
Abstract
Purpose:
To test the safety and feasibility of laser lithotripsy for midsize renal stones using a newly developed robotic retrograde intrarenal surgery (RIRS) system (easyUretero) in a porcine model.
Materials and Methods:
Three urologic surgeons representing three different RIRS experience levels (beginner, intermediate, and expert) participated. Four female pigs (aged 6 months) underwent manual or robotic RIRS. Under general anesthesia, a nephrostomy tract was created ventrally, and calcium stones (diameter, 1.0–1.5 cm) were inserted at renal calices. For manual RIRS, surgeons operated a flexible ureteroscope. For robotic RIRS, the ureteroscope was attached to the robotic slave device. The Auriga XL™ Holmium laser was used for lithotripsy. Lasering and stone retrieval time were measured. Kidneys and ureters were inspected for injury at the end of each session.
Results:
For the expert, both lasering and stone retrieval by manual RIRS were quicker than by robotic RIRS (22.8 ± 11.0 s/stone vs 234.5 ± 102.5 s/stone, p = 0.02; 41.5 ± 0.5 s/stone vs 79.3 ± 8.1 s/stone, p = 0.02). For the intermediate and beginner, lasering and stone retrieval times were not significantly different between manual and robotic procedures (127.8 ± 93.2 s/stone vs 284.8 ± 112.3 s/stone, p = 0.08; 86.0 ± 30.5 s/stone vs 84.1 ± 21.4 s/stone, p = 0.92). All stones were removed. Grade 1 ureteral and renal injuries occurred in both manual RIRS and robotic RIRS.
Conclusions:
The laser lithotripsy using the easyUretero robotic system is safe and feasible in a porcine model, even for less-experienced surgeons.
Introduction
Retrograde intrarenal surgery (RIRS) using a flexible ureteroscope is an attractive alternative to conventional percutaneous nephrolithotomy or shockwave lithotripsy for renal stone disease. 1,2 RIRS is considered less morbid to percutaneous nephrolithotomy in terms of blood loss and adjacent organ injuries and can achieve higher stone-free rates than shockwave lithotripsy. 3 It is now considered standard treatment for 1 cm or smaller renal calculi together with shockwave lithotripsy. 4
Robotic surgical systems have revolutionized endoscopic urology, providing a diverse degree of motions at the operative field and better ergonomics for surgeons than manual laparoscopy. 5 It has been adopted for most oncological urologic surgeries such as prostatectomy, partial nephrectomy, and cystectomy. 6 In urinary stone disease, RIRS using a flexible ureteroscope has been also considered a challenging and standard technique with the advancement of optical technology. 7,8 In particular, RIRS laser lithotripsy requires the presence of two people: the operator, the primary surgeon, who controls the flexible ureteroscope to target the stone, and the assistant who activates stone basket.
Therefore, to seamlessly perform RIRS, highly coordinated movement between the operator and assistant is required. In other words, the surgical outcomes may be affected by the proficiency of the assistant, as well as that of the primary surgeon. As presented in previous robotic systems, robotic assistance greatly reduces the dependence on the assistant surgeon's ability. In this regard, the adoption of a robotic system can greatly advance RIRS lithotripsy and stone retrieval. Yet, only a few surgical robots have been tested for RIRS. Roboflex Avicenna™ (Elmed Medical Systems, Ankara, Turkey) is a master-slave robotic system that was first clinically tested for RIRS. 9 In addition, the earlier developed robot-assisted RIRS exhibited unique advantages such as better ergonomics, tremor elimination, superior vision was reported, and decreased radiation exposure. 10 –12
In this study, we introduce a new master-slave robotic RIRS system easyUretero (ROEN Surgical, Inc., Daejeon, Korea) (Fig. 1) and describe our initial experience in a porcine renal stone model. The system utilizes the popular single-use flexible ureteroscope LithoVue™ and the Auriga XL™ Holmium laser (Boston Scientific, Marlborough, MA), assuring easy adoption in a clinical situation. At the master console, the surgeon can control simultaneously the flexible ureteroscope (deflection, rotation, and forward and backward movement), stone basket (open and close and forward and backward movement), or laser fiber (forward and backward movement and firing) at the console without the need for a second person. In this study, we aimed to assess the safety and feasibility of robotic RIRS laser lithotripsy and stone retrieval for midsize kidney stones in a porcine model.

System configuration of easyUretero.
