectively collected from the patients' electronic medical records: age, body mass index (BMI), International Prostate Symptom Score (IPSS), IPSS-related quality of life (IPSS-QoL), International Index of Erectile Function (IIEF), total prostate specific antigen (PSA), peak urinary flow rate (Q-max), post-void residual volume (PVR) urine volume, transrectal ultrasound-determined prostate volume, previous urinary retention, urinary catheter supply, previous medication, oral anticoagulation, and previous prostate surgery. In addition, we recorded the following perioperative parameters: enucleation weight, enucleation time, enucleation efficiency (enucleation weight/enucleation time; g/min), operation time, morcellation efficiency (morcellation weight/morcellation time; g/min), hemoglobin loss, laser time efficiency (laser time/weight; min/g), laser energy efficiency (laser energy/weight; kJ/g), length of hospital stay, and time to catheter removal. Furthermore, transurethral reinterventions and complications according to the Clavien-Dindo classification as well as the Complication Comprehensive Index (CCI) 18 within the first 30 days postoperatively were evaluated.
Technique and laser settings
HoLEP was performed with the Pulse 120 Moses® Holmium Laser (Lumenis, Yokneam Illit, Israel) with a Slimline® 550 Laserfiber. Morcellation was performed using the Piranha® morcellation system (Richard Wolf, Knittlingen, Germany) in combination with a 26F continuous-flow laser resectoscope (Richard Wolf). Surgeons performed the enucleation in a three-lobe, 19 two-lobe, or en-block technique 20 as to the patients' anatomy and personal preference.
In general, Surgeon 1 preferred an en-block technique for the majority of patients, while Surgeon 2 preferred a two-lobe technique. Early apical release and mucosal sparing as described by Saitta et al 20 was performed in the vast majority of cases (100% Surgeon 1 and 62% Surgeon 2). Laser settings for enucleation were 2 J 50 Hz short pulse for Surgeon 1 and 1.2 J 60 Hz short pulse for Surgeon 2, representing the personal preference. Coagulation was performed at 1 J and 40 Hz with long pulse setting for both surgeons.
Statistical analysis
Descriptive statistics were carried out to present the baseline and perioperative characteristics. Quantitative data were expressed as mean and standard deviation, and categorical date as absolute and relative frequencies. The Kruskal–Wallis test was used to compare perioperative characteristics to different experience levels of the two surgeons. Spearman's correlation analysis was performed to analyze the relationship between the variable of interest and the number of surgical cases. All statistical analyses were carried out with JMP v14 (SAS Institute, Cary, NC). The level of significance was set at 0.05.
Results
Baseline characteristics
A total of 100 patients (the first 50 patients of each surgeon), who underwent HoLEP at our department between January 2021 and January 2022 were included in the analyses. Baseline characteristics were similar for both patient collectives (all p > 0.05) and are summarized in Table 1. Twenty and 15 patients were carrying a bladder catheter at the time of admission. Forty-seven (94.0%) and 33 patients (66.0%) had taken an α-blocker before surgery, and 6 (12.0%) and 10 patients (20.0%), respectively, had taken a 5-α-reductase inhibitor. One patient of each surgeon had known prostate cancer (one palliative enucleation, one enucleation before radiotherapy), and one patient of Surgeon 2 had previously undergone prostate surgery (TUR-P).
Baseline Characteristics
BMI = body mass index; IIEF = International Index of Erectile Function; IPSS-QoL = International Prostate Symptom Score-related quality of life; PVR = post-void residual volume; SD = standard deviation; TRUS = transrectal ultrasound.
Perioperative parameters
The perioperative parameters are summarized in Table 2 (all p > 0.05 except for laser energy efficiency p = 0.002). Both surgeons started with an enucleation efficiency of around 1 g/min in their first 10 cases. Neither surgeon reported any intraoperative complications. The pathology report identified incidental prostate cancer in three patients (6.0%) of Surgeon 1 (all T1a, Gleason score 3 + 3) and a B cell lymphoma in one patient. Three patients (6.0%) of Surgeon 2 were also diagnosed with incidental prostate cancer (two patients T1a, Gleason score 3 + 3, one patient T1b, Gleason score 3 + 4).
