
Abstract
Introduction:
Transurethral resection of bladder tumor (TURBT) remains the gold standard method of diagnosing and treating nonmuscle invasive bladder cancer. Laser resection has been demonstrated as a safe and efficacious alternative; however, its mainstream use remains limited. The aim of this review is to comparatively evaluate clinical outcomes of TURBT and laser resection of bladder tumor (LRBT) for bladder cancer.
Methods:
A systematic review of the literature was performed for studies comparing TURBT and LRBT for bladder cancer. Outcome measurements were recurrence rates, complication rates, patient demographics, operative duration, and inpatient stay. Meta-analysis was performed using Review Manager 5.
Results:
Twenty studies on 2621 patients (n = 1364 for TURBT and n = 1257 for LRBT) met inclusion criteria. Demographics, including age and gender ratio and follow-up period, were similar in both groups. Recurrence rates were similar between TURBT and LRBT (29.1% vs 28.2%, p = 0.12). TURBT had a significantly greater obturator kick rate (11.5% vs 0.4%, p < 0.0001) and perforation rate (3.7% vs 0.009%, p = < 0.0001). In the six studies which reported on presence of detrusor muscle in the specimen, it was significantly greater in the LRBT group (96.6% vs 88.1%, p = 0.01). There was no significant difference in operative time between the two groups. TURBT was associated with a significantly longer catheter duration (mean difference [MD] 0.98 days shorter in LBRT group; 95% confidence interval [95% CI] −1.45 to −0.5, p = < 0.00001), and length of stay (MD 1.12 days shorter in LRBT group, 95% CI −1.7 to −0.54, p = 0.0001).
Conclusions:
LRBT for bladder cancer has the benefit of reduced catheter duration, length of stay, and perforation without impacting negatively on operation duration, recurrence rates, or specimen quality.
Introduction
Transurethral resection of bladder tumor (TURBT) remains the gold standard treatment for nonmuscle invasive bladder cancer (NMIBC). 1,2 Despite being a well-established modality, complications such as the obturator nerve reflex (ONR) can result in perforation or injury to the iliac vessels. 3 Similarly, piecemeal resection has been shown to increase the risk of tumor recurrence via the scatter and reimplantation of tumor cells upon resection. 4,5 Various other methods, such as thulium and holmium laser resection, have been proposed as alternatives to standard TURBT, in an effort to alleviate some of the risks associated with the procedure. 6,7
Holmium laser, first utilized in urologic surgery in the early 1990’s, has been shown to have a noninferior safety and efficacy profile when compared to conventional TURBT. 8 The thulium laser, first applied to the field of urology in 2005, has been shown to have a reduced depth of penetration and smoother incision than its holmium counterpart. 9 This allows for precise en bloc resection, vaporization of tissue, and excellent hemostasis. 6 While various laser types have been used in the treatment of bladder cancer, holmium and thulium are the most frequent, with neither type demonstrating superiority of the other with regard to safety and efficacy in comparative studies. 10 With the rapidly evolving use of lasers in the field of urology, the potential of laser resection to replace conventional TURBT in the resection of bladder tumors has become a topic of interest. 11
Several randomized-controlled trials (RCTs) and observational studies have attempted to explore this issue, with limited consistency in their results. The aim of this study is to assess evidence from current RCTs and observational studies in the literature to compare outcomes in the laser resection and TURBT groups. Specifically, we examine the effectiveness of laser resection in terms of recurrence rates, ONR, bladder perforation, detrusor muscle acquisition, operative time, duration of catheterization, and length of inpatient stay.
Methods
Study design and reporting guidelines
This study is a systematic review of RCTs and cohort studies, following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines. 12 Our systematic review was registered on PROSPERO in February 2022 (ID: 329623).
Search strategy
The following databases were searched in February 2022: Medline PubMed, EMBASE and Web of Science. The following search terms were used: “transurethral resection*,” “bladder tumour*,” “laser*,” “TURBT,” “LRBT,” and “bladder cancer*.” The symbol “*” was used to allow variations on a word stem to be included in the search results. Furthermore, the following MeSH (medical subject headings) were used: (transurethral resection[MeSH] OR laser[MeSH] OR TURBT[MeSH] or LRBT[MeSH]) AND (bladder tumour[MeSH] OR bladder cancer[MeSH]). The last date of search was February 12, 2022. The grey literature (academic articles, research and committee reports, conference articles, and ongoing research) was also searched to further identify ongoing works of literature.
Types of study design included
Study designs were limited to RCTs, nonrandomized comparative studies and comparative observational studies comparing conventional and laser TURBT in the diagnosis and treatment of NMIBC. Animal studies, case reports, and conference abstracts were excluded.
Types of interventions included
Conventional TURBT and laser TURBT were evaluated. Studies were excluded if they failed to compare these interventions.
Types of outcome measures included
The primary outcomes were quantitative measures of detrusor muscle acquisition, recurrence perforation, and ONR. The secondary outcomes were total operative time, catheterization duration, and postoperative length of stay.
Study selection, data extraction, and risk of bias assessment:
A database was created using the reference managing software EndNote X9™. Two researchers (N.J.O.S. and E.M.C.) independently reviewed outcomes of the initial search.
