
Abstract
Purpose:
This study aimed to compare different laser systems for the enucleation of benign prostate hyperplasia.
Methods:
Randomized controlled trials (RCTs) on different lasers for prostate enucleation were searched from PubMed, Embase, and CNKI databases. Pairwise and network meta-analyis (NMA) were performed to analyze the outcome regarding surgery time, complications, short-term postvoid residual (PVR), long-term PVR, and short-term international prostate symptom score (IPSS), long-term IPSS, short-term maximum urine flow rate (Qmax), and long-term Qmax. RevMan software was used for paired meta-analysis. Considering the variance uncertainty caused by the different source regions of RCTs and the different primary conditions of surgeons and patients, this study uses Bayesian NMA conducted with ADDIS software to compare different treatment methods indirectly. Node-splitting analysis was used to test inconsistency for closed-loop indirect comparison.
Results:
Nine studies were included in this study, involving four types of lasers: diode laser, holmium laser, thulium laser, and greenlight laser. In safety paired meta-analysis, holmium laser could bring more complication risk than thulium laser (odds ratio: 2.70, 95% confidential interval [CI]: 1.79–4.00, p < 0.001), and no other significant result was detected. In the efficacy comparisons, holmium laser could offer better postoperative long-term PVR (standardized mean difference [SMD]: −0.35, 95%CI: −0.62, −0.09, p = 0.011), better postoperative long-term IPSS (SMD: −0.30, 95%CI: −0.57, −0.04, p = 0.011), better postoperative short-term Qmax (SMD: 0.44, 95%CI: 0.17, 0.70, p = 0.001) compared with greenlight laser. According to the results of NMA, greenlight laser may bring more complication risks when applied to prostate enucleation than the other three lasers. Thulium laser may be the recommended laser system for prostate enucleation.
Conclusion:
Thulium laser may be the recommended laser system since it can bring less complication risk with comparable efficacy. More RCTs are still needed to validate this study.
Introduction
With the increasing number of aging populations worldwide, more older men have experienced lower urinary tract symptoms caused by benign prostate hyperplasia (BPH). 1 Further surgical therapy is necessary to improve the quality of life for BPH patients who continue to experience frequent urine retention, hematuria, and urinary tract infections despite oral medications. 2 In the surgical management of BPH, the most common procedures are transurethral incision of the prostate, transurethral resection of the prostate (TURP), enucleation, and vaporization. 2 Currently, TURP is the procedure that is most frequently performed to treat BPH around the globe. 3 Even though TURP can provide an outstanding balance between the treatment of lower urinary tract symptoms and cost, it is nevertheless challenged by many other developing technologies, such as prostate enucleation. 4 In clinical settings, plasmakinetic enucleation, holmium laser enucleation, thulium laser enucleation, diode laser enucleation, and green light laser enucleation are frequently employed to remove prostate tissue. 5,6
Which energy device is better suited for prostate enucleation has been extensively discussed in articles. 7 The initial conclusion at the time was that surgical methods and anatomical knowledge were significantly more significant than the types of energy devices. 2,8 The fact that more randomized controlled trials (RCTs) have been published recently, however, suggests that there may still be variations in the security and effectiveness of various laser systems for prostate enucleation. 9 To better assess the safety and efficacy of prostate enucleation, the goal of this study was to pool all published RCTs using various lasers using the network meta-analysis (NMA) method. This work used the Bayesian NMA method to covertly compare various therapeutic modalities, taking into account the variance uncertainty brought on by the various source regions of RCTs and the various fundamental conditions of surgeons and patients.
Materials and Methods
This NMA was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline for NMA. 10
The selection criteria applied in this analysis followed PICO criteria as follows: Patients: Patients with benign prostatic hyperplasia requiring surgical intervention were included. There were no restrictions on patient age, prostate size, or preoperative PSA level. Intervention: Prostate enucleation surgery using a specific laser as the primary energy device. Studies that applied combined techniques were excluded. Comparators: Prostate enucleation surgery using another laser as the primary energy device. Comparisons between laser and other techniques such as plasma kinetic resection or bipolar plasma kinetic enucleation should be excluded. Although NMA can use other surgical techniques as nodes for indirect comparisons, the inclusion of only RCTs involving laser devices can reduce statistical bias due to transitivity. Outcomes: Surgery time, complications, postvoid residual (PVR), international prostate symptom score (IPSS), and maximum urine flow rate (Qmax) should be reported in the included studies. Study design: Only two or multiple arm RCTs should be included in this analysis.