Perioperative Parameters
Treatment-related adverse events
Surgeon 1 reported four Clavien-Dindo I adverse events (AEs) (urinary retention n = 3, prolonged gross hematuria n = 1), and Surgeon 2 reported two Clavien-Dindo I AEs (urinary retention n = 1, prolonged gross hematuria n = 1). Clavien-Dindo II AEs occurred in one patient of Surgeon 1 (urinary tract infection [UTI] n = 1) and two patients of Surgeon 2 (clot retention n = 1, UTI n = 1), respectively. In the study cohort, there was only one complication (1.0%) requiring reintervention under general anesthesia due to prolonged bleeding. Treatment-related AEs according to the Clavien-Dindo classification are summarized in Table 3 (all p > 0.05). The CCI was 12.9 ± 4.5 for Surgeon 1 and 18.8 ± 4.5 for Surgeon 2.
Overall Treatment-Related Adverse Events According to the Clavien-Dindo Classification and the Complication Comprehensive Index
AEs = adverse event.
Learning curves
Enucleation efficiency
The development of enucleation efficiency was evaluated for each surgeon. Therefore, a Spearman's correlation analysis was performed (Fig. 1). The variables were found to be statistically significantly related (p = 0.0003) and the correlation was positive, meaning that enucleation efficiency increased significantly with the number of cases performed for either surgeon. The correlation between the variables is intermediate (ρ = 0.351).
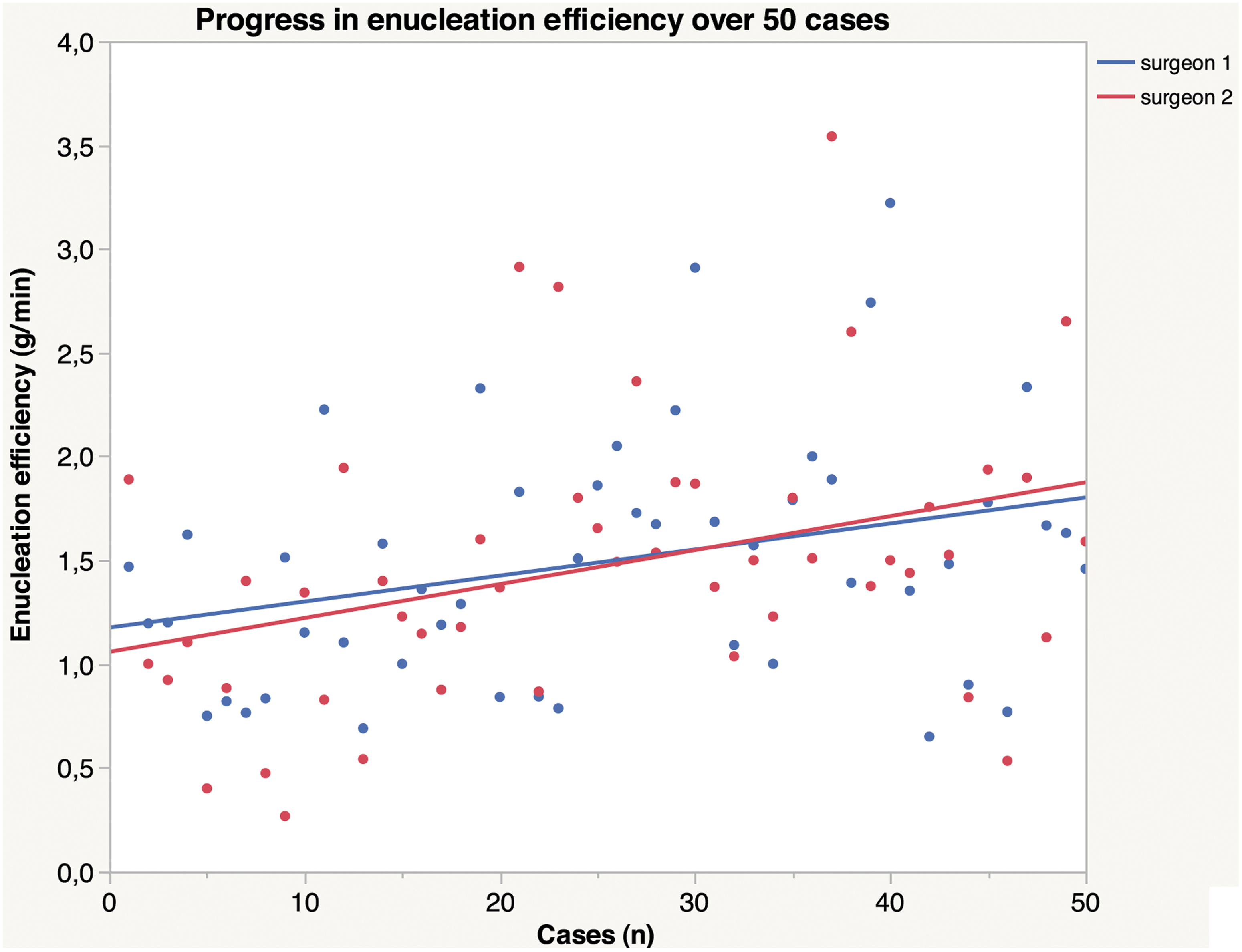
Development in enucleation efficiency: Spearman's correlation analysis. The progress in enucleation efficiency (g/min) over 50 cases of each surgeon is shown. Spearman's correlation analysis was performed. The variables were statistically significantly related (p = 0.0003) and the correlation was positive. The correlation between the variables is medium (Spearman's ρ = 0.351). Color images are available online.
