
Abstract
Background:
Endoscopic enucleation of the prostate (EEP) is a safe and effective intervention option for management of variable-sized adenomas.
Purpose:
The aim of this study was to point out the safety and efficacy of bipolar needlescopic enucleation of the prostate (BNEP) in comparison with bipolar vapoenucleation of the prostate (BVEP).
Materials and Methods:
This is a prospective randomized trial. In all, 214 patients with variable size adenoma were randomly assigned (1:1) to either the BNEP group (108 patients who underwent bipolar endoscopic enucleation of the prostate [BEEP] using a needle electrode) or the vapoenucleation (BVEP) group (106 patients who underwent BEEP using vaporization electrodes). Intra- and intergroup objective and subjective outcomes were compared at different time points for 1 year. In addition, all other procedure-related events and mishaps were registered and compared.
Results:
The medians (interquartile ranges) for operative time (OT), resected tissue weight, postoperative irrigation time, and hemoglobin drop were 60 (50–88) vs 80 (60–98) minutes, 67 (56–86) vs 46 (40–61) grams, 10 (8–12) vs 12 (10–18) hours, and 1 (0.6–1.3) vs 1.2 (0.88–1.9) g/dL for BNEP and BVEP groups, respectively (p < 0.05). Both subjective and objective parameters were analogously improved in the two groups (p > 0.5). However, the postoperative irritative symptoms and urinary infections were lower in the BNEP group (p < 0.05).
Conclusions:
Our results revealed that although both BNEP and BVEP are effective and safe in the management of benign prostatic obstruction, BNEP is superior in terms of less OT, intraoperative blood loss, irrigation time, irritative symptoms, and urinary infections.
Introduction
Lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH) are a common health problem in seniors, with a serious impact on their quality of life (QoL). 1 From its inception into practice, transurethral resection of the prostate (TURP) is considered a relatively minimally invasive gold standard intervention for management of BPH. Indeed, TURP is still recommended by the most popular guidelines as the first choice for management of small- to medium-sized glands requiring more than medical treatment. 2,3
TURP is a size-limited procedure and is associated with considerable morbidity. Therefore, for larger prostates, the enucleation procedure is the most viable option for management of this subset of BPH as it enables surgeons to remove as many prostatic tissues as possible with excellent durability. 4 The energy required for prostate enucleation may be from either mechanical sources (simple prostatectomy: open, laparoscopic, or robotic) or endoscopic nonmechanical sources such as different laser types or electrical energy (either monopolar or bipolar). 5
Originally, the concept of endoscopic enucleation of the prostate (EEP) using monopolar energy was introduced by Hiraoka. 6 Fifteen years later, holmium laser enucleation of the prostate (HoLEP) was described. 7 After another 8 years, bipolar endoscopic enucleation of the prostate (BEEP) was introduced as a fabulous alternative to HoLEP. 8
In the present study, we compared the safety and efficacy of bipolar needlescopic enucleation of the prostate (BNEP) with bipolar vapoenucleation of the prostate (BVEP) in patients with variable size adenomas.
Patients and Methods
Two hundred fourteen of 257 patients with LUTS due to BPH were finally included in the present study (Fig. 1). After obtaining institutional review board approval, all recruited patients in this trial were asked to sign a well-informed written consent according to the Declaration of Helsinki. This study was registered at

Flow diagram illustrating the study design. BNEP = bipolar needlescopic enucleation of the prostate; BVEP = bipolar vapoenucleation of the prostate. Color images are available online.
Inclusion criteria were patients with an enlarged prostate >70 g, maximum flow rate (Qmax) of ≤10 mL/s, and International Prostate Symptom Score (IPSS) >7. The exclusion criteria were patients with prostate and/or bladder cancer, bladder diverticulum, urethral stricture, active urinary tract infection (UTI) unless properly treated and the urine proved to be sterile, and a previous prostatic surgery; patients complaining of neurogenic voiding dysfunction; and cases with coagulopathy.
All patients underwent the following routine preoperative evaluations: urine analysis with culture and sensitivity (when indicated); renal function tests; hemoglobin (Hb) concentration, coagulation profile, serum electrolyte, blood sugar, and liver function tests; and serum prostate-specific antigen (PSA) test. Furthermore, abdominal and transrectal ultrasonography (TRUS) was performed for assessment of the upper tract, postvoiding residual urine (PVRU), and prostate size (PV). Besides, Qmax and body mass index (BMI) were determined.
