
Abstract
Background:
In robot-assisted partial nephrectomy (RAPN) renorrhaphy is used to achieve hemostatic control of the tumoral resection bed, with detrimental impact on renal function. Hemostatic agents are used to achieve rapid and optimal hemostasis. GATT-Patch is a new hemostatic sealant that has already demonstrated promising results.
Objective:
Compare GATT-Patch and standard renorrhaphy in terms of hemostatic capacity, ischemia time, and prevention of urinary leakage after RAPN in a porcine model.
Design, Setting, and Participants:
In this preclinical randomized controlled trial, four pigs underwent 32 RAPNs. After resection, GATT-Patch application and performance of classic renorrhaphy were randomized. After the procedure, the resection bed was reinspected. A necropsy study evaluated the adhesiveness of the patch, and retrograde pyelography was performed to determine the leakage burst pressure.
Intervention:
Application of GATT-Patch and performance of classic renorrhaphy were randomized and surgeons blinded to the hemostatic technique to be performed.
Outcome Measurements and Statistical Analysis:
Warm ischemia, hemostatic control, active bleeding during hemostatic control, total procedure time, bleeding at reinspection, and presence of urinary leakage on retrograde pyelography were recorded. Continuous variables were compared using the Student t-test. Categorical variables were compared using the Chi-square or Fisher's exact test.
Results and Limitations:
GATT-Patch reduced warm ischemia time (WIT), time to achieve hemostatic control, active bleeding time, and total procedure time, achieving hemostasis in 100% of the cases. Rebleeding at reinspection occurred in 0% of the GATT-Patch group. Renal parenchyma damage was observed in 100% of renorrhaphy cases and in 0% of GATT-Patch cases.
Conclusions:
GATT-Patch guaranteed optimal hemostasis and urine sealant effect after RAPN in porcine models. Compared to renorrhaphy, we observed a reduction in WIT, total procedure time, and potential reduction in healthy parenchyma loss.
Patient Summary:
GATT-Patch stops bleeding and provides hemostasis faster than suturing after resection of portions of the kidney in pigs. It might be tested in patients undergoing partial nephrectomy for kidney cancer.
Introduction
Partial nephrectomy is a common procedure due to the increased incidence of renal-cell carcinoma. 1 It is challenging since arterial clamping and double-layer renorrhaphy are used to control bleeding and obtain rapid hemostatic control of the tumoral resection bed. 2 Robot-assisted partial nephrectomy (RAPN) decreased the learning curve and technical difficulty of renorrhaphy, although this step can still significantly prolong ischemia time. 3,4 Moreover, suturing causes loss of healthy parenchyma, having a detrimental impact on renal function. 4 –6 However, secure and durable parenchymal hemostasis is mandatory.
In this context, several hemostatic agents have been evaluated to quickly and safely control bleeding after PN. 6 In the case of selective suturing and sutureless RAPN, they help achieve hemostasis and prevent leakage of urine from the renal collecting system. A new poly(2-oxazoline)-based hemostatic sealant (NHS-POx), GATT-Patch, is a biodegradable, hemostatic sealant that has already demonstrated promising results in other applications. 7 With specific design features for hemostatic performance even in severe bleeding and with flexibility and pliability to allow ease of use in minimally invasive procedures, its use during RAPN may present a safe and effective solution to reduce the requirement of suturing, yet provide durable hemostatic seal.
In this preclinical randomized controlled trial, we compared GATT-Patch and double-layer standard renorrhaphy in terms of hemostatic capacity, prevention of urinary leakage, and ischemia time after RAPN in a porcine model.
Materials and Methods
This experiment complies with the national and international guidelines for the care and use of laboratory animals. Four anesthetized pigs (60–80 kg) were used. Bilateral synchronous upper- and lower-pole, anterior and posterior surface transperitoneal RAPNs were simulated. The standard pneumoperitoneum setting used was 8 mm Hg. Three expert surgeons performed 32 pseudotumoral resections. Each renal defect produced was 20–30 mm in diameter and 10–15 mm in depth. The opening of the urinary collecting system was confirmed by endoscopic visualization. Blood pressure was registered before creating the lesion.