In addition, the enucleation efficiency was evaluated in clusters of 10, using the Kruskal–Wallis test. We found two significantly different case pairs for Surgeon 1 and four case pairs for Surgeon 2 (Fig. 2). Overall, the enucleation efficiency of both surgeons increased significantly (Surgeon 1 p = 0.034, Surgeon 2 p = 0.006) with the number of cases performed, indicating that there was a significant learning curve (Fig. 2).
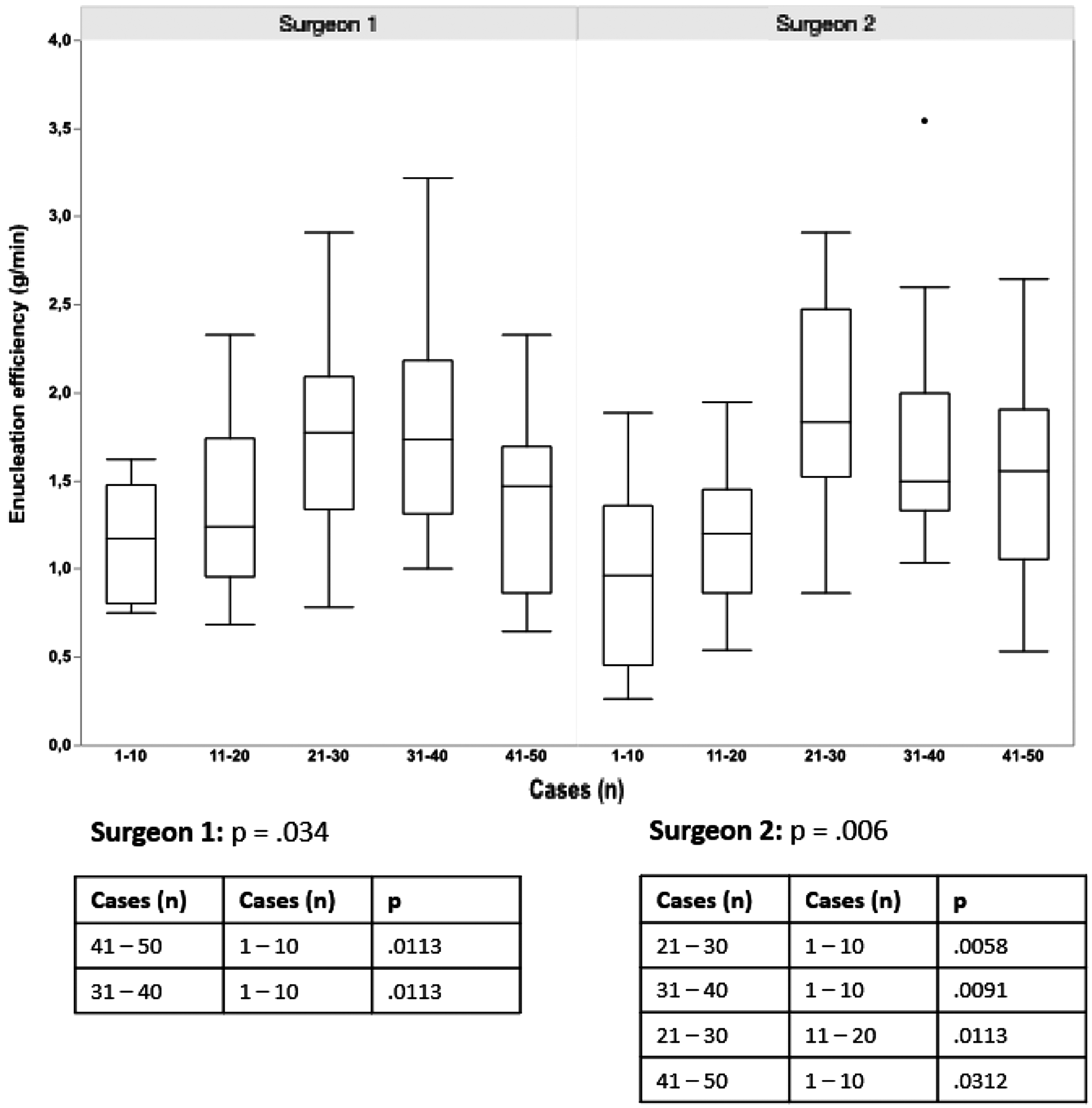
Development in enucleation efficiency
Hemoglobin loss
No significant correlation could be seen between hemoglobin loss and experience according to the Spearman's rank test (p = 0.823, ρ = 0.025).
Morcellation efficiency
There was no significant correlation between morcellation efficiency and experience according to the Spearman's rank test (p = 0.785, ρ = 0.028).
Laser energy efficiency
The laser energy efficiency indicates how many kJ of energy were used per gram of enucleation weight. The Kruskal–Wallis test showed a significant difference only for Surgeon 2 (p = 0.014), but not for Surgeon 1 (p = 0.469). Therefore, only one of the two surgeons was found to have a significant learning curve. Boxplots are shown in Figure 3.

Development in laser energy efficiency. The laser energy efficiency (kJ/g) of different case pairs of 10 cases was compared for both surgeons using the Kruskal–Wallis test. Boxplots, overall significance and the significant case pairs are shown.
Discussion
We evaluated the learning curve of HoLEP in two surgeons with experience in ThuLEP after a change of the laser system in our department in early 2021. The reason for changing the laser system was the superior versatility of the Ho-YAG laser, which enables both endoscopic enucleation of the prostate (EEP) and lithotripsy of urinary stones. We found that a learning curve is present even in surgeons with previous experience in ThuLEP, but that this learning curve is largely limited to the enucleation efficiency, which was at a comparatively high level at baseline, but improved significantly over time. No learning curve was observed for other parameters such as morcellation efficiency, blood loss, or incidence of complications.
