
Abstract
Purpose:
To evaluate the clearance of metal particles produced and released in the pelvicaliceal system (PCS) during percutaneous nephrolithotomy (PCNL) with the use of the Swiss Lithoclast® Trilogy dual-energy (EMS Urology, Nyon, Switzerland) lithotripter.
Methods:
An experimental in vivo study and a clinical investigation of case series were conducted. An in vivo porcine model with two pigs for lithotripsy (after inserting artificial stones into the collecting system) and two pigs for submucosal injection of metal particles (provided by the manufacturer of Trilogy) was conducted. Porcine kidney histology analysis for metal leftovers was conducted immediately or 2 weeks after the surgery. A prospective observational study design included 10 consecutive patients treated with conventional 30F PCNL or with 22F mini-PCNL technique. Only the patients with the confirmed metal particles in the PCS during the initial PCNL and the need for additional retrograde intrarenal surgery over a period of 2–4 weeks were selected. The presence of metal particles was evaluated during the second endoscopic surgery.
Results:
The generated metal particles during PCNL and the submucosally injected particles were not found macroscopically 2 weeks postoperatively in porcine models. No pathologic changes such as foreign body granuloma or inflammation were found. Similarly, no metal particles were observed during the second look endoscopy (n = 10).
Conclusion:
Metal particles observed endoscopically using the Trilogy lithotripter are cleared with no pathologic evidence of tissue damage from the metal particles 2 weeks after the procedure. Thus, the intraoperative release of any particle by the Trilogy lithotripter should not raise any safety concerns.
Introduction
Percutaneous nephrolithotomy (PCNL) is the treatment of choice for renal stones ≥2 cm. A variety of lithotripters with improved efficacy and safety along with faster stone clearance and lower complication rates is currently available in the technologic armamentarium of urologists. 1,2
Pneumatic and ultrasonic lithotripters are the devices of choice by many urologists who perform PCNL as they are associated with high efficiency. The Swiss Lithoclast® Trilogy dual-energy (EMS Urology, Nyon, Switzerland) offers the possibility of combining ballistic impact, ultrasound waves, and suction simultaneously on the same device. 3 The lithotripsy is achieved by different sizes of metal probes inserted through the working channel of the metal nephroscope. 4 As such, the use of these devices can be associated with the generation of metal particles, a known issue in the urologic community. 5 In our clinical practice, we have observed generation of metal particles with both small (3.4F) and big (3.9F) lithotripter probes.
Currently, the literature lacks studies investigating the safety profile of those particles on the tissue. One of few studies published by Marberger and colleagues in 1985 evaluated patients' safety in cases where the metal particles were visible. 6 In their study, a leporine bladder was used with rubbing of particles into the bladder mucosa wherein besides inflammation no significant damage was observed. That setting, though, is not an adequate simulation model for a PCNL scenario, wherein instead of the bladder the target anatomical structure is the kidney.
Considering the high-energy potential of dual-energy lithotripters and, in general, the fragility of kidney parenchyma, it is of paramount importance to critically analyze the safety profile of those instruments. Therefore, the aim of our study was to evaluate the clearance of metal particles produced and released in the pelvicaliceal system (PCS) during the PCNL procedure with the use of the Swiss Lithoclast Trilogy dual-energy lithotripter in in vivo experimental and clinical observational study designs.
Materials and Methods
Study design
For this study, we utilized two different design settings. An experimental in vivo porcine model, being closest to the human kidney as an experimental model, was used to assess the clearance and the potential damage of the metal particles on kidney tissue investigated by the histopathologic evaluation of the kidneys immediately and after 2 weeks.
A prospective study design including 10 consecutive patients treated with conventional 30F PCNL or with 22F mini-PCNL technique was then utilized to further investigate the clearance of generated metal particles and the findings of an experimental study in the clinical practice.