The application of GATT-Patch and the performance of classic inner and outer renorrhaphy were randomized such that the surgeon was unaware of the hemostatic technique to be performed until the renal resection defect was completed. Half of the GATT-Patch was applied at the depth of the lesion, and the other half was applied on top of the previous one, overlapping nonbleeding parenchyma by at least 1 cm on all sides. Thirty seconds of pressure with a saline wet gauze was initiated, after which hemostasis was checked by careful removal of the gauze. If bleeding persisted, additional 30 seconds of pressure was applied. If bleeding persisted, an additional GATT-Patch could be applied. There was no maximum to how much GATT-Patch could be used. Hemostasis was checked after lowering the pneumoperitoneum pressure below the diastolic pressure of the animal.
When four RAPNs were performed in each kidney, a Hem-O-Lok was placed in the ureter to produce hydronephrosis, potentially increasing the likelihood of urine leakage from the resected areas. When eight RAPNs were performed the animal remained anesthetized during 3 hours, after which the surgeon reinspected resection beds for rebleeding and/or urine leakage. In the case of bleeding its severity was scored by two trained investigators according to the Severity Bleeding Surface Scale (SBSS) (Supplementary Appendix SA1). 8 –10
To evaluate hemostatic performance, the “initial hemostasis” was defined as an SBSS of 0 at the end of the hemostatic control period, and the “rebleeding at reinspection” was defined as an SBSS >0 at robotic reinspection.
Warm ischemia, hemostatic control, active bleeding during hemostatic control, and total procedure time were recorded. Warm ischemia time (WIT) was measured between the moment a bulldog clamp was placed on the renal artery before resection and until unclamping. Early unclamping was performed in the renorrhaphy group. In the GATT group, unclamping was performed after the initial 30 seconds of compression and upon removal of the gauze. For the GATT-Patch group, hemostatic control was measured between the placement and removal of the wet gauze, and for the renorrhaphy group it was measured between the first inner renorrhaphy stitch and the removal of all needles upon completion of renorrhaphy. Active bleeding time was defined as the time during which active bleeding occurred during the hemostatic control phase. Total procedure time began with the placement of the bulldog clamp on the renal artery, including resection of the pseudotumor and completion of hemostatic control.
Following euthanasia and completion of reinspection, a necropsy study evaluated the adhesiveness of the GATT-Patch to the resection bed. Retrograde pyelography was performed by introducing a 5F ureteral catheter into the mid-ureter and injecting ∼15 mL of a mixture of saline and methylene blue with gentle steady pressure. A digital monitor (GMH 3151®; Greisinger, Regenstauf, Germany) connected to a digital sensor (GMSD 25® MR-K31; Greisinger) was used to monitor the fluid injection and determine the burst pressure point. After pressure measurements were completed, the size of the pseudotumoral resection area was measured. Kidney damage was evaluated by observing a change in color of its parenchyma, from red rose to dark purple.
The usability of GATT-Patch was evaluated by observing the ease and effectiveness of introducing it through the 12 mm AirSeal® trocar, its maneuverability inside the abdomen, and placement onto the resection site with robotic instruments. The adhesion of the wet gauze to GATT-Patch and its adhesion to the pseudotumoral area were evaluated and rated as “Pass” if the patch could not be easily removed. Four surgeons (three console surgeons and one tableside assistant surgeon) completed a GATT-Patch usability questionnaire using a 5-point Likert scale (Supplementary Appendix SA2).
Statistical analysis was performed using the IBM Statistical Package for the Social Sciences Version 26.0 (IBM Corp, Armonk, NY). Continuous variables were expressed as mean and standard deviation and compared using Student's t-test. Categorical variables were presented as frequencies and compared using the chi-square or Fisher's exact test, where appropriate. Statistical significance was set at p < 0.05.