Sample size and data manipulation
The sample size was calculated using G*Power software, version 3.1.9.2, based on a medium effect size of IPSS between the two study groups (d = 0.5), alpha and power levels were adjusted at 5% and 90%, respectively. The calculated minimum required sample size was 180 in all (90 cases per group). In an attempt to avoid type I errors and with a presumed dropout rate (20%), the total number of allocated patients was raised to 214 patients.
The study was conducted on 214 patients with BPH who were randomly allocated to one of the following procedures: Group 1: 108 patients underwent BEEP by needle (hot knife) electrode (needlescopic enucleation) (BNEP). Group 2: 106 patients underwent BEEP by vaporization (ball) electrode (vapoenucleation) (BVEP).
Randomization and patient assignment were computer generated (1:1). Both patient and parameter assessors (radiologist and outcome assessor) were blinded to patient allocation. Provided that the patient was followed up at least once postoperatively, the missing data were imputed by the last observation carried forward method. However, for adverse events (AEs), no imputation for missing data was used.
Statistical analyses were conducted using SPSS, version 26 (IBM, Armonk, NY). Continuous data are presented by the median and interquartile range (IQR). For assessment of functional outcomes at baseline, 3 months, 6 months, and 1 year, the Bonferroni-adjusted Kruskal–Wallis or analysis of variance test was used as appropriate. All pairwise intergroup comparisons were performed by either Mann–Whitney U or Student's t-tests, while pre- vs postoperative outcomes were compared in each group (intragroup) using the Wilcoxon signed-rank test or paired t-test, as appropriate.
Categorical data are shown as numbers and/or percentages and were analyzed using Fisher's exact or χ 2 tests when appropriate. Statistical significance was considered when p < 0.05.
Surgical procedures
All patients underwent transurethral enucleation of the prostate using bipolar plasma kinetic energy, utilizing either a needle or vaporization electrode. All procedures were performed by one single expert surgeon (W.E.) who performed more than 250 BEEP procedures. The technique required a high-frequency bipolar generator with an external resection module, namely VIO® 300 D (ERBE Elektromedizin GmbH, Tubingen, Germany).
As per manufacturer recommendation, the power output setting was 5 and 6 for cutting and coagulation modes, respectively. A rotating 26F continuous-flow resectoscope with an active bipolar working element (Karl Storz, Tuttlingen, Germany) was used. The three-lobe technique was utilized, and resultant chips (resected by the cutting electrode) were retrieved and washed out by Ellick's evacuator and then a 22F three-way urethral catheter was inserted. The enucleoresection technique was previously described 9,10 and is illustrated in Figures 2, 3, and 4. All the retrieved chips were weighted and sent for meticulous histopathological examination.
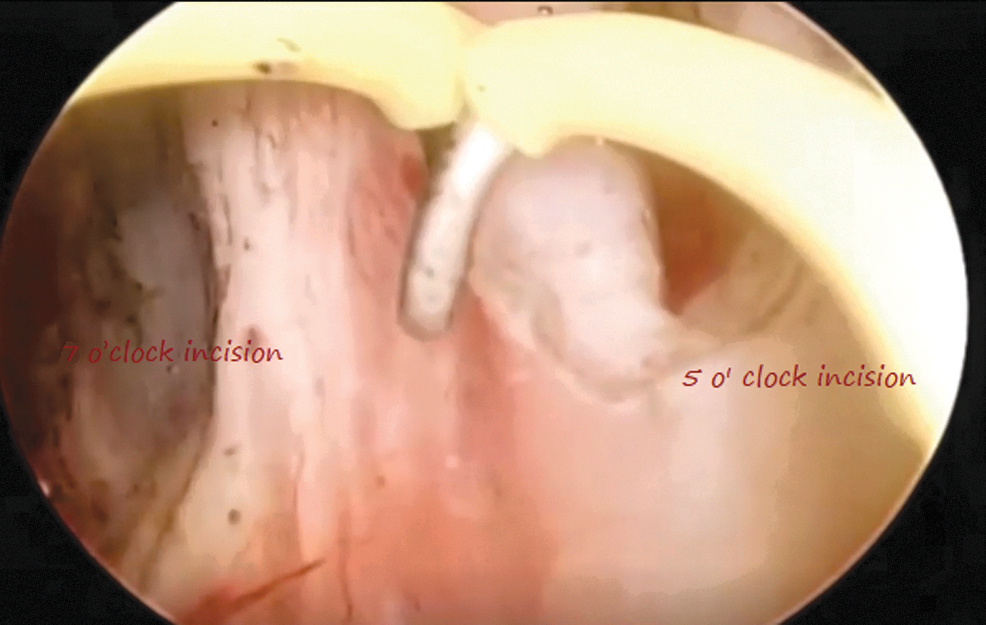
Five- and 7-o'clock incisions. Color images are available online.