Materials and Methods
Robotic RIRS system easyUretero
The easyUretero by ROEN Surgical, Inc., is a master-slave robot system for RIRS. The slave robot can mount a commercial flexible ureteroscope. The master console provides a handle that controls a flexible ureteroscope, a stone basket, and laser fiber with a single operator in a sitting position. A radiation shield barrier can be placed at the console. Control of the scope and laser fiber can be fine-tuned through motion scaling. The robot system has automation capability that can record and play the ureteroscope motion, which can be effectively utilized in a repetitive task such as multiple stone retrieval.
In addition, the robot system provides a safety function that detects the grasping and retrieval of an oversized stone to avoid the ureteral injury. The grasped stone size is automatically calculated by using the predetermined relationship between the amount of basket opening and the stone size. Also, the robot has a sensor that detects physical collision between ureteral access sheath tip and the grasped stone.
Population and participants
The Institutional Animal Care and Use Committee of Yonsei University Health System (Seoul, Korea) approved the study protocol (Approval No. 2020-0309). Four female pigs aged 6 months (weight, 45.7 ± 2.1 kg) acclimated for 7 to 10 days in our animal facility (Department of Laboratory Animal Medicine, Medical Research Center, Yonsei University Health System, Seoul, Korea) were used for the evaluation. Three urologic surgeons participated, each representing a different RIRS experience level: beginner, <100 procedures; intermediate, 100 to 400 procedures; and expert, >400 procedures.
Porcine renal stone model
Animal sedation was achieved using tiletamine (Zoletil 50; Virbac, Carros, France) 5 mg/kg and xylazine (Rompun; Bayer Korea Ltd., Seoul, Korea) 2 mg/kg. Mechanical ventilation was applied to maintain respiration during the study, as the animal received anesthesia with 2% isoflurane (Forane; JW Pharmaceutical, Seoul, Korea) and underwent muscle relaxation using 4 mg vecuronium bromide (0.10 mg/kg). Each anesthetized animal was placed in the dorsal lithotomy position. For nephrostomy, a Chiba biopsy needle with an echo tip (18-gauge and 20 cm; Cook Medical, Bloomington, IN) was used under ultrasonography guidance (Fig. 2).
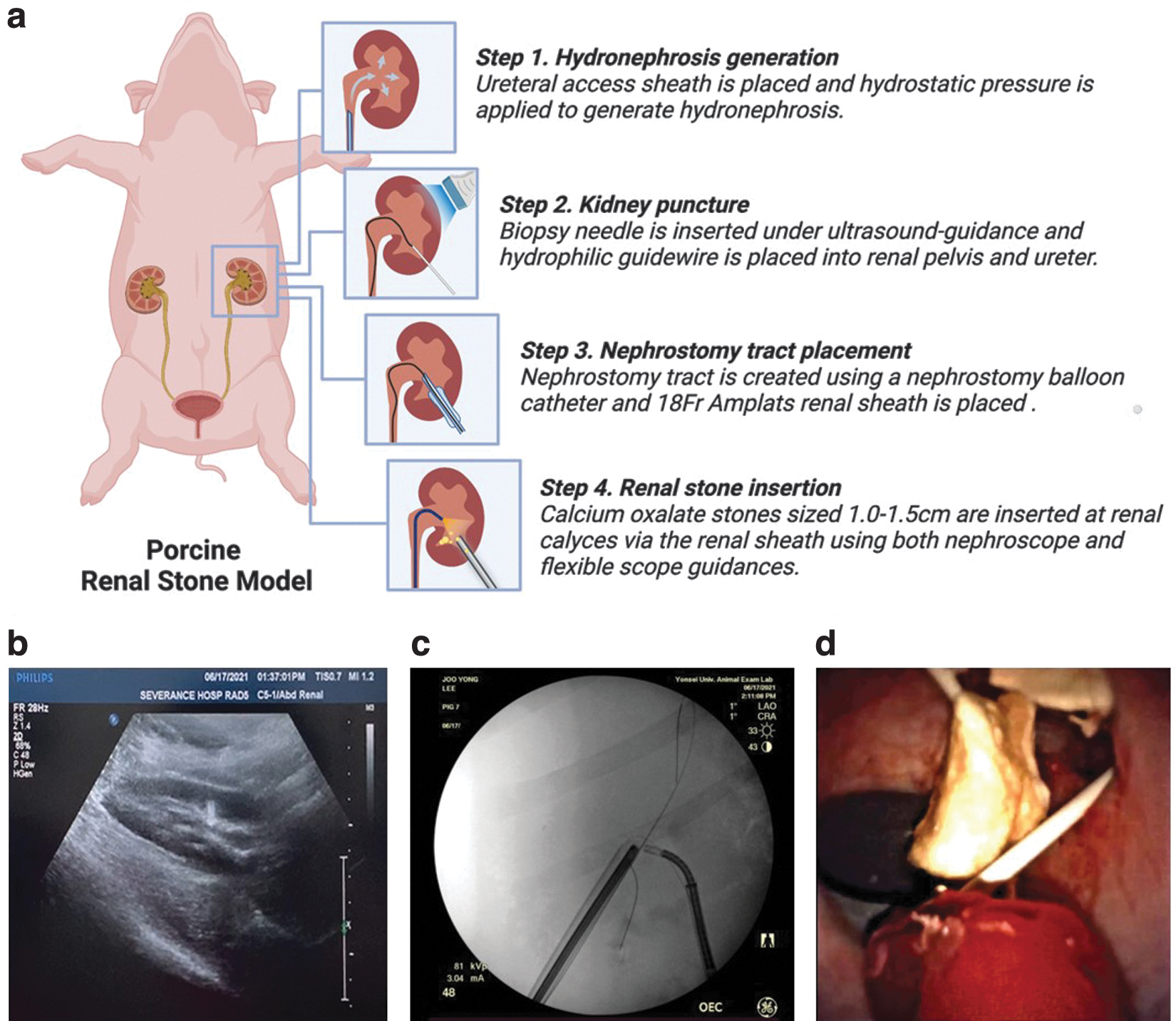
Porcine renal stone model.
After puncture into the intrarenal space, a hydrophilic guidewire was inserted into the kidney and ureter, and a nephrostomy tract was created using Utraxx™ nephrostomy balloon catheter (18F; Cook Medical). Calcium oxalate stones sized 1.0 to 1.5 cm were inserted at renal calices through an 18F Amplatz renal sheath using a 15F mini nephroscope (Olympus, Tokyo, Japan). For the retrograde robotic approach, a ureteral access sheath (11/13F, 36 cm, Navigator HD; Boston Scientific) was placed under fluoroscopic guidance through the hydrophilic guidewire. The ureteral assess sheath tip was located right below the ureteropelvic junction.