The enucleation efficiency is one of the more suitable parameters to evaluate the efficiency of the surgeon performing the enucleation procedure, as it takes into account the prostate volume, which is the main determinator of procedure time. In our series, both surgeons start with an enucleation efficiency of around 1 g/min in their first 10 cases, which is considerably higher than in most published series of surgeons without previous experience in EEP, where the enucleation efficiency was mostly <0.5 g/min. 21,22
Throughout the course of the study, the enucleation efficiency of both surgeons increased up to 1.8 g/min, which is close to 2 g/min, which is generally seen as a benchmark for experts in HoLEP. 23 The enucleation efficiency correlates not only to experience but also inversely to prostate volume, as the area to be detached becomes smaller in correlation with the total volume of the adenoma. 24 This explains why Surgeon 1 was slightly slower in cases 41 to 50 compared to the previous clusters, as the median prostate size in this cluster was below average. The enucleation efficiency will possibly continue to increase slightly after the 50 cases, as Figure 1 suggests. If this should be regarded as part of the learning curve, this is debatable since the curve has already flattened.
There is one outlier in operation time, where one procedure took 262 minutes. This was one of the first cases of HoLEP and involved a large gland of above 250 cm3. Retrospectively, those challenging cases should best be attempted after the surgeon has become reasonably accustomed to the new laser, that is, after at least 10 cases.