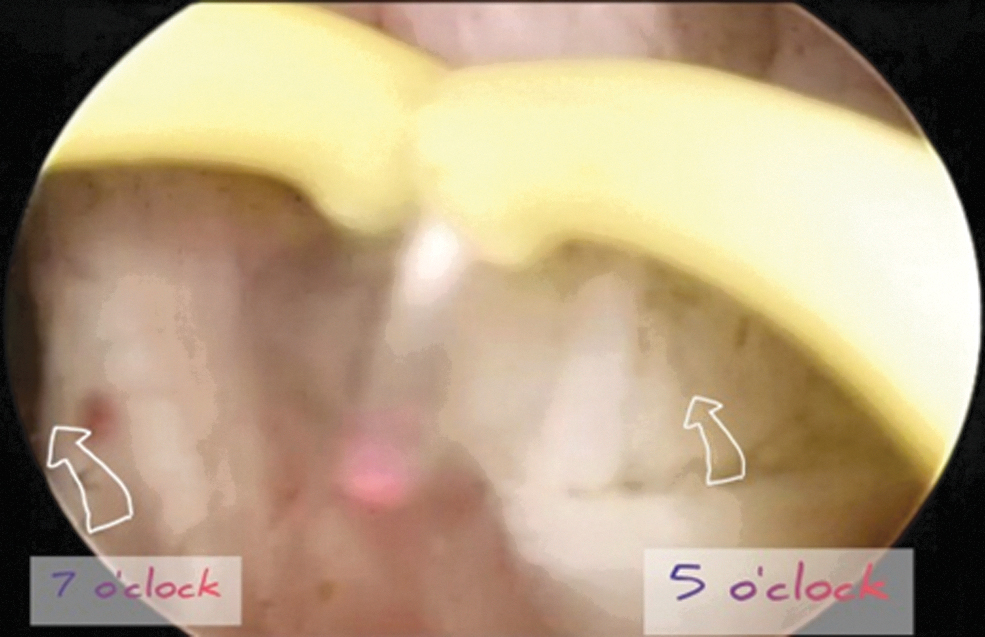
A transverse incision between the 5- and 7-o'clock incisions while the electrode is active. Color images are available online.

An enucleated lobe attached by a pedicle during its resection. Color images are available online.
Perioperative evaluation
The perioperative parameters, including operative time (OT), [which was calculated from insertion of the resectoscope (start of enucleation) to insertion of a urethral catheter], intraoperative mishaps, retrieved tissue weight, postoperative bladder washout, duration of postoperative catheterization, Hb deficit, length of hospital stay, and trial without catheter (TWOC), were recorded. In addition, perioperative AEs such as pyrexia, blood transfusion rate, clot retention episodes, and/or mortality rates were recorded.
Follow-up
The primary endpoint of the present study was improvement of IPSS, while secondary outcomes were other parameters, including short- and long-term complications. To do so, all patients' parameters were recorded and followed up at baseline and 3, 6, and 12 months postoperatively. At each visit, IPSS, QoL, Qmax, PVRU, PV, PSA, and any AEs were assessed.
Results
As indicated in Table 1, the preoperative patients' demographic criteria, including age, BMI, comorbidities, PV, Hb, serum electrolyte levels, IPSS, Qmax, QoL, PVRU, and PSA, were similar in both groups (p > 0.05).