If one trial or relative cohort was reported in more than one publication, the higher quality studies should be included to avoid any potential reporting bias.
Two independent authors extracted the data using a unified standard. The extracted data were as follows: name of the first author, publication year, country of responding author, the sample size of each group of included study, patient age of each group, the prostate volume of each group, laser equipment parameters of each included studies, follow-up schedules, outcome information such as surgery time, complications, PVR, IPSS, and Qmax.
Two reviewers independently performed a study quality assessment by using Cochrane risk-of-bias tool. Six main domains were assessed: the randomization process, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting. Disagreements were resolved by discussion between quality reviewers and the corresponding author.
Paired meta-analysis was performed by using RevMan V5.4.1 software. The standardized mean difference (SMD) was calculated and synthesized as an estimate for a continuous variable (surgery time, PVR, IPSS, Qmax). The odds ratio (OR) was synthesized for discontinuous variables (complications). In this analysis, since different follow-up time points were reported in different included studies, we mainly selected two time points to compare short-term and long-term efficacy. Three months after surgery was the main time point for short-term efficacy comparison. If a study did not report follow-up information 3 months after surgery, the time point closest to 3 months was selected as the short-term efficacy evaluation time point. Similar principles have also been applied in the comparison of long-term efficacy. This study's time point of long-term efficacy was 12 months after surgery.
The NMA in this analysis was based on the Bayesian random-effects model and was conducted with the ADDIS V1.16.8 with the assistance of “gemtc” and “rjags” packages in R v4.0.5. For a closed-loop network with both direct and indirect comparisons, the node-splitting analysis was used to evaluate the consistency. If there was no significant inconsistency (p > 0.05), a consistency model was applied for this NMA. Otherwise, an inconsistency model was used for evaluation, and the sources of inconsistency were also analyzed. In the NMA analysis of this study, the potential scale reduction factor (PSRF) was calculated to evaluate the degree of convergence of the model. If the PSRF is close to 1, the model was considered to have good convergence, and the consistency model could be applied to obtain relatively stable results. The threshold of PSRF was set at 1.02 in this study. The ranking probability of each laser for different outcomes after prostate enucleation was also estimated by using ADDIS. Benefit–risk analysis was also carried out with ADDIS v1.16.8 software based on the stochastic multicriteria acceptability analysis (SMAA) model.
Results
After carefully searching PubMed, Embase, and CNKI, there were 402 candidate studies identified. After removing 133 duplicate records, 269 studies entered the title screening stage. One hundred forty-two records were not related to the topic we were concerned about. Seventy-one studies were reviews, comments, or basic research. Three studies were excluded in the abstract and full-text reviewing stage since they discussed the MOSES technique. The detailed flow chart is shown in Figure 1. According to Cochrane tools, the risk of bias assessment indicated that three studies had a high risk of performance bias (Supplementary Fig. S1).