Surgical procedures
Four animals underwent surgery, two with manual RIRS and the other two with robotic RIRS. Each of the three surgeon participants performed a portion of the surgery in each animal in randomized order. For manual RIRS, a surgeon operated the LithoVue flexible ureteroscope and an assistant operated the stone basket and laser fiber. For robotic RIRS, the LithoVue, a modified stone basket, and a laser fiber were attached to the robotic slave device, and a surgeon operated the LithoVue, stone basket, and laser fiber remotely at the master console. Per each session, the surgeons performed laser lithotripsy by using AurigaTM XL and retrieval of the fragmented stones. We used fixed lasering power (800 mJ, 12 Hz) during all procedures.
Assessment and statistical analyses
We compared lasering and stone retrieval time between manual and robotic RIRSs, stratified by the surgeon's experience level. Lasering time was defined as the time taken to crush a stone into fragments with a size smaller than the inner diameter of the access sheath. Stone retrieval time was defined by the total time spent to remove stone fragments using the stone basket divided by the number of removed stone fragments. In addition, the time included the time to empty the basket outside the ureteral access sheath and relocate it to kidney. Stone retrieval beginning and end were defined by when the flexible scope is placed into the kidney and when the last stone fragment is removed from the access sheath.
Frequency and grade of ureteral and renal injuries between manual and robotic RIRSs were also compared. Injuries were graded using the criteria proposed by Traxer and Thomas. 13 All pigs were exsanguinated through the cephalic vein before and after RIRS. Hemoglobin and serum creatinine were measured through blood collection and analyzed for each group of manual and robotic RIRSs. Finally, the surgeon's workload was assessed using the validated National Aeronautics and Space Administration (NASA) task load index (TLX) questionnaire, which measures the surgeons' self-reported performance, effort, frustration, and mental, physical, and temporal demands of the task. 14
Statistical analysis of the achieved data was performed using GraphPad Prism (version 9.0; GRAPH PAD software, Inc., CA). Values are presented as the mean ± standard deviation. Analysis was conducted using paired or unpaired t-tests with Welch's correction; a p-value <0.05 was considered significant.