Experimental in vivo porcine model
Ethical approval of the in vivo experimental and clinical studies was obtained before the initiation of the experiment (No.: 20/24.06.2020 PGNP). In total four female pigs weighing >30 kg were included. Ketamine (5 mg/kg), xylazine (1 mg/kg), and atropine sulfate were injected for initiation of anesthesia. The maintenance of anesthesia was achieved using intravenous injection of propofol 5% throughout the whole procedure. For rigorous evaluation, the in vivo experiment was conducted in two distinct parts.
The initial procedure included the establishment of a percutaneous tract in one of the kidneys while leaving the other kidney intact. Specifically, a cystoscopy was performed with the animal in the supine position, and a 0.035 sensor guidewire (HiWire™ COOK Medical; Cook Ireland Ltd., Limerick, Ireland) was advanced in one of the kidneys followed by the insertion of a ureteral catheter in the renal pelvis. The animal was then repositioned to prone. Using a fully fluoroscopic guided biplanar puncture technique (Bull's eye), percutaneous access was achieved with an 18-gauge needle. A 24F PCNL tract was created using two-step dilatation with 16F and 24F dilators.
For the performance of the first part of the experiment, artificially made stones (Begostone Plus; powder-to-water ratio 15:3) were inserted through the lumen of the 24F sheath. Stone disintegration in the selected kidney of each pig was performed using the Trilogy lithotripter. The presence of metal particles after the lithotripsy on the urothelium was confirmed endoscopically (Fig. 1).

Metal particles attached to the mucosa of the pig renal pelvis after lithotripsy. Color images are available online.
For the second part of the in vivo experiment, no lithotripsy was performed. Instead, after establishing 24F PCNL access, the metal particles were injected submucosally in the pelvis of the porcine kidney under endoscopic vision using a long percutaneous needle (Echotip®, disposable two-part trocar needle, COOK Medical, Cook Ireland Ltd., Limerick, Ireland) inserted through the lumen of the nephroscope. We injected ∼0.5 cm3 of metal particles diluted in 0.5 mL saline. The particles were injected submucosally into the pelvis in the anterior and posterior parts. The amount injected was ∼10 times more than the usual amount seen during lithotripsy.
Of note, during lithotripsy, metal particles can go submucosally when there is a submucosal tear. Usually the metal particles are seen on the mucosa. The metal particles were obtained by the manufacturer (EMS Urology, Nyon, Switzerland) and were made of the same material as the single-use probes of the lithotripter. For each experimental part, two pigs were considered. Two pigs, one from each experiment, were sacrificed immediately, whereas the other two pigs were left alive and sacrificed 2 weeks after the procedure. In every case the experiment was performed only in one kidney, leaving the other intact.
The clearance of the intraoperatively generated or submucosally injected metal particles or any other histologic alternation (i.e., inflammation) was evaluated with the histopathologic examination of the PCS of the kidneys. Both the treated and the control kidneys of each pig were evaluated by a blinded pathologist.
Clinical study design
Prospective data of 10 consecutive patients treated either with conventional PCNL (30F) or mini-PCNL (22F) were collected. Informed written consent was obtained from each patient included in the study. The applied inclusion criteria were the performance of a PCNL using either conventional or mini-PCNL, presence of metal particles during the initial PCNL procedure, and patients requiring retrograde intrarenal surgery (RIRS) after the initial PCNL.
Patients were subjected to fluoroscopic guided prone PCNL. The dilatation was performed using Amplatz dilators. According to the usual practice of our department, an access size of 30F or 22F was performed accommodating a 26F or 18F nephroscope, respectively. The Trilogy lithotripter was used for lithotripsy with maximal settings (100% ballistic [shockwave], 100% suction, 100% ultrasound, and 12 Hz frequency). Depending on PCNL tract size, two different Trilogy probes with an external diameter of 3.9 or 3.4 mm and the length 440 and 445 mm were used. At the end of the procedure, a 24F malecot tail stent or 14F nephrostomy tube was placed in each kidney to ensure postoperative drainage. All cases were operated by two highly experienced endourologists.