After removal of duplicate, study titles were reviewed for potential relevance, followed by abstracts and full texts based on the inclusion criteria previously outlined. Conflicts between the two reviewers were resolved by open discussion, with final decision being made by an independent third reviewer where necessary.
The Cochrane Collaboration screening and data extraction tool, Covidence, was used to extract and store data efficiently. 13 Similarly, data were collected by two reviewers independently and conflicts between the two reviewers were resolved following an open discussion and final decision by the senior author.
A critical appraisal of the methodologic quality and risk of bias of the included studies was completed by two reviewers independently (N.J.O.S. and E.M.C.) using the Cochrane Collaboration's tool for assessing risk of bias was used for included RCTs and the Newcastle–Ottawa Scale for the remaining included studies. 14,15 Certainty of evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) tool for grading quality of evidence. 16
Data analysis
Statistical analysis was performed using Revman Statistical Software (Ver. 5 Copenhagen, Denmark). Binary outcome data were reported as odds ratios (OR) and 95% confidence interval (95% CI) and were estimated using the Mantel-Haenszel method whereas for continuous data, mean differences and 95% CI were estimated using inverse variance weighting. Outcome measures, in the format of mean, standard deviation (SD), and median/interquartile ranges were documented. If required, outcome variables (mean and SD) were estimated from the median and range (where provided) using the formula described by Hozo et al. 17 Heterogeneity was assessed by I 2 statistics, with anything over 50% being considered as considerable heterogeneity. A fixed effects model was applied where I 2 was <50%, whereas a random-effects model was applied in cases of considerable heterogeneity. Statistical significance was considered a p-value <0.05.
Results
Search results
Our initial search yielded 2832 results (Fig. 1). After the removal of duplicates, 1660 studies were assessed. After the initial screen, 253 abstracts were reviewed and assessed for eligibility, of which 30 were selected for full-text review. A total of 20 studies met our inclusion criteria and were included in our study. All studies were included in the quantitative analysis.
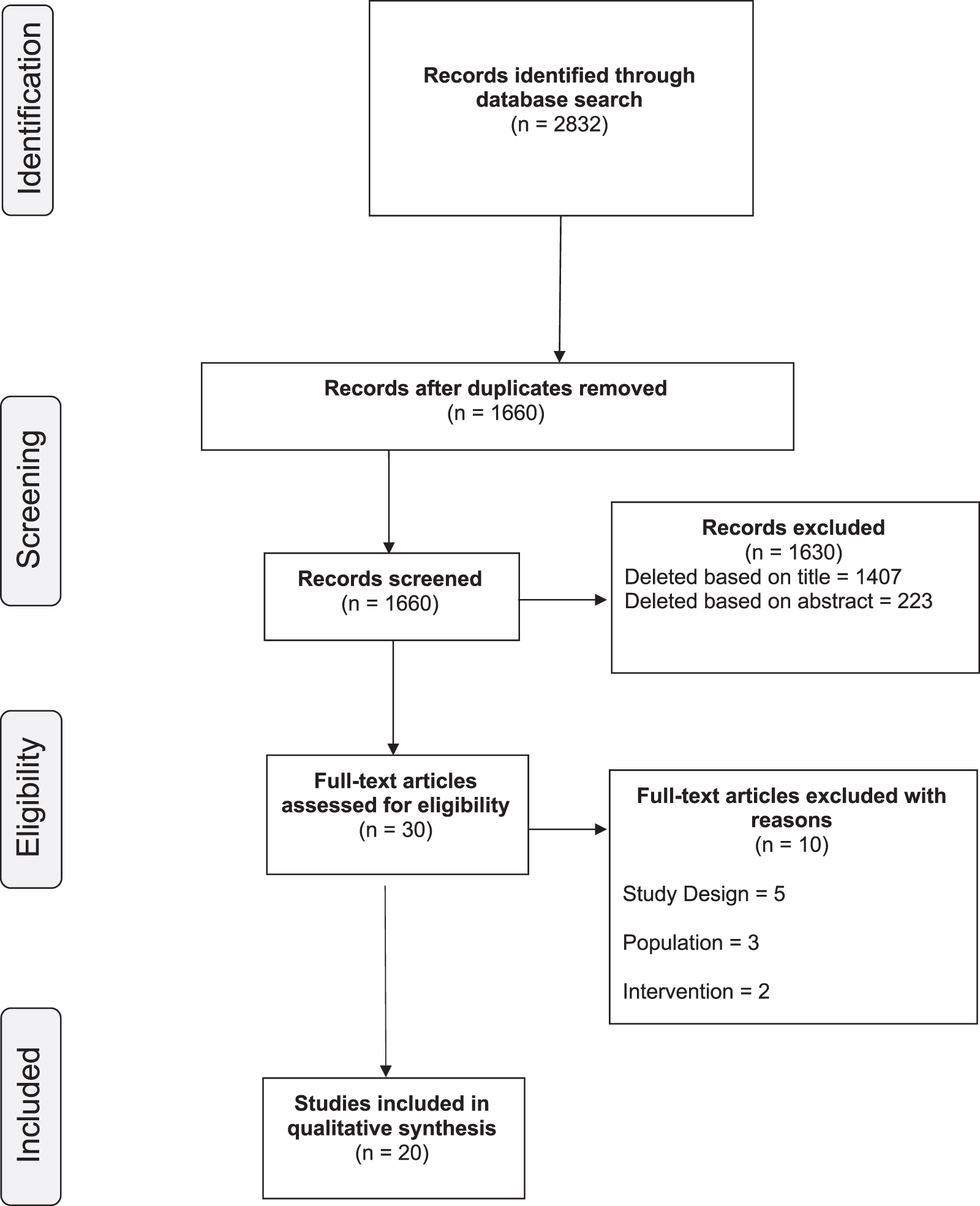
Study selection. A PRISMA flowchart of the selection of relevant publications included in this review. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Methodologic characteristics and quality of studies
Seven of the included studies were prospective RCTs. 7,18 –23 Six studies were prospective cohort studies. 24 –29 The remaining seven studies were retrospective cohort studies. 22,30 –35 Table 1 summarizes the methodologic characteristics of the included studies. The methodologic quality of the included studies was generally good and is presented in Table 2, and Figures 2 and 3. Six studies achieved a rating of 7 or higher on the Newcastle Ottawa Scale, meeting criteria for “high quality” studies. The GRADE certainty of evidence ranged from extremely low to low and is presented in Figure 4.