Results
Baseline characteristics
A total of 32 resection areas were created and randomized into 16 GATT-Patch and 16 renorrhaphy-treated areas. Blood pressure at the time of resection was comparable between both groups: 68.3 ± 12.5 vs 71.1 ± 12.3 mm Hg (p = 0.53). The size of the resected area, as confirmed at the time of necropsy, was also comparable for the diameter (GATT-Patch vs renorrhaphy: 2.6 ± 0.4 vs 2.6 ± 0.5 cm (p = 0.85) and depth (GATT-Patch vs renorrhaphy: 1.4 ± 0.1 vs 1.4 ± 0.1 cm (p = 0.30) (Fig. 1).

Creation of resection area and systematic opening of the renal collecting system. Color images are available online.
GATT-Patch handling
It was easily rolled up and introduced through the trocar without damaging the patch. In one case, it was damaged, but could still be used for hemostasis. It could be easily maneuvered inside the body and placed at the bleeding site. The gauze used for the application did not stick to the GATT-Patch and could easily be removed without damaging it. All surgeons responded with “Strongly Agree” or “Agree” on its usability (Supplementary Appendix SA2).
Procedural times
GATT-Patch significantly reduced all specific times (Table 1). The WIT was reduced by 40% (p = 0.004), time to achieve hemostatic control by 300% (p < 0.001), active bleeding time by 1142% (p < 0.001), and total procedure time by 227% (p < 0.001) (Table 1).
Procedural Times of GATT-Patch vs Suturing
Suture group = start renorrhaphy until removal of needles; GATT-Patch group = placement gauze until removal of gauze from the patch.
Arterial clamping+lesion creation for hemostasis (end renorrhaphy/patch application).
WIT, warm ischemia time.
Initial hemostasis
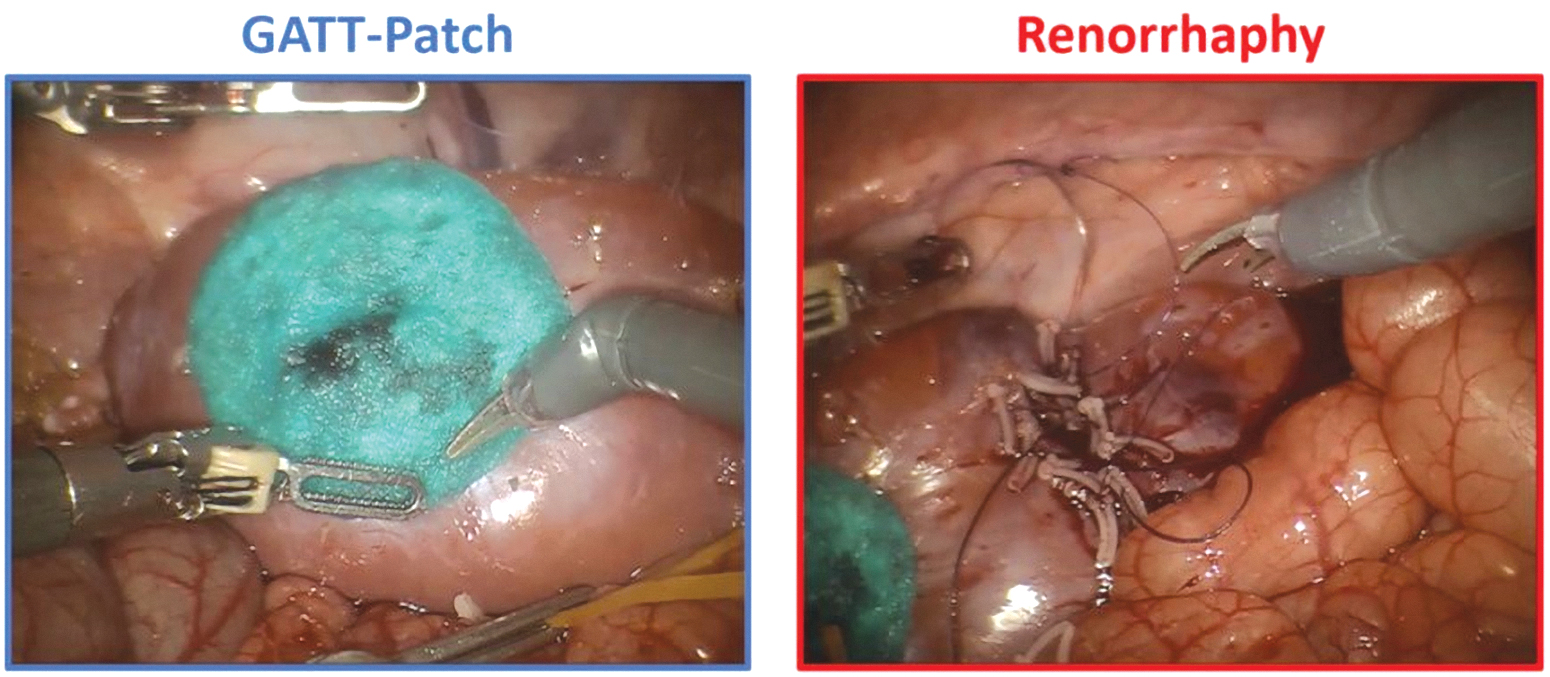
Active bleeding during hemostatic control was 19% with GATT-Patch vs 94% with renorrhaphy (p < 0.001); however, initial hemostasis was achieved in 100% of patients in both groups (p > 0.99). An example of the final result is shown in Figure 2.
GATT-Patch achieved hemostasis with 30 seconds of pressure in 81% of the cases (n = 13/16). Additional hemostatic maneuvers were required in three cases due to persistent bleeding. This consisted of additional 30 seconds of pressure in one case and additional GATT-Patch placements in two cases (case two required two and case three required three additional half GATT-Patches).
Rebleeding assessment
The time between achieving hemostasis and reinspection was 3:50 ± 1:14 hours for GATT-Patch vs 3:49 ± 1:08 hours for renorrhaphy (p = 0.96). Rebleeding at reinspection occurred in 0% for GATT-Patch vs 12.5% (n = 2/16) for renorrhaphy and consisted of SBSS 1 (e.g., minimal bleeding) at both times (p = 0.48).
Urine sealing