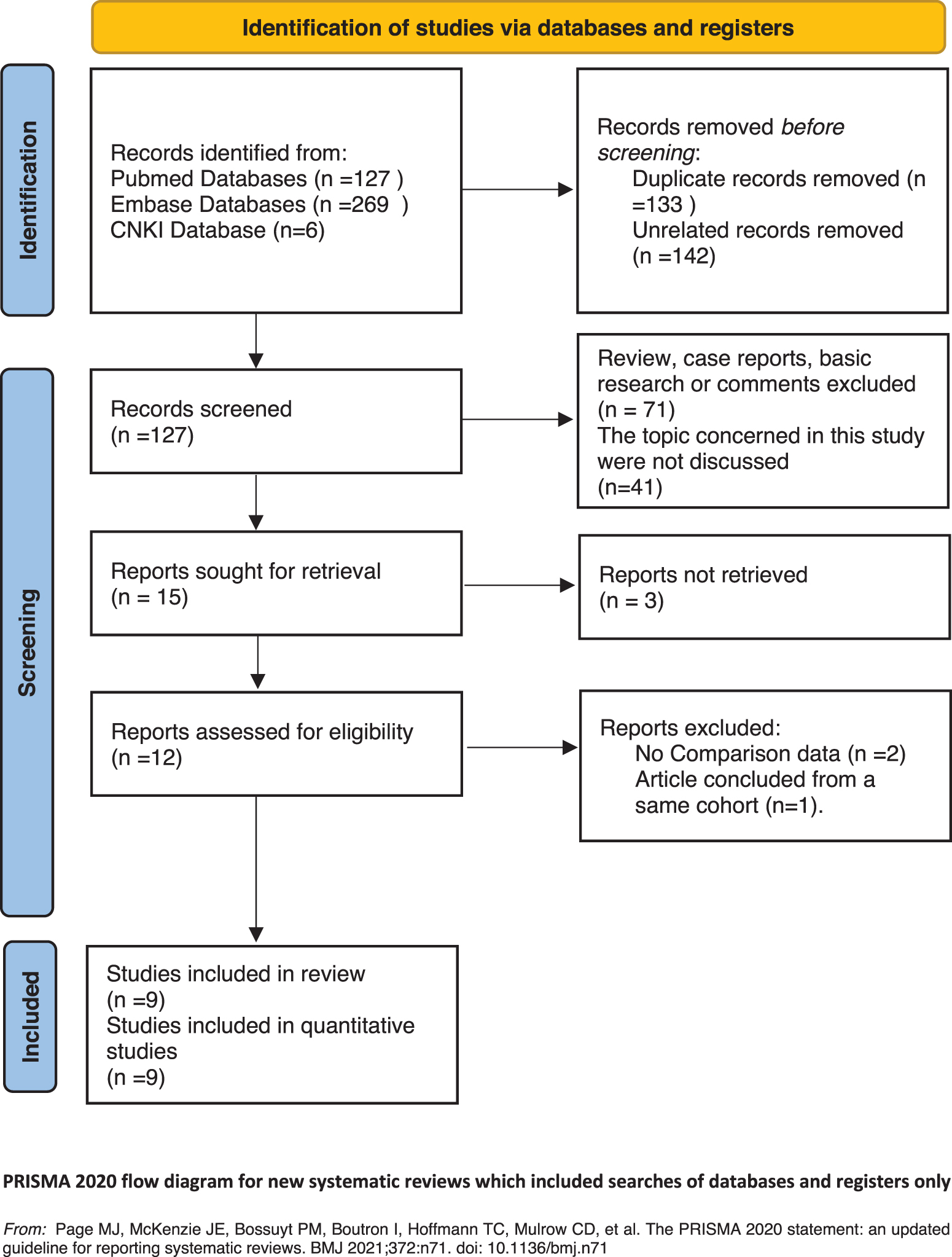
The literature screening flow chart. Color images are available online.
The basic characteristics of the nine included studies are shown in Table 1. All nine included studies were published in recent 10 years. One study was concerned with the comparison between diode laser and thulium laser used in prostate enucleation. 11 One study compared diode laser and holmium laser. 12 Five studies discussed the comparison between holmium laser and thulium laser. 13 –17 Two studies were concerned with comparing holmium laser and greenlight laser. 9,18 The follow-up time of included studies ranged from 1 to 36 months, and not all the included studies offered both short-term and long-term efficacy outcomes. NMA was performed to compare the different laser systems in prostate enucleation for different outcomes in the diode, holmium, thulium, and greenlight laser (Fig. 2). Each node represents one laser system with its name, and connections between nodes represent current published direct comparisons. The thickness of the connections varied according to the number of studies included in the comparison.

Network comparing the different laser systems in prostate enucleation.
Characteristics of Included Studies
NR = not reported.
The results of the pairwise meta-analysis between other laser systems and holmium laser, which is the most commonly used laser system, indicated that there were no significant differences in the surgery time (p = 0.462 for a diode laser, p = 0.744 for greenlight laser, p = 0.258 for thulium laser), postoperative short-term PVR (p = 0.867 for a diode laser, p = 0.258 for greenlight laser, p = 0.514 for thulium laser), postoperative short-term IPSS (p = 0.867 for a diode laser, p = 0.312 for greenlight laser, p = 0.932 for thulium laser), and postoperative long-term Qmax (p = 0.614 for a diode laser, p = 0.137 for greenlight laser, p = 0.722 for thulium laser). Thulium laser could offer significantly less risk for complication after surgery than holmium laser (holmium laser vs thulium laser: OR = 2.70, 95% confidential interval [CI]: 1.79–4.00, p < 0.001).