Risk of bias summary for RCTs (illustration a). RCT = randomized-controlled trial. Color images are available online.
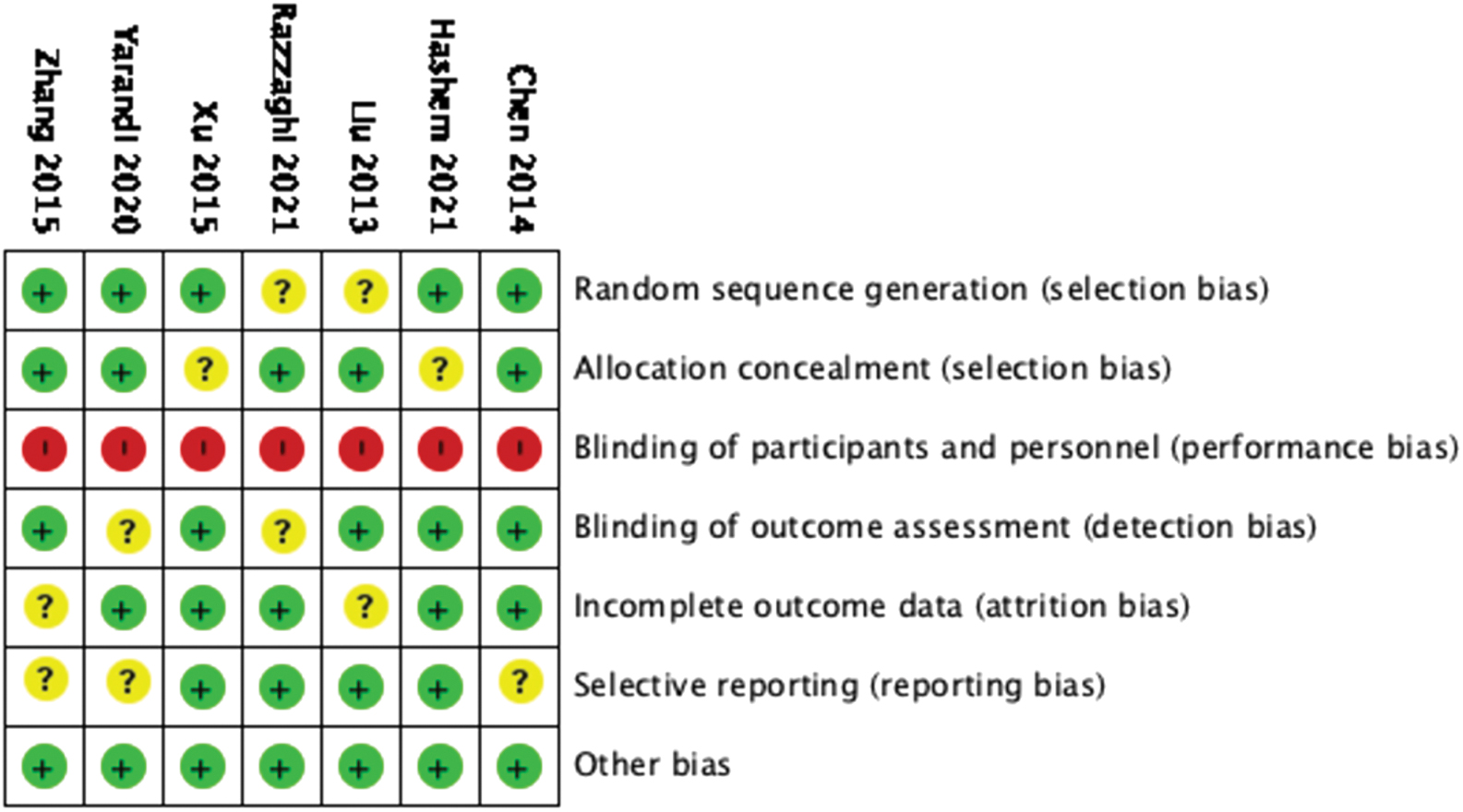
Risk of bias summary for RCTs (illustration b). Color images are available online.