Patients' Preoperative Demographic Criteria for Both Groups
BMI = body mass index; BNEP = bipolar needlescopic enucleation of the prostate; BVEP = bipolar vapoenucleation of the prostate; DM = diabetes mellitus; Hb = hemoglobin; HTN = hypertension; IPSS = International Prostate Symptom Score; IQR = interquartile range; PSA = prostate-specific antigen; PV = prostate size; PVRU = postvoiding residual urine; Qmax = maximum flow rate; QoL = quality of life.
Our operative data revealed that the medians (IQRs) for OT; retrieved prostatic tissue weight; postoperative irrigation time; and Hb drop were 60 (50.0–87.5) vs 80 (60–97.5) minutes; 66 (55–86) vs 45 (40–60) grams; 10 (8–12) vs 12 (10–18) hours; and 1 (0.6–1.3) vs 1.2 (0.88–1.9) g/dL for BNEP and BVEP groups, respectively (p < 0.05). On the other hand, there were no significant differences between both groups in terms of postoperative creatinine and serum electrolyte levels, catheter duration, and length of hospital stay (p > 0.05) (Table 2).
Differences Between Groups According to Perioperative Events
Significant p < 0.05.
OT = operative time.
Overall, at the different postoperative follow-up visits, both subjective and objective parameters, that is, IPSS, QoL, PV, PVRU, Qmax, and PSA levels, were robustly improved in the two groups compared with their corresponding baseline values (p < 0.05) (Table 3).
Differences Between Groups According to Functional Outcomes
Pc: Bonferroni-corrected p-value, including corresponding baseline values.
Significant p < 0.05.
N/A = not applicable.
The postoperative AEs are listed in Table 4. The reported LUTS and UTIs were lower in the BNEP group than the BVEP group (p < 0.05). Otherwise, there were no statistically significant differences in other reported AEs between the two groups (p > 0.05). Interestingly, one patient of the two in the BNEP group who experienced urinary retention after the first TWOC was managed by urinary catheter insertion.
Long- and Short-Term Complications Classified According to the Modified Clavien System (M.C.)
Significant p < 0.05.
LUTS = lower urinary tract symptoms; M.C. = Modified Clavien; UTI = urinary tract infection.
Yet, the patient experienced recurrent attacks of urinary retention when attempting TWOC due to obstruction of the catheter, and many trials were performed for manual irrigation to wash out the bladder. Last, pelvic ultrasound (US) indicated that there was a missed detached lobe that was engaged into a hole of the catheter. Therefore, under Ultrasound guidance, while a negative pressure was applied (suction of the catheter using a 50-mL syringe), the catheter was removed with the missed lobe (Fig. 5).