The time between clipping the ureter and reinspection was 3:28 ± 1:08 hours for GATT-Patch vs 3:28 ± 1:09 hours for renorrhaphy (p = 0.99). There was no urine leakage upon reinspection in any group. At the time of necropsy, burst pressure measurements were performed in three of the four pigs because the pressure system malfunctioned during the assessment in the first animal. In the other three animals, burst pressures were well above physiologic levels (Table 2).
Pressure Test of Treatments
The test was not performed until the burst occurred because it was considered a sufficiently high pressure to withstand clinical scenarios.
Adhesion of GATT-Patch to the kidney
At the time of necropsy, adhesion of GATT-Patch to the renal parenchyma was rated as “Pass” for all applications and could not be easily removed by pulling on its edge.
Kidney damage
During surgery and robotic reinspection (Fig. 3), a dark purple renal parenchyma was observed around the renorrhaphy area in 100% of the cases and in 0% of the GATT-Patch treated areas (p < 0.001).

Examples of kidney damage as a result of suturing. Color images are available online.
Discussion
We evaluated GATT-Patch against classic double-layer renorrhaphy to determine whether it provides more efficient and effective control of bleeding and collecting system closure in simulated RAPN cases. Partial nephrectomy (PN) is strongly recommended, as it has been shown to be superior to radical nephrectomy in terms of functional outcomes and overall survival while guaranteeing noninferior oncologic control. 11 PN allows for better preservation of kidney function, lowering the risk of end-stage renal disease, cardiovascular disorders, and cardiovascular-specific mortality rate. 12
RAPN is becoming the standard of care for the management of renal masses. 13 Depending on the surgeon's expertise and tumor characteristics, open or laparoscopic approaches can be used. 14 However, the invasiveness of open surgery and the steep learning curve of the laparoscopic approach justify the wide dissemination of the less technically challenging RAPN. 15
Despite the advantages of RAPN, it remains one of the most challenging urologic procedures to perform. First, owing to the rich vascularization of the kidney, bleeding control is demanding. Therefore, renal artery clamping can be used to reduce perfusion of the kidney and control excessive bleeding, which can compromise the visualization of the resection bed and endanger patient's life. But WIT during arterial clamping is an important predictor of postoperative renal function 3 and should therefore be as short as possible. In our study, we found that GATT-Patch reduced WIT by 40% compared with standard renorrhaphy. This may have a significant impact on the degree of renal parenchymal preservation and long-term renal function.