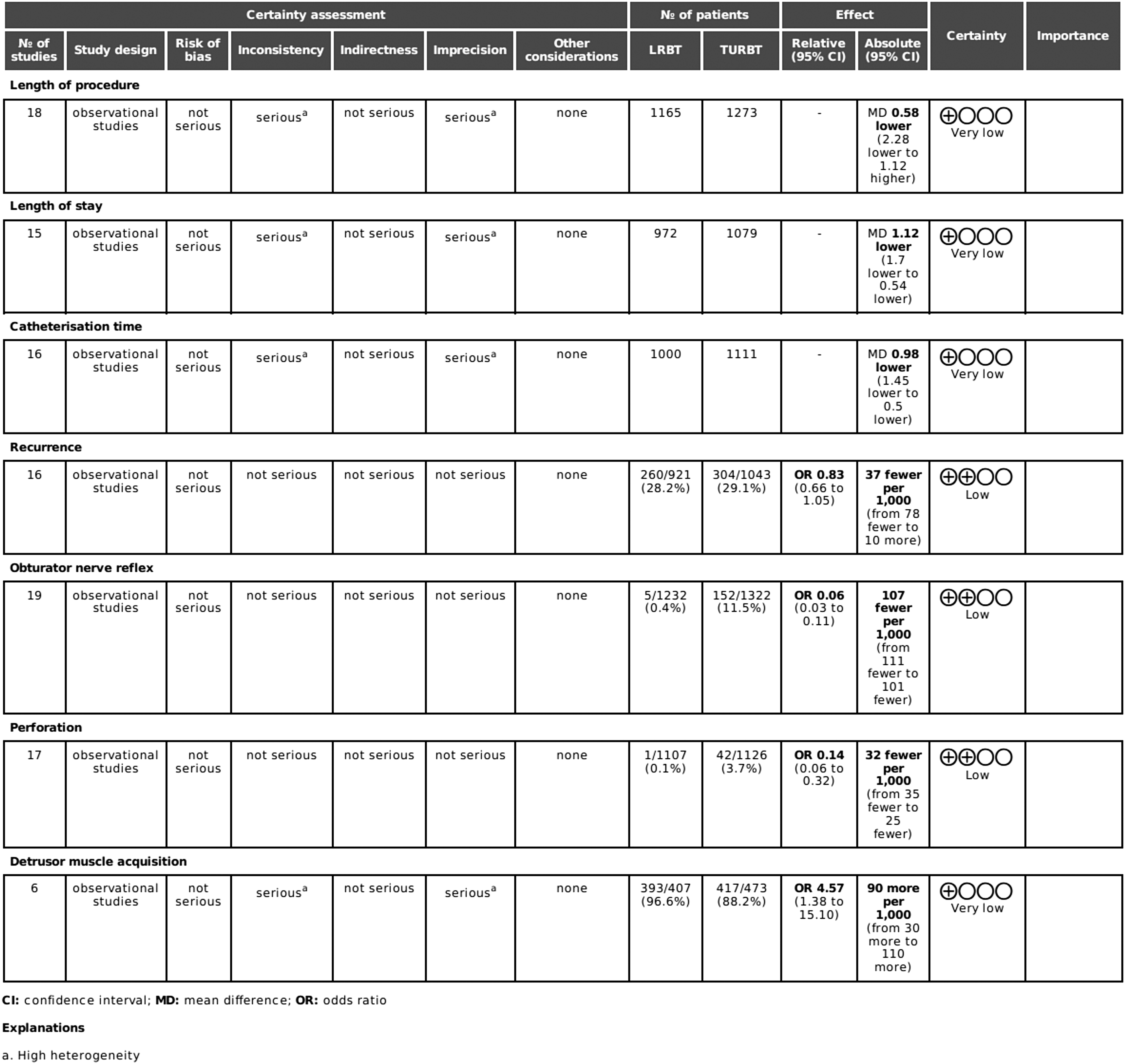
GRADE certainty of evidence table. GRADE = Grading of Recommendations, Assessment, Development, and Evaluations.
Methodologic Characteristics of the Included Studies
PCS = Prospective Cohort Study; RCS = Retrospective Cohort Study; RCT = Randomized Controlled Trial.
Newcastle Ottawa Scale Risk of Bias Assessment for Nonrandomized Studies
= 1 point; ** = 2 points; / = no points.
Participant characteristics
The total number of participants from the 20 included studies was 2621. Overall, 1257 patients underwent laser resection (73.9% male, 26.1% female), with the remaining 1364 patients undergoing conventional TURBT (75.5% male, 24.5% female). Mean age at operation was 63.1 ± 11.4 years in LBRT group and 63.7 ± 11.1 years in TURBT group. Median (range) follow-up was 24 (12–40) months. The baseline characteristics of participants are outlined in Table 2. Table 3 outlines the laser subtype and TURBT current compared in each study
Laser Subtype and Transurethral Resection of Bladder Tumor Current Used in Study
TURBT = transurethral resection of bladder tumor.