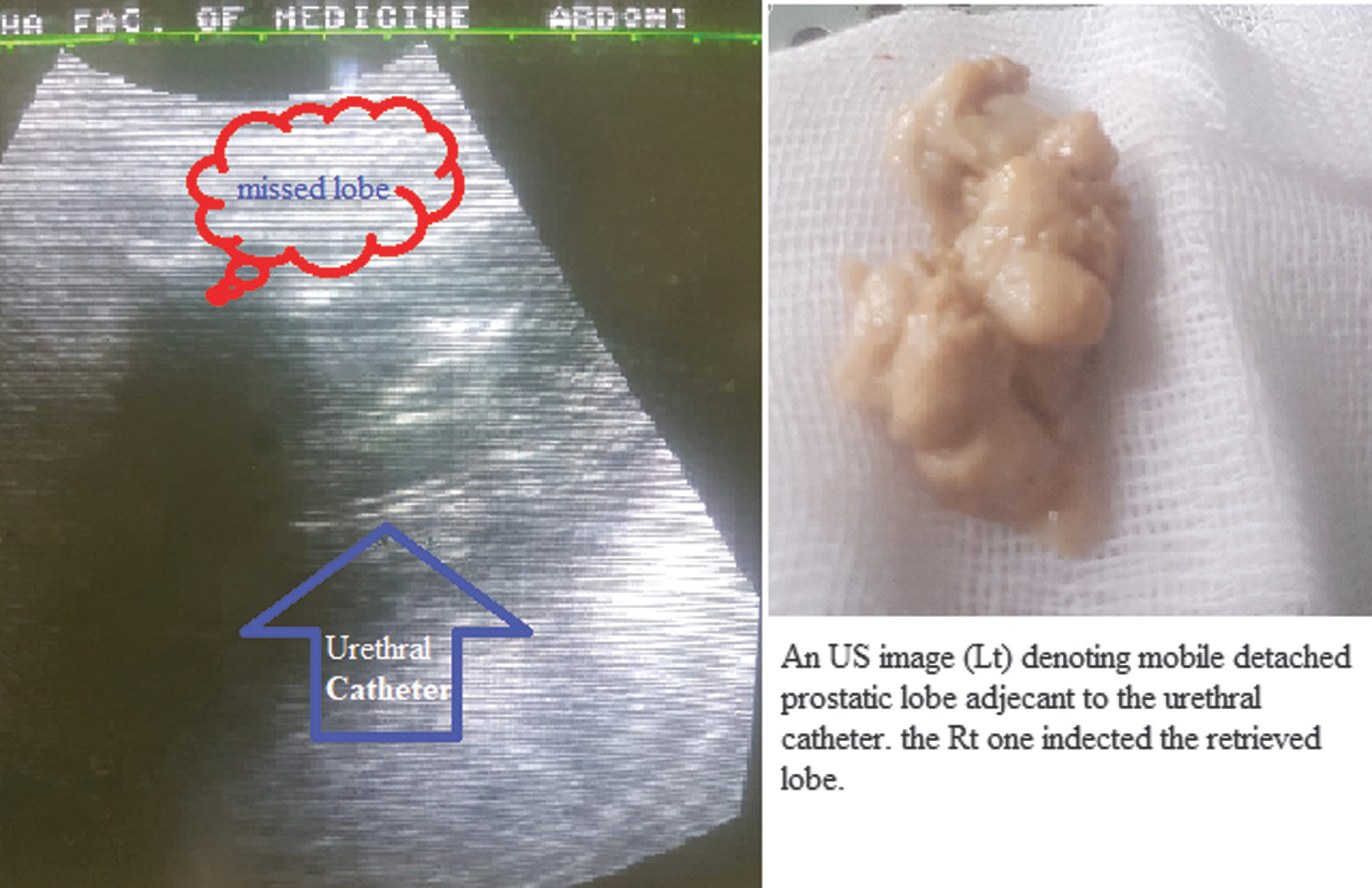
Illustration of the retrieval maneuver of the missed lobe. US, ultrasound. Color images are available online.
Discussion
BEEP is one of the front-runners, a size-independent option, for management of BPH with a considerable safety profile and excellent functional outcomes. 11 BEEP is an efficient and safe procedure such as HoLEP with shorter operative, catheterization, and hospitalization times. Both functional outcomes and complications are similar in both procedures for at least 1 year postoperatively. 12 In addition, BEEP costs less than HoLEP as the generators are readily available in most hospitals. Besides, unlike in the commonly reported classical HoLEP procedure, which is sophisticated and relatively expensive, the morcellator is not a necessary device in the BEEP armamentarium. 13 –15
Not surprisingly, compared with open prostatectomy (OP), BEEP has similar functional outcomes and comparable amounts of retrieved tissues with the advantages of lesser invasiveness, shorter hospitalization, and fewer AEs. 16
In the present study, the median OT was shorter in the BNEP group than the BVEP group (65 vs 80 minutes, p = 0.009). This finding can be explained in light of the fact that using needle electrodes in BNEP enables rapid and precise hemostasis during the procedure, which ultimately saves time. This plausible explanation is supported by another finding in our study; blood loss, indicated by Hb drop, was much lower in the BNEP group than the BVEP group (p = 0.005).
In the same line, bladder irrigation time until clear washout was shorter in the BNEP group than the BVEP group (p < 0.001). The clarity of the visual field and decreased blood loss during TURP have a considerable positive effect on OT and postoperative irrigant fluid volume. 17,18 A recently published study conducted by Patard and colleagues stated that BEEP had a shorter OT, catheterization time, and hospitalization than HoLEP. 12
Regarding the weight of resected tissue, our results revealed that there was a statistically significant difference in retrieved specimen weight in favor of BNEP (p < 0.001). Nonetheless, this finding is not necessarily indicative of more efficacy of BNEP than BVEP since the TRUS-measured PV was similar in both groups (p > 0.05) during different postoperative follow-up visits.