Compared with the holmium laser, the greenlight laser shows a clear disadvantage in complication risk (holmium laser vs greenlight laser: OR = 0.48, 95%CI: 0.26–0.87, p = 0.019), postoperative long-term PVR (holmium laser vs greenlight laser: SMD = −0.35, 95%CI: −0.62, −0.09, p = 0.011), postoperative long-term IPSS (holmium laser vs greenlight laser: SMD = −0.30, 95%CI: −0.57, −0.04, p = 0.029), and postoperative short-term Qmax (holmium laser vs greenlight laser: SMD = 0.44, 95%CI: 0.17–0.70, p = 0.001). Detailed paired meta-analysis results are shown in Table 2.
Paired Meta-Analysis Between Different Laser Systems and Holmium Laser Results Based on Random-Effects Model
The direction of comparison is comparator vs treatment.
CI = confidential interval; IPSS = international prostate symptom score; OR = odds ratio; PVR = postvoid residual; Qmax = maximum urine flow rate; SMD = standardized mean difference.
Before NMA, we first performed node-splitting analysis to detect inconsistencies between direct and indirect comparisons between each laser system. According to the node splitting analysis results (Table 3), we found that in the all closed-loop comparison, no significant inconsistency was found. Therefore, a consistency model should be applied. For other nonclosed loop comparisons, consistency and inconsistency models were performed to offer more information.
Node-Splitting Analysis of Inconsistency
Number of chains = 4, tuning iterations = 20,000, simulation iterations = 50,000, thinning interval = 10, inference samples = 10,000, variance scaling factor = 2.5.
MD = mean difference.
In the NMA (Table 4), we can find that the holmium laser and greenlight laser system could introduce more complication risk after prostate enucleation compared with the thulium laser and greenlight laser might have the highest risk. For postoperative short-term Qmax, greenlight laser also had the most negative effects. All analyses based on the inconsistency model were similar to those of the consistency model, with no significant differences in postoperative long-term PVR, postoperative long-term IPSS, and postoperative long-term Qmax among the four different lasers (Table 4, inconsistency model analysis part). The treatment safety and efficacy rankings of the different laser systems in prostate enucleation are displayed in Figure 3 (complication ranking) and 4 (efficacy ranking). According to the ranking results, greenlight laser might have minimal safety and efficacy simultaneously. Thulium laser has the best safety performance with comparable efficacy compared with the other three laser systems (Figure 3, Figure 4).

Ranking probability of each laser effect on complication. Color images are available online.

Ranking probability of each laser effect on efficacy.
Network Meta-Analysis Results Based on Consistency and Inconsistency Model
Bold means statistical significance..
Number of chains = 4, tuning iterations = 20,000, simulation iterations = 50,000, thinning interval = 10, inference samples = 10,000, variance scaling factor = 2.5.
MD = mean difference; CI = confidential interval; OR= odds ratio; IPSS = international prostate symptom score; PVR = postvoid residual; Qmax = maximum urine flow rate; RR = relative risk.
The SMAA model was used for benefit–risk analysis in this analysis. 19 When considering all operation time, complication, short-term efficacy, and long-term efficacy outcomes among four types of enucleation techniques, thulium laser enucleation may still be the best technique to obtain a benefit–risk balancing outcome (Fig. 5).

Benefit and risk analysis based on complication and efficacy. Color images are available online.
Discussion
The key to managing lower urinary tract symptoms and avoiding postoperative complications in BPH patients is safe and successful excision of hyperplastic prostate glands. 20 Although several different kinds of lasers have been used for prostate enucleation, their effectiveness has not been properly evaluated. Previous literature has pointed out that indirect comparisons may lead to less bias than direct comparisons. 21 Therefore, the objective of this NMA was to combine direct and indirect evidence to choose the best laser system for prostate enucleation. In this NMA, we discovered that the thulium laser may have the highest safety performance and the greenlight laser may have the worst safety and efficacy performance in prostate enucleation.