Tumor characteristics
Tumor characteristics were reported on and categorized in 18 studies (Table 4). Out of 1224 tumors, 2% were Tis (n = 24), 63.4% were Ta (n = 780), 33.2% (n = 420) were T1, and the remaining 1.4% (n = 17) were ≥T2. In terms of tumor grade, 9.2% (n = 68) were Papillary Urothelial Neoplasm of Low Malignant Potential, 64.2% (n = 473) were low grade, and the remaining 26.6% (n = 196) were high grade.
Tumor Characteristics
HG = high grade; LG = low grade; PUNLMP = papillary urothelial neoplasm of low malignant potential.
Surgical technique
Sixteen studies reported a breakdown of tumor resection technique. 7,18,19,22 –27,29 –34,36 En bloc resection of bladder tumor was performed in the laser TURBT groups in all 16 studies. Similarly, piecemeal resection was performed in all conventional TURBT groups in these studies.
Recurrence
Sixteen studies reported tumor recurrence rates postresection of bladder tumor. The recurrence rate was 28.2% (n = 260/921) in the laser resection of bladder tumor (LRBT) group and 29.1% (n = 304/1043) in the TURBT group. A meta-analysis of the included studies using an M–H fixed-effects model showed no significant difference between the two groups with regard to recurrence rates (OR 0.83, 95% CI, 0.66–1.05, p = 0.12), with no heterogeneity reported across the 16 studies (I 2 = 0%) (Fig. 5).
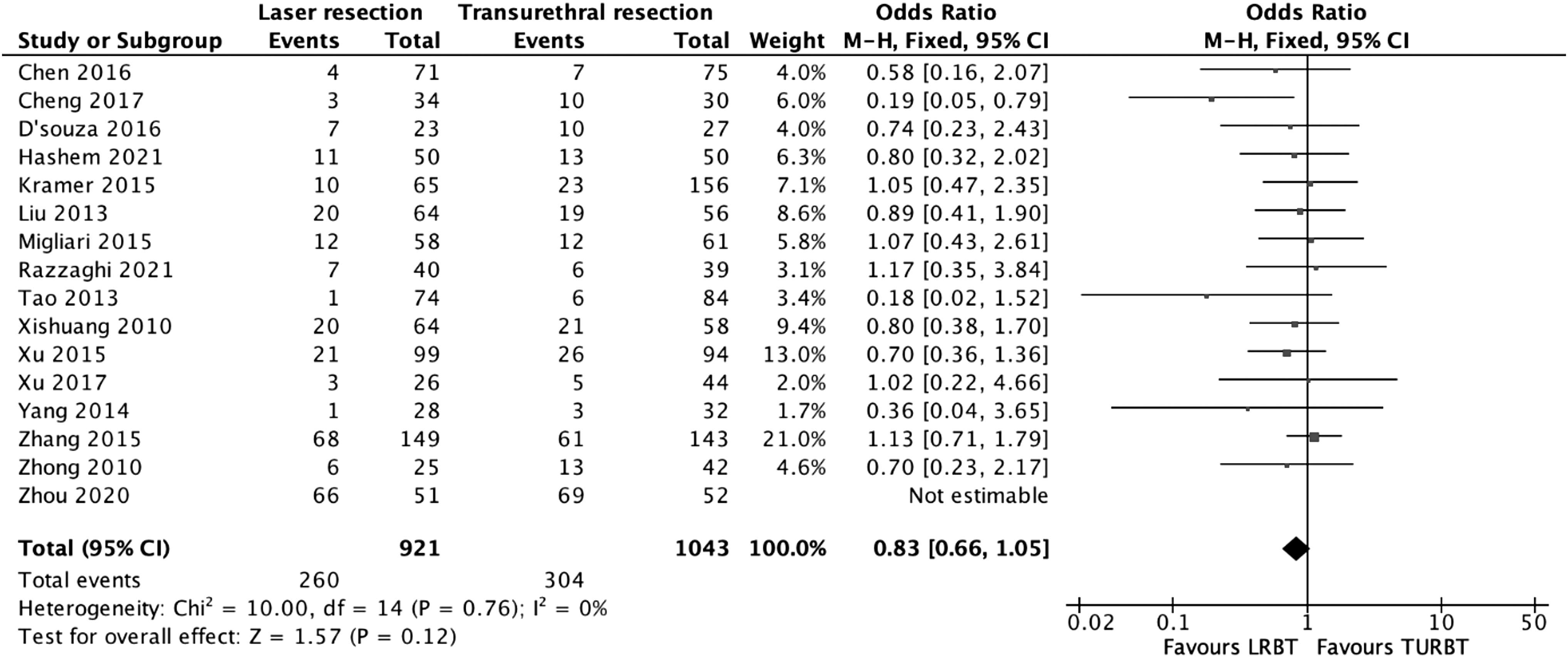
Recurrence meta-analysis results.
Bladder perforation
Seventeen studies reported bladder perforation rates between the two groups. Perforation was diagnosed on the table after an ONR in five studies 22,2325,32,36 and by CT imaging postoperatively in one study. 7 The remaining 11 studies did not provide a breakdown of the diagnosis of perforation. The rate of perforation was 0.009% (n = 1/1107) in the LBRT group and 3.7% (n = 42/1126) in the TURBT group. A meta-analysis of the included studies using an M–H fixed-effects model showed a significant difference between the two groups with regard to perforation rates, in favor of laser resection (OR 0.14, 95% CI 0.06–0.32, p = < 0.0001), with no heterogeneity reported between the studies (I 2 = 0%) (Fig. 6).