Patients' follow-up and variables of interest
The postoperative follow-up of the patients was performed on the second postoperative day and at 1-month after the initial PCNL using kidney, ureter, bladder radiography, and ultrasonography or noncontrast enhanced CT. The patients with residual stones (stone size >4 mm) requiring auxiliary treatment for residual stones (RIRS) within 2–4 weeks after the initial PCNL were considered as potential candidates for the involvement in this study. As such, the clearance of metal particles was evaluated on patients requiring auxiliary treatment to avoid performing additional procedures to those patients who did not require any additional treatment.
The main variable was the presence or absence of any metal particles in the collecting system or visible metal particles in or under the mucosa. Basic demographic characteristics were collected. Data regarding stone characteristics as well as treatment efficiency including the stone-free rate and the auxiliary treatment were not the aim of the current studies and were not collected. Simple descriptive statistics were performed using IBM SPSS version 20 statistical software (IBM Corp., Armonk, NY, USA).
Results
Experimental study
In total, four porcine renal units were considered for our study. Immediate histopathologic examinations were performed in two pigs, whereas the remaining two pigs were investigated 2 weeks after the PCNL procedure.
Pathologic analysis of porcine kidneys performed immediately and 2 weeks after the surgery revealed the absence of metal particles embedded in the PCS (Fig. 2). Pronounced inflammation and fibrosis were observed in the regions surrounding the PCNL tract at pathology analysis at 2 weeks. For the second part of the experiment wherein metal particles were injected submucosally, the pathologic macroscopic investigation revealed the site of metal particle injection into the renal pelvis.
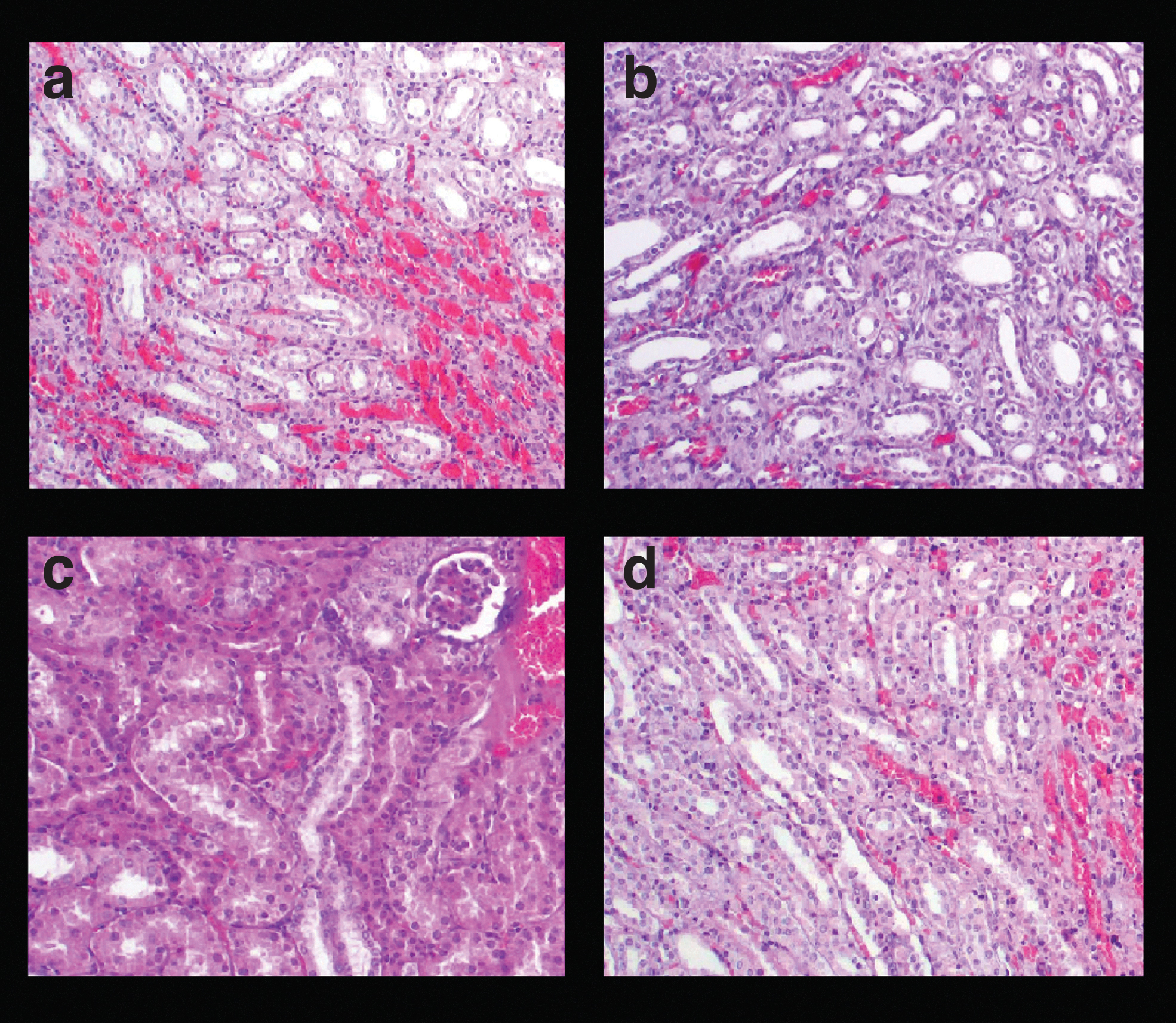
Histologic images after experimental porcine PCNL surgery. Hematoxylin and eosin stained section showing renal parenchyma without any amorphous material ( × 100)
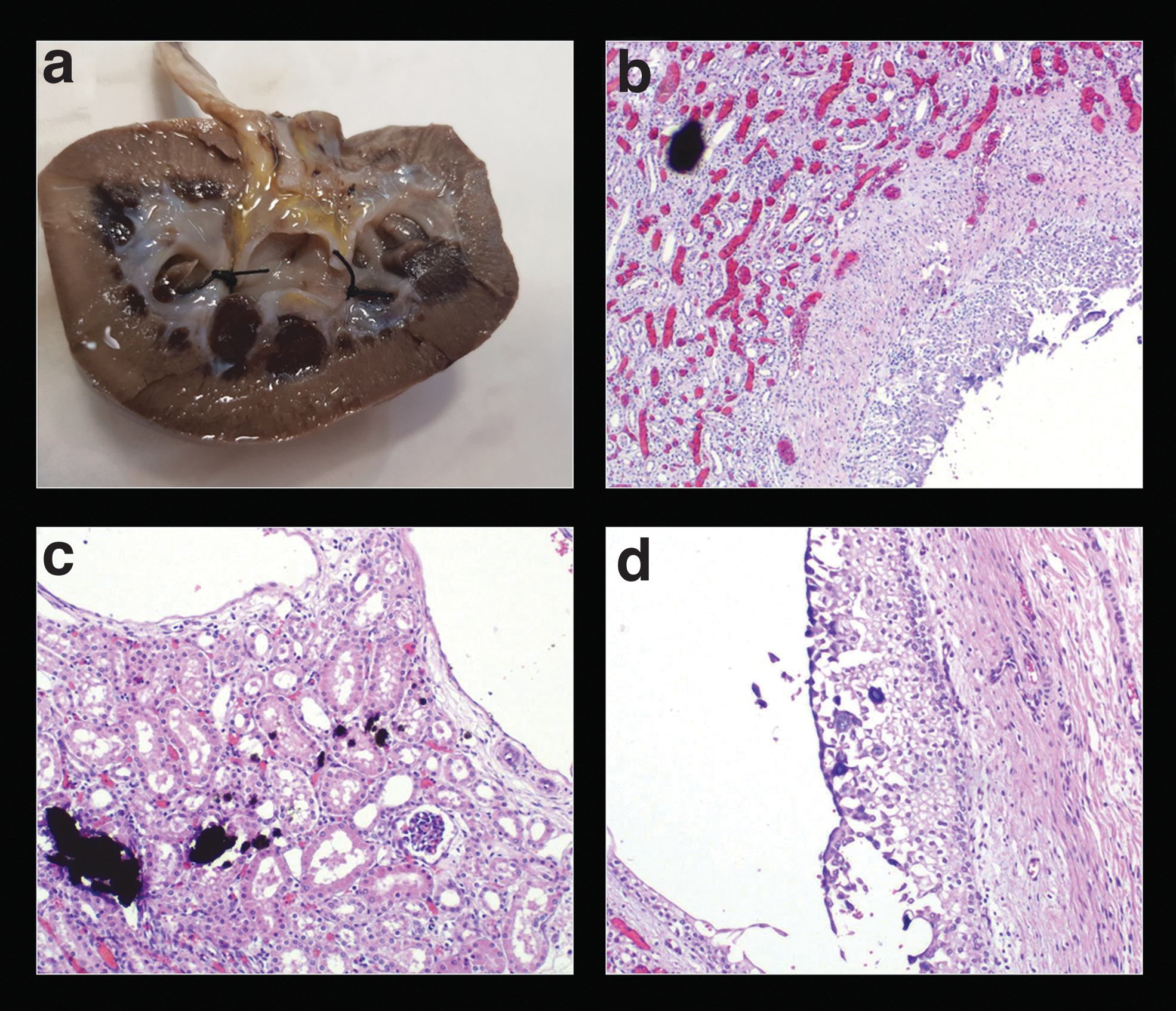
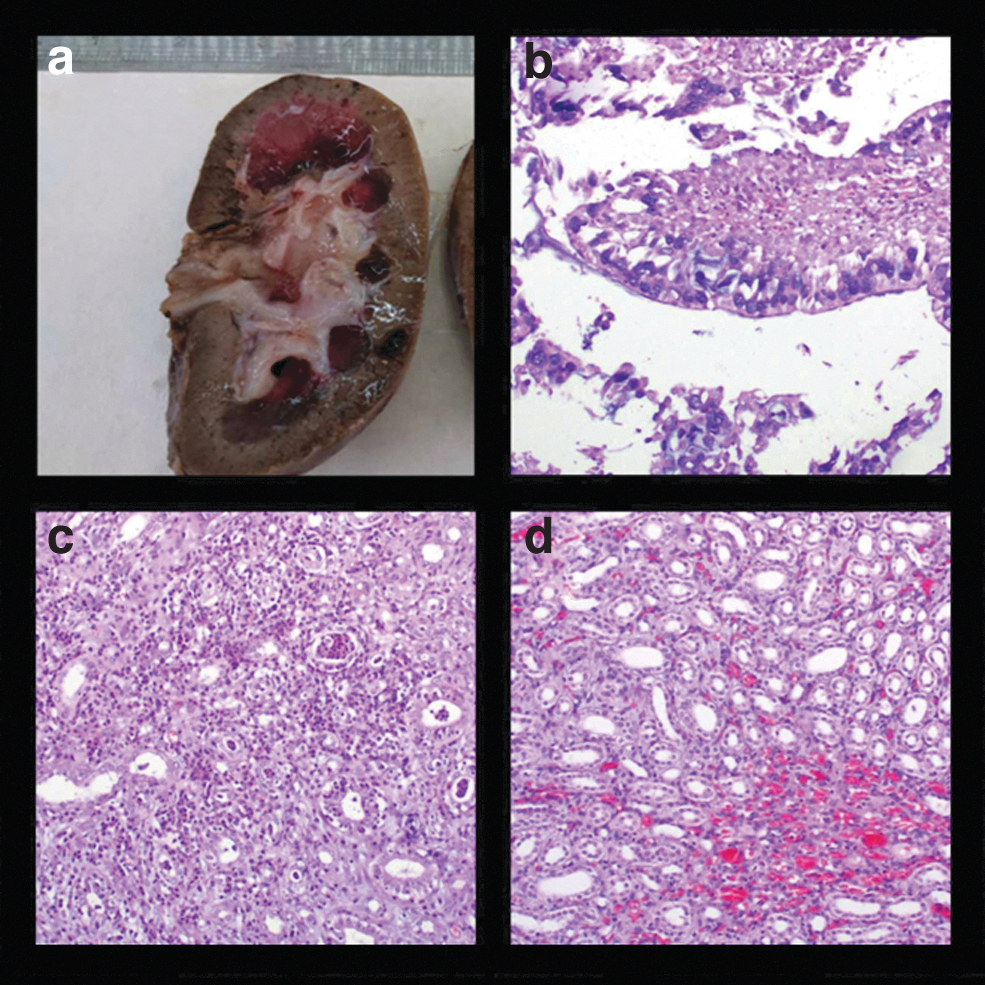
Hematoxylin and eosin staining showed a black amorphous material entrapped into the renal medulla adjacent to a renal calix within the urothelium (Fig. 3). The pathologic evaluation after 2 weeks found no metal inclusions in the submucosa of the injected kidney (Fig. 4). In addition, moderate to pronounced inflammation and fibrosis in the peri-PCNL tract were reported in the treated kidneys compared with the control groups. No other adverse reactions such as foreign body granuloma and other tissue changes were observed by metal particles.