Interestingly, an improvement in laser energy efficiency was seen in surgeon 2 but not in surgeon 1. Since both surgeons applied a no touch technique, the laser energy administered does not necessarily correlate with the energy reaching the capsular tissue, since the distance of the laser fiber to the line of attack has a major impact. The laser settings used by surgeon 2 had a higher frequency but a lower energy, requiring the tip of the laser fiber to be closer to the tissue to have the desired thermochemical effect. In combination with the lower mechanical energy due to the lower pulse energy, this might be an explanation why an improvement was seen over time.
It is encouraging that overall complications were low, with UTIs and a failed first voiding attempt being the most common low-grade complications. The overall reintervention rate was extremely low at 1%, where one patient taking anticoagulants developed a bladder tamponade that required cystoscopic evacuation under general anesthesia. These numbers are considerably lower than what might have been expected during the regular learning curve of HoLEP 25 and lower than in most other series of high-volume centers. 26 In our experience, the risk of reintervention is determined not only by the surgery itself but also by the postoperative management, with continuous postoperative irrigation being essential in the first hours after surgery in patients requiring anticoagulants. Therefore, these promising results highlight that the nursing staff was already familiar with the postoperative care of EEP patients, which is a cornerstone for minimizing complications.
Hemoglobin loss was below 1 g/dL throughout the study and was not influenced by experience according to the Spearman's rank test. No transfusions were administrated. This is remarkable given that approximately one third of all patients were taking some form of anticoagulants (28% Surgeon 1 and 36% Surgeon 2), further highlighting the excellent safety profile of HoLEP.
As expected, no change in the morcellation efficiency was noted throughout the study, supporting the assumption that both surgeons had already surpassed the learning curve for this part of the procedure.
In summary, the present data show that there is a laser-specific learning curve, but it is largely limited to the speed of the enucleation part of the procedure and has no impact on blood loss or complications. In addition, both surgeons started with an enucleation speed of >1 g/min, cases and improved further upon that. The authors' personal experience is in line with the data presented.
Subjectively, both surgeons felt that switching between lasers was straightforward and preferred HoLEP to ThuLEP after a few cases. It was our impression that less bleeding occurred since the mechanical energy of the Ho:YAG laser facilitates anatomic dissection of the planes, so penetration into venous sinuses etc. was much less frequent. It should be noted that this observation is not necessarily consistent with current randomized evidence. 13 We found that the overall quality of the enucleation was subjectively slightly higher. On the downside, more care must be taken to stay in the enucleation plane, as leaving the plane can make the procedure difficult and lead to an excessively long operation time. With ThuLEP, which is basically a vapoenucleation, the plane does not have to be adhered to so strictly, as the surgeon can chose to “cut through” the adenoma if the plane is lost.
According to our results, we believe that a surgeon experienced in laser enucleation can start with HoLEP immediately without increasing the risk of complications. However, the authors recommend choosing intermediate size prostates (60–100 g) for the first 10 to 15 cases to get used to the subtle differences between the two lasers before attempting larger glands. Apart from that, we believe that special training, such as mentoring, is probably not necessary when switching lasers, without increasing the risk of complications as shown by our results.
Limitations
As this was a retrospective study, we could not provide a follow-up in the form of patient-reported outcome measures or functional parameters. For the same reason, minor complications that may have been treated elsewhere might have been missed.
Conclusion
Experience with ThuLEP significantly speeds up the learning curve of HoLEP. Nevertheless, a significant learning curve was observed in enucleation efficiency for both surgeons and in laser energy efficiency for one of the two surgeons, indicating that some adaptation is necessary. No improvement could be seen in terms of hemoglobin drop or complications. The incidence of relevant complications and blood loss was extremely low, highlighting the excellent safety profile of the procedure. Overall, switching from ThuLEP to HoLEP is a safe bet.
Footnotes
Authors' Contributions
M.H.: data collection, data analysis, and article writing. B.G.: data analysis, article writing, and editing. J.V.H.: data collection, data analysis, and editing. F.O.H.: data collection and editing. K.F.K.: data collection and editing. M.C.R.-S.: data collection and editing. M.S.M.: supervision and editing. J.H.: conception of the study, supervision, article writing, and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.