Results
Operative time
The operative record is summarized in Table 1. The average docking time per case was 2.6 ± 0.4 minutes in this experiment. This time consists of slave unit approximation to operation bed and attachment of ureteral access sheath and LithoVue to the slave unit. This time does not include initial ureteral access sheath placement procedure. For the RIRS expert, both lasering and stone retrieval by manual RIRS were quicker than robotic RIRS (22.8 ± 11.0 s/stone vs 234.5 ± 102.5 s/stone, p = 0.02; 41.5 ± 0.5 s/stone vs 79.3 ± 8.1 s/stone, p = 0.02). For the RIRS intermediate and beginner, lasering time and stone retrieval time were not significantly different between manual and robotic procedures (127.8 ± 93.2 s/stone vs 241.8 s/stone, p = 0.14; 85 ± 30.5 s/stone vs 96.1 ± 32.7 s/stone, p = 0.63) (Table 1). All stones were removed.
Outcomes After Manual vs Robotic Retrograde Intrarenal Surgery by Surgeons of Different Experience Levels in a Porcine Renal Stone Model
RIRS = retrograde intrarenal surgery.
Operative complications
A grade 1 ureteral injury and a grade 1 renal injury occurred in manual cases. Similarly, a grade 1 ureteral injury and a grade 1 renal injury occurred in robotic cases (Table 1). Video review identified that all the ureteral injuries were considered to have occurred during the access sheath insertion, which was performed manually in both types of RIRSs. The renal mucosal injury was caused by the direct firing of the laser. At postoperative days, there was no sign of discomfort or pain among the animals. In addition, hemoglobin and serum creatinine levels were measured before and after surgery, and a trend of increased creatinine levels was observed in all tested animals (Table 2).
Perioperative Changes in Hemoglobin and Serum Creatinine Levels
Cr = creatinine; Hgb = hemoglobin.
Surgeon self-reported outcomes
Answers to the self-reported NASA-TLX questionnaire revealed that across all aspects of the surgery, surgeons considered robotic RIRS to require particularly less physical demand than manual RIRS (Fig. 3).

Surgeon answers to self-reported Task Load Index Questionnaire by RIRS experience level. Each dot represents an answer from one of the three surgeons (RIRS expert, red; intermediate, green; and beginner, blue) who participated in this experiment. RIRS = retrograde intrarenal surgery.
Discussion
We performed RIRS in a live porcine renal stone model using a new master-slave robot-assisted flexible ureteroscope system. Robotic RIRS was feasible and safe, provided ergonomic benefits, and showed potential as an alternative to the conventional manual RIRS. In particular, surgeons with little experience with a flexible ureteroscope recorded similar surgery times regardless of performing robotic or manual RIRS. Before the animal experiment, all the surgeons underwent robot console training that consisted of scope handling and manipulating basket and laser fiber. Considering that average total training time of each surgeon was ∼5 hours, we can expect the possibility of easy and fast learning through the proposed robotic assistance.
To test the feasibility of manual or robot-assisted laser lithotripsy, we developed a live porcine renal stone model. Our model has several benefits that may be useful for experimental or educational purposes. First, it is a one-stage procedure: both renal stone placement and lithotripsy are performed in a single anesthesia session, which minimizes animal stress and experimental costs. Second, because the nephrostomy tract is placed ventrally, there is no need to change position. Third, additional renal stones can be inserted through the tract whenever necessary. Finally, we used an 18F renal Amplantz sheath, which allows passing of as much as 1-cm round stones or larger oblique stones.
To proceed with ease, we utilized a ureteral access sheath and a flexible ureteroscope thoroughly: (1) renal pelvis dilatation by hydrostatic pressure helps the initial needle puncture; (2) direct visualization of calices helps guidewire placement and tract dilation; and (3) combined visualization with a nephroscope helps placing stones in renal calices. To maintain patency of the nephrostomy tract, we used two guidewires. No significant renal function decline or hemodynamic event was observed perioperatively.
Introduction of the da Vinci robotic system (Intuitive Surgical, Inc., Sunnyvale, CA) in laparoscopic surgery has provided many benefits, such as decreased muscle fatigue and relatively shorter learning periods than manual laparoscopy. 15 –17 Theoretically, an “equivalent of the da Vinci robotic system” in endoscopic surgery could bring such advantages to surgeons—better ergonomics, limitless motion, or stabilization of the manipulator and monitor. 6,18 –20 In our experiment, robotic assistance was particularly effective during lasering because the flexible ureteroscope head can be stably positioned, thus allowing surgeons to focus on laser shooting. This benefit was reflected in the self-reported outcomes, as surgeons documented less pain and discomfort during manipulation of devices and overall less physical demand in robotic RIRS than in the manual procedure.
In our view, the expertise in the field of stone endoscopic surgery was gained through the sacrifice of the operator's enduring exposure to radiation and prolonged discomfort. If the new endoscopic robot advances to a sufficiently mature level of technology, it may help young urologists become experts in stone endoscopy, even as avoiding such a series of sacrifices.