Clinical cases
A total of 10 cases (6 men and 4 women) were included in this study. The median age and BMI were 53.5 years (interquartile range [IQR] = 46.5–68.5) and 24.1 kg/m2 (IQR = 22.5–28.5). In all 10 cases, the presence of metal particles was proved endoscopically at the time of the initial PCNL (Fig. 1). All these cases were subsequently treated with RIRS to achieve stone-free status. The initial procedure was standard PCNL with 30F access in three patients and mini-PCNL with 22F access sheath in seven patients. No complications were related to PCNL and RIRS cases. In all patients, the metal particles were not visible in the PCS during the second RIRS procedure.
Discussion
The advancements in technology such as the dual-energy lithotripters have changed dramatically the operative approach to combat urolithiasis with a large stone burden. 7 The trilogy lithotripter, using the trimodality of ultrasonic and electromagnetic energy and an efficient suction system, is an excellent tool for the lithotripsy surgical armamentarium. 8 The technology is highly efficient and can potentially destroy all varieties of stone composition. 9 Desai et al have shown that the use of Lithoclast Trilogy resulted in effective stone clearance during both standard and mini-PCNL procedures. 10
One of the concerns when using the Lithoclast Trilogy lithotripter is the generation of metal particles after the PCNL procedure, either from the direct ballistic effect of the lithotripter on the stone or from metal to metal impact. These particles seem to be flushed out by continuous irrigation during surgery, though the exact amount of material left behind and its effect on the tissue have never been investigated.
In this study, we evaluated the potential kidney damage and metal particle deposition after PCNL using a dual-energy Lithoclast Trilogy lithotripter. With the experimental porcine model and clinical observation, clinical and pathologic concerns regarding metal particles were resolved. We found that the generated metal particles are flushed out immediately after the PCNL, leaving the urothelium without any visible particles. The pathologic evaluation at 2 weeks showed no sign of inflammation and granuloma formation in the treated kidneys, even when the metal particles were injected submucosally. Clinical observation also showed evacuation of the metal particles at 2–4 weeks post-PCNL.