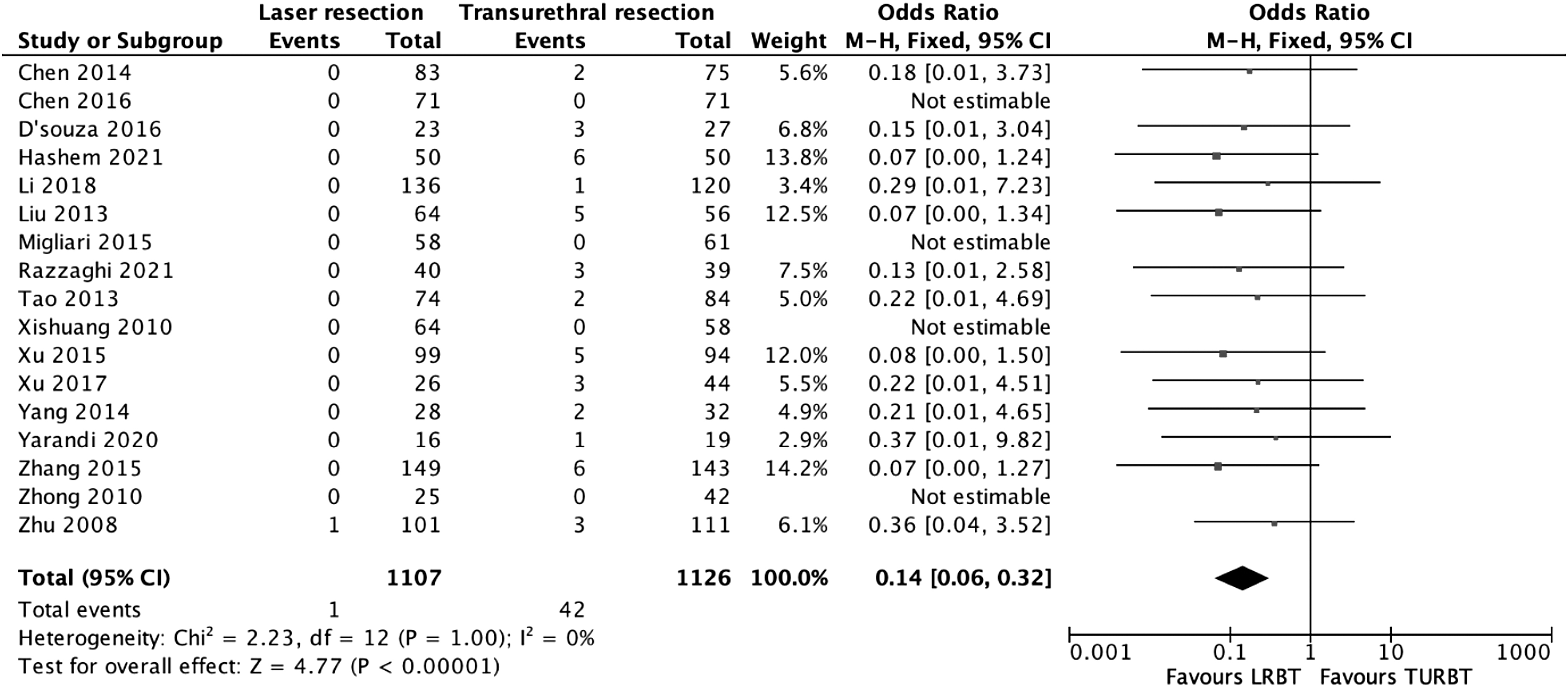
Perforation meta-analysis results.
Detrusor muscle acquisition
Six studies reported detrusor muscle acquisition rates between the two groups. The rate of detrusor muscle acquisition was 96.6% (n = 393/407) in the LRBT group and 88.1% (n = 417/473) in the TURBT group. A meta-analysis of the included studies using an M–H random-effects model showed a significant difference between the two groups with regard to detrusor muscle acquisition, in favor of LBRT (OR 4.57, 95% CI 1.38–15.10, p = 0.01), with considerable heterogeneity between the studies (I 2 = 59%) (Fig. 7).