In fact, the difference in resected tissue weights between the two groups can be explained by the large concave surface area of the ball electrode in the BVEP group, which leads to vaporization and loss of some prostatic tissue, unlike in the BNEP group in which the enucleation with minimal vaporization technique was adopted, which led to more tissue retrieval (less tissue loss). The enucleation efficiency ratio in the present study ranged from 57% to 71%. This is similar to previously published results for BEEP, HoLEP, and OP. 4,11,12,14,16,19 However, in a contemporary systemic review, it was stated that BEEP has superior efficiency compared with TURP. 20
The key parameters of functional outcomes such as Qmax, IPSS, QoL, and PVR, as well as PSA, were evenly and robustly improved in both study arms when comparing baseline values with their counterparts in different postoperative follow-ups for 12 months. This is in line with the previously published data for different enucleation techniques. 12,14,16,19,21 Some other studies indicated that the technique is durable based on long-term follow-up. 4,9,20
In this study, the nadir level of PSA was 1.9 (1.5–2.5) vs 2 (1.6–2.93) and PSA density was 0.067 (0.05–0.096) and 0.072 (0.05–0.093) ng/mL 2 (p = 0.167) for BNEP and BVEP groups, respectively, at first postoperative evaluation. This level remained relatively consistent across subsequent follow-up visits. In a recently published literature review, the authors concluded that there is indirect evidence that nadir PSA is an indicator of surgical success and possible prostate cancer (PCa) and this level varies from 0.5 ± 0.4 to 1.9 ± 2.1 ng/mL at 3–6 months post-EEP. 22
Conversely, Martos and colleagues reported that nadir PSA is an independent factor in the diagnosis of PCa postoperatively. 23 A previously published study recommended that nadir PSA <1 ng/mL 2 and PSA density below 0.1 ng/mL 2 eliminate the possibility of postoperative PCa. 24
Overall, AEs were similar in both study groups. However, early postoperative irritative symptoms were more in patients of the BVEP group than in the BNEP group (p = 0.021). In our opinion, this difference may be attributed to the larger concave surface of the vaporization electrode used in BVEP, which led to more tissue denaturation and charring during its activation. On the other hand, the small, pointed hot knife (needle electrode) of BNEP resulted in less charring and/or necrotic tissue formation.
Not surprisingly, the documented postoperative UTI rate was higher in the BVEP group than in the BNEP group (p = 0.035). The previously reported rates of LUTS and UTI with different prostatectomy procedures vary between 3.6% to 34% and 3.8% to 34%. 25 –31 This discrepancy was imputed to several factors such as the baseline PV, the applied energy for prostatectomy (BEEP, laser, OP, and TURP, etc.), and the utilized technique such as excessive activation of the electrode or blunt enucleation with minimal ignition during the procedure.
From the aforementioned findings of this study, both BNEP and BVEP are suitable options for interventional management of BPH. Both techniques proved to be safe and effective with minimal AEs and functional outcomes analogous to other options such as traditional OP and the more modern game changers, that is, laser prostatectomy, especially HoLEP.
There are several advantages of BEEP over OP and HoLEP; first, it is a minimally invasive option with shorter hospitalization than OP, and second, the capital and maintenance costs are much lower compared with HoLEP. Furthermore, bipolar loops (ball and needle electrodes) are reusable and cost lower than laser fibers. 32 –34
There are several strengths of this study, including the prospective and randomized study design, besides the reasonable postoperative follow-up period (12 months). However, there are some limitations to the current study. For instance, our findings need to be confirmed in further multicentric and more extensive comparative studies that include different cohorts of patients such as subjects with bleeding disorders and/or on anticoagulants.
Conclusions
The results of this study revealed that although both BNEP and BVEP are effective and safe options for management of benign prostatic obstruction, BNEP is superior to BVEP in terms of less OT as well as less intraoperative blood loss and irrigation time and fewer irritative symptoms and urinary infections. Both options are cost-effective, minimally invasive endoscopic options with outcomes similar to other endoscopic options such as HoLEP.
Footnotes
Authors' Contributions
All authors included in this article submission are responsible for (1) substantial contributions to the conception or design of the work or acquisition, analysis, or interpretation of data for the work; (2) drafting the work or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Informed Consent
Informed written consent has been obtained.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
No funding was received for this article.