Dual-energy lithotripters have the advantage of combining two energy sources (ultrasonic and pneumatic probes) in a single instrument. 11 The latest devices (the Lithoclast Trilogy and the ShockPulse-SE [Olympus, Tokyo, Japan]) work with a double system in one probe. 11 These lithotripters quickly and effectively disintegrate stones as shown in experimental and clinical studies. 4,12 –14
The effect of energy sources on the pathohistologic changes of the mucosa was evaluated by Khoder and colleagues. 15 They conducted a comparative in vivo study to investigate the effects of dual-energy vs single-energy ultrasound lithotripters. The authors used porcine bladders for their experiment. The pigs were euthanized 1 week after the procedure. No systemic signs of inflammation were observed, independently of the lithotripter used. The histologic reports showed ongoing healing of the bladder mucosa. There were no significant differences in histologic findings taking changes of the epithelium, the leukocyte infiltration, the vascular congestion, and edema between the single- and the dual-mode groups. The mentioned findings are in keeping the results of this study.
The main difference is that in our study, the tissue examined was the PCS, which is also the point of interest for PCNL surgery. In addition, artificial stones were used in this experiment to fully mimic the real-life conditions of the procedure. The metal particles were also injected submucosally to ensure their presence in the renal pelvis at the end of the surgery. The particles were taken from the metal probe of the EMS lithotripter.
The first study evaluating the effect of metal particles generated during the ultrasonic lithotripsy was conducted in 1985 by Marberger et al using rabbit bladders. 6 The investigators used an ultrasound lithotripter. They found that the metal particles were present macroscopically after 9 weeks, although the histologic results revealed no indications of inflammatory reaction. Our experiment was conducted in real-life conditions. The tools used were the same that is used for a real PCNL case.
The histologic reports at 2 weeks after the procedure (injection or PCNL) proved that there were no metal particles or signs of inflammation in the renal pelvis. We tend to believe that this happened because of the continuous irrigation and urine flow in the PCS, in contrast to the remaining urine in the bladder, which is more a reservoir than a constantly urine-producing environment.
To our knowledge, this is the first study to evaluate metal particle clearance after PCNL. An advantage of this study was the thorough evaluation of the effect of metal particles in both animal and clinical settings. Performing a clinical observational study, we evaluated the trends of our experimental setting in a clinical scenario.
Our study was not free of limitations. A pathologic investigation could not have been taken in patients for medical and patient safety reasons. This limitation was resolved by examining the pathology samples of the sacrificed pigs, the latter resembling the human anatomy best. Supposing that there are not many centers globally that have the opportunity to conduct such experimental evaluation, we consider this study a unique chance to investigate the safety and efficacy of this technology.
Another criticism may be the small number of patients enrolled in this study. Best clinical practice and standard of care were applied to our patients. As such, only patients who needed a complementary RIRS, that is, residual stone burden, were enrolled. Even with relatively small sample size, we believe we were able to show the trends of the treatment outcomes and the safety of the technology.
Conclusion
The Lithoclast Trilogy lithotripter is an important surgical tool in PCNL. After initial concerns about the safety caused by visible metal particles in the renal pelvis, this study could show that the Trilogy lithotripter did not leave any metal particles after a follow-up of 2 weeks on pathology analysis. No adverse pathologic findings including inflammation and granulomas were observed in the experimental setting. The clinical case series proved that the generated metal particles left the PCS within 2–4 weeks postoperatively, suggesting no adverse events in humans.
Footnotes
Authors' Contributions
A.N. contributed to project development and conception data analysis, data collection and data analyses, performance of the experiment, and article drafting; A.T. was involved in data collection and data analysis, performance of the experiment, and article drafting; A.P., C.A., K.P., V.B., D.K., and T.V. contributed to data collection and critical revision; G.K., K.G., and E.L. carried out project development and critical revision; and P.K. was in charge of project development and conception, interpretation of data, and critical revision.
Acknowledgment
The authors thank EMSUrology (Switzlerand) for providing metal particles.
Ethical Standards
The study was carried out in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The experiments were carefully designed and preapproved by the Veterinary Administration of the Prefecture of Western Greece and conducted according to Directive 2010/63/EU (
Disclaimer
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.