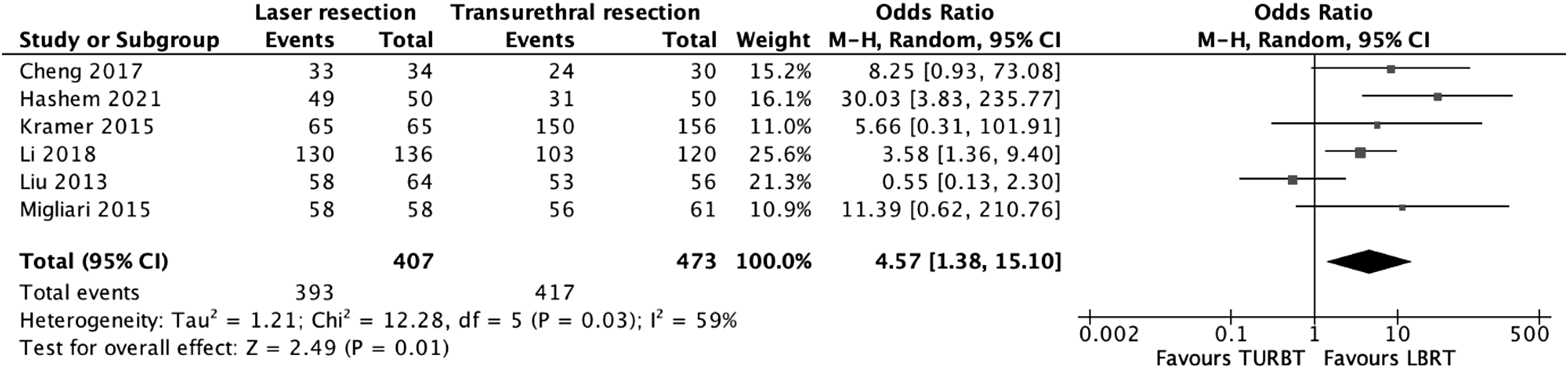
Detrusor muscle acquisition meta-analysis results.
Operative time
Eighteen studies reported on operative time (minutes). A meta-analysis performed using the random-effects model revealed a marginally reduced operative time in the LRBT group, however, these results were not statistically significant (mean difference [MD] was 0.58 minutes shorter in LRBT group; 95% CI, −2.28 to 1.12, p = 0.5). Considerable heterogeneity was found (I 2 = 73%) (Fig. 8).

Operative time meta-analysis results.
Catheterization duration
Sixteen studies reported duration of catheterization between the two groups. A meta-analysis performed using the random-effects model revealed a significant reduction in duration of catheterization in the LRBT group (MD 0.98 days shorter in LBRT group; 95% CI, −1.45 to −0.5, p = < 0.00001), with considerable heterogeneity between studies (I 2 = 96%) (Fig. 9).

Catheterization duration meta-analysis results.
Length of stay
Fifteen studies reported length of stay. A meta-analysis performed using a random-effects model revealed a significant reduction in length of stay in the LRBT group (MD 1.12 days shorter in LRBT group, 95% CI −1.7 to −0.54, p = 0.0001), with considerable heterogeneity between studies (I 2 = 97%) (Fig. 10).
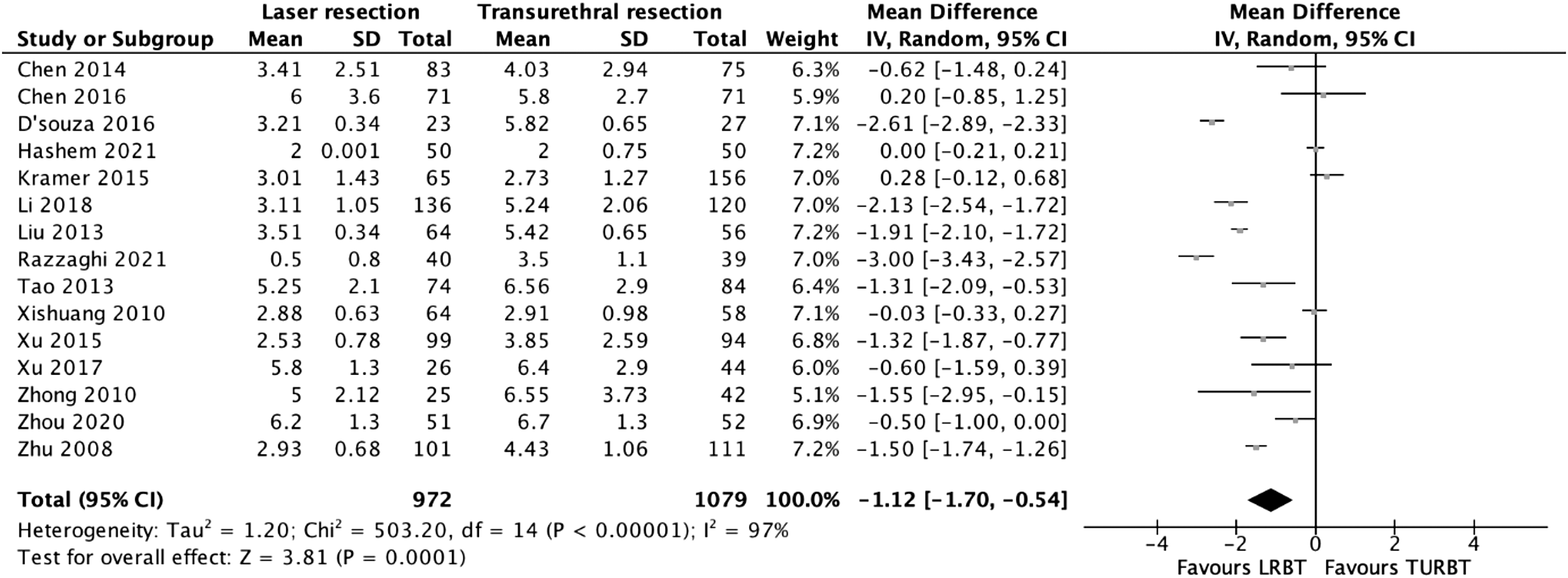
Length of stay meta-analysis results.