One of the main lower urinary tract symptoms in BPH patients is the persistent increase in the volume of leftover urine in the bladder due to the constriction of the urethra by the hyperplastic prostate glands. BPH patients who were unable to benefit from pharmacological treatment must undergo surgery to relieve the urethral tightness caused by the hyperplastic prostate gland. 22 These four-key outcomes—surgery time, complication, PVR, IPSS, and Qmax—were routinely utilized essential indicators for assessing the surgical therapy of BPH in this study. 23,24
Diode lasers did not exhibit statistically significant advantages or drawbacks over other types of lasers in this NMA in terms of safety and efficacy. This conclusion remains consistent with previous reports. 12 The diode laser has the strongest tissue penetration capabilities of the four lasers examined in this study, with an effective distance of 5 mm. 25 Its capacity to harm the prostate's surgical capsule when used for prostate enucleation cannot be disregarded. Nevertheless, this study did not find a significant difference in complications caused by diode lasers, which may need to be confirmed by other RCTs. However, while diode lasers do not have significant advantages in medical performance when compared with other laser generators, such as holmium lasers, they do have the physical properties of high energy conversion efficiency, small size, and long life, which may contribute to the further application of diode lasers in the medical field.
The holmium laser, a laser that is frequently utilized in the medical industry, has a long history of being a safe and dependable source of energy. 5 Holmium laser enucleation is the most researched method now available for removing the prostate, and numerous RCTs that compared it with various energy systems have been published. In this NMA, which served as the basis of comparison, we discovered that when used for prostate enucleation, holmium lasers could provide a higher risk of complications than thulium lasers. The holmium laser's physical characteristics need to be examined to determine the cause of this phenomena. Holmium lasers operate in a pulsed form, which could cause more harm and mechanical impacts. The holmium laser has a wavelength of roughly 2140 nm and can penetrate tissue for 0.4 to 0.5 mm, which is substantially longer than the 0.1 to 0.2 mm of the thulium laser. There is a greater chance that the prostate will be damaged during enucleation, increasing the risk of intraoperative and postoperative complication. 5,6
One of the most recent lasers utilized in prostate enucleation is the greenlight laser, and relevant clinical trials were carried out around 2010. 26 It had the weakest medical performance, safety, and efficacy of the four lasers in this NMA. The greenlight laser is one of the lasers with good tissue penetration performance, according to an investigation of physical parameters. The thermodynamic conduction distance is 1–2 mm, and its optical visible penetrating ability is 0.8–0.9 mm. 6 At the same time, it works in the continuous mode. Although the mechanical effect can be avoided, the tissue damage caused by the thermodynamic effect of the continuous working mode and the strong tissue penetration is worthy of attention. 27
Recently, the thulium laser has received a lot of attention. Its tissue-penetrating ability is just about 0.4 mm, and its wavelength is 2013 nm. According to the study's findings, the thulium laser looks to be the best laser for prostate enucleation because it has a low risk of complications and efficacy equivalent to other lasers. 6 The maximum amount of tissue damage brought on by mechanical impacts can also be minimized by the continuous working mode of thulium laser.
There are still many limitations in this study. First, the number of comparative studies between different lasers is inconsistent. Holmium laser and thulium laser are currently the most widely used laser types. Among the nine studies included in this study, five discuss the comparison between them. Too little original data for green and diode lasers may affect the results. Second, because there were no randomized controlled clinical studies with other lasers, the eraser laser, a type of laser already used in prostate enucleation, was excluded from the analysis of this NMA.
Conclusion
According to this NMA, greenlight laser may be more complication risk when applied in the prostate enucleation than the other three lasers. Thulium laser may be the recommended laser system since it can bring less complication risk with comparable efficacy. More RCTs are still needed to validate this study.
Footnotes
Authors' Contributions
Conception and design: T.J. Administrative support: T.J. Provision of study materials or patients: Y.M., L.L. Collection and assembly of data: Y.M., L.L. Data analysis and interpretation: Y.M., L.L., Z.L. Article writing: all authors. Final approval of article: all authors.
Ethics Approval
This is a NMA, which did not require an informed consent.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.