For urologists who have already reached the professional level, it is expected to be an attractive enough benefit to reduce the repetitive and chronic stress that they are putting on their bodies. As in the burn-out syndrome of high-end workers, accumulation of physical and mental stress at work can eventually lead to a decline in job satisfaction and early retirement. Given that the innovation brought about by laparoscopic surgery robots has helped patients as well as doctors and other assistants, the stone endoscopy robots will ultimately improve the work potential of endourologists.
In RIRS laser lithotripsy, three operating components are required: flexible ureteroscope, laser fiber, and stone basket. Therefore, the surgery is generally considered a two-person procedure. For the LithoVue flexible ureteroscope, an optional retrieval deployment device was developed to improve task completion time when handled by a single surgeon. However, muscle fatigue attributable to increased device weight can be an issue. 21 Avicenna Roboflex (ELMED™) is the first robotic system developed for RIRS application. 9 One of the benefits of the Roboflex system is that its operator can control laser intensity, firing, and irrigation pump intensity at the console, in addition to ureteroscope deflection and rotation. 22 However, basket handling was not incorporated in the system, which necessitates one additional field operator.
By contrast, the easyUretero system enables control of both the ureteroscope and the stone basket at the console, turning essentially a two-person task into a one-person operation. This was one of the largest advantages noted by participating surgeons with minimal or intermediate RIRS experience. The primary role of the assistant at the operating field was to collect stone fragments, switch laser fiber from/to stone basket, or reengage the ureteroscope to assess sheath entrance. These works do not require coordinated motion. The assistant used the LithoVue monitor for observation, and there were minimal communication issues between the operator and the assistant.
In addition, the robotic surgical system can be beneficial for training purposes. 23,24 The new system is capable of recording not only videos but also motion input, which can greatly facilitate the learning process by reviewing the procedure on the monitor and in the field together, in all view angles. In this regard, a robot endoscopic simulator can also be helpful for training, which minimizes animal sacrifice. 25
A few limitations of the tested robot were noted. First, the master and slave system require a large space, similar to the da Vinci console and slave system, which may increase operative flow disruption in some small operating rooms. 26 Second, a millisecond delay was observed between the operator input and the actual scope motion. We did not experience any issue owing to the delay during this trial, yet there is a room for improvement. Third, although all procedures occurring within the access sheath or operative field (renal pelvis) did not need assistance, manual assistance was needed for retrieval of stone fragments outside, installation of the stone basket or laser fiber, and reinsertion of the scope into the access sheath. It was again similar to robotic laparoscopic surgery where the assistant surgeon or nurse needs to insert the robotic arm into the laparoscopic port.
Fourth, the number of surgeons in this study was limited. A larger sample size of surgeons would be necessary for rigorous and comprehensive validation of this system, including statistical subanalysis and learning curve analysis. However, given the steps taken to limit study bias, we believe the results of this initial study validate the feasibility and safety of the system in animals.
Conclusions
The easyUretero robotic RIRS system is feasible and safe in animals undergoing laser lithotripsy, even for less-experienced surgeons. A clinical trial is planned to confirm the feasibility of the system in humans.
Footnotes
Authors' Contributions
Conception and design: J.K., D.S.K., and J.Y.L. Data acquisition: H.H., J.K., Y.J.M., H.D.J., B.C., J.H., and J.Y.L. Data analysis and interpretation: J.K., B.C., and J.H. Drafting the article: H.H., H.D.J., and J.Y.L. Critical revision of the article for scientific and factual content: H.H., J.K., and J.Y.L. Statistical analysis: H.H. Supervision: S.Y.C., D.S.K., and J.Y.L.
Acknowledgments
The authors deeply appreciate Se Hoon Kim, DVM, and Gyuri Park, DVM, from the Department of Laboratory Animal Resources at Yonsei Biomedical Research Institute for the support of animal care and perioperative hematological examination and Hyun Se Seo and Sukju Kang of ROEN Surgical, Inc., for the technical support during the experiment.
Author Disclosure Statement
H.D.J., Y.J.M., H.H., and J.Y.L. have received research grants from ROEN Surgical, Inc., for this work. J.Y.L. and S.Y.C. hold a position on the advisory board of ROEN Surgical, Inc., J.K., B.C., and D.-S.K. have stock ownership of ROEN Surgical, Inc., J.H. declares no potential conflict of interests.
Funding Information
This work was supported by ROEN Surgical, Inc. Grant number: 2020-31-1550.