Obturator nerve reflex
Nineteen studies reported on ONR rates between the two groups. Obturator kick rate was 0.4% (n = 5/1232) in the LRBT group and 11.5% (n = 152/1322) in the TURBT group. A meta-analysis of the included studies using an M–H fixed-effects model showed a significant difference between the two groups with regard to ONR rates, in favor of laser resection (OR 0.06, 95% CI 0.03–0.11, p = < 0.00001), with no heterogeneity reported between the studies (I 2 = 0%) (Fig. 11).

ONR meta-analysis results. ONR = obturator nerve reflex.
Discussion
Our results demonstrate significant advantages of LRBT compared to traditional TURBT in terms of reducing perforation, duration of catheterization, detrusor muscle acquisition, postoperative length of stay, and ONR, without sacrificing oncologic outcomes. There was no significant difference between the two groups for tumor recurrence. Overall, our results show that where practical and affordable, utilizing LBRT over TURBT can reduce perioperative morbidity and length of stay and should be the treatment modality of choice in favorable tumors. To our knowledge, this is the most up-to-date meta-analysis incorporating data from both randomized and nonrandomized studies available in the literature.
The economic burden of managing bladder tumors is one of the highest of all cancers, exacerbated by long inpatient stays and the need for repeat procedures. 37 A low risk of progression in combination with a high risk of recurrence results in this highly comorbid group of patients often undergoing multiple procedures as well as readmissions and interventions for perioperative complications. 38 While laser equipment is generally more costly than conventional TURBT equipment, a reduced postoperative stay might have the potential to offset this cost. 39 Wong et al demonstrated the safety, tolerability, and cost-effectiveness of performing outpatient laser ablation for NMIBC under local anesthesia over traditional inpatient cystodiathermy. 38
The authors concluded that over the course of a patient's lifetime, outpatient laser ablation was more clinically effective and less costly than conventional inpatient cystodiathermy. Fewer inpatient days, coupled with reduced perioperative complications, highlights the potential for substantial cost-savings to be made when opting for a laser approach to resecting NMIBC.
The incorporation of lasers into urologic procedures has made the treatment of elderly patients with multiple comorbidities more feasible, as it eliminates the need to modify anticoagulant treatment. 39 Depending on the wavelength, absorption by water and hemoglobin, and depth of penetration, lasers can be utilized to coagulate, vaporize, or enucleate. 39 Similarly, lasers can be used safely in patients with pacemakers, due to the lack of an electrical current in its mechanism. 11 The European Association of Urology (EAU) acknowledges the use of Thulium-Yttrium Aluminium Garnet (YAG) or Holmium-YAG laser in resecting selective exophytic bladder tumors; however, concludes that “the technique selected is dependent on the size and location of the tumor and experience of the surgeon.” 2 In bladder tumor resections, the laser instrument is in a noncontact state with the bladder mucosa and therefore no electrical current passes through the tissue and surrounding nerves, effectively eliminating the risk of an ONR. 11
Piecemeal resection, a technique commonly used in TURBT, is well known to increase the risk of tumor recurrence via the scatter and reimplantation of tumor cells upon resection. 4,5 This “incise and scatter” technique disregards oncologic principles, as it essentially involves breaching surgical margins, increasing the risk of seeding and tumor fragment reimplantation, thus augmenting the risk of recurrence and progression. 1 The mechanics of laser resection allow for a coagulation zone to form beneath the vaporized tissue, thereby potentially reducing the spread and seeding of tumor cells. 40,41
In certain cases, large tumors (2–4 cm) may be unsuitable for en block resection, due to the inability to extract them intact via a resectoscope sheath. 42 TURBT is an acceptable alternative in these circumstances, offering similar oncologic outcomes. While many studies have demonstrated the safety and efficacy of LRBTs, the sample sizes within these studies have generally been small and inadequately powered. We aimed to pool data from both these small studies as well as larger cohort and randomized trials, to investigate whether one treatment modality had a clear benefit over another from a safety and efficacy standpoint.
Our review has several limitations. There is a lack of long-term data on tumor recurrence in the literature, and we were therefore only able to analyze recurrence in the short term, up to 24 months. Further research is required to evaluate the superiority of one modality over another with regard to long-term recurrence rates. Finally, there was considerable heterogeneity between the included studies on several of our outcomes, likely due to a variation in practice, technique, and patient condition between centers.
Conclusion
Our review demonstrated a significant advantage of LRBT over TURBT in terms of ONR, perforation, duration of catheterization, detrusor muscle acquisition, and postoperative length of stay, without impacting tumor recurrence rates. Overall, LRBT appears to be a safe and feasible option in the treatment of bladder tumors, with the potential to become a new gold standard in the future.
Footnotes
Authors' Contributions
N.J.O.S. and E.M.C.: Project development, data collection, and article writing; H.C.T. and A.N.: Data collection and article writing; N.F.D.: Project development and article writing.
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Research Committee and with the Declaration of Helsinki 1975 and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was recieved for this research.