Second, achieving satisfactory hemostasis is a demanding but non-negotiable requirement after tumor excision. Different renorrhaphy techniques have been proposed to maximize the preservation of vascularized parenchyma, achieve complete hemostasis, and close the collecting system. 4 However, the classic and most effective hemostatic approach is suture ligation of the bleeding vessels and renal parenchyma by performing inner and outer renorrhaphy. Having no consensus on the optimal approach, with this two-layer technique, the inner layer closes the collecting system and ligates the bleeding vessels of the tumoral bed, and the outer layer closes the renal cortex and parenchyma. 16 Using this technique, we achieved optimal hemostasis after all resections, even when polar branches with ≥3 mm were open. Compared with double-layer renorrhaphy, GATT-Patch guaranteed the same rate of initial hemostasis (100%), with a significant reduction in active bleeding during hemostatic control. Moreover, we observed two cases of rebleeding at reinspection for renorrhaphy and none for GATT-Patch, but this difference was not statistically significant. GATT-Patch was able to achieve hemostasis within 30 seconds in most cases; therefore, we report a large reduction in the time to achieve hemostatic control and of active bleeding during the procedure meaning that the overall time of the procedure using standard renorrhaphy was twice that of GATT-Patch, and suggesting a significant reduction in the operating room time and related costs, although the magnitude of time reduction cannot be easily translated from pig models to real patients.
Third, in the posteuthanasia retrograde pyelography monitoring of intraureteral pressure to determine the burst pressure point, the authors reached pressures above the physiologic levels, suggesting the potential clinical safety of GATT-Patch in guaranteeing closure of the renal collecting system.
Different hemostatic sealants have been introduced to help achieve hemostasis and prevent urine leakage.
17,18
Working as thrombotic promoters, they have distinct sealant mechanisms and are used in conjunction with other hemostatic maneuvers.
17,18
Few studies have compared the use of hemostatic sealants with renorrhaphy. Although they presented promising results by providing adequate hemostasis and significantly decreased the blood loss and transfusion rate, as well as renal ischemia and operative times, none of them showed safe and effective use in lieu of traditional two-layer renorrhaphy.
19,20
However, GATT-Patch, which is a new NHS-POx polymer-based, biodegradable hemostatic sealant, may present a reliable alternative to renorrhaphy. It has demonstrated promising results compared to other commercially available hemostatic agents, TachoSil® and Veriset®, in previous preclinical models of open surgery and is currently being evaluated in a first human clinical trial of patients undergoing open liver surgery (
While previous studies suggested that hemostatic agents were not associated with significant benefits, GATT-Patch might change this paradigm since it was able to control arterial bleeding without the need for suturing. 21,22 Surgeons experienced a high hemostatic effect during surgery and were able to complete the procedure without renorrhaphy. At necropsy reinspection, its strong adhesiveness to the pseudotumoral resection bed was evident, as well as the contrast between the dark purple color around the renorrhaphy areas, presumably due to renal parenchyma ischemia induced by renorrhaphy and the red rose healthy parenchyma around the GATT-Patch treated areas. Finally, the retrograde pyelography evaluations suggest its capacity to produce a watertight closure of the renal collecting system, since leakage was only identified when supraphysiologic intraureteral saline pressures were produced. GATT-Patch might potentially help reduce the steep learning curve of RAPN and laparoscopic PN, democratizing these procedures to less experienced surgeons and low-volume surgical centers.
This study had some limitations. First, this was a single-center preclinical study. Second, porcine kidneys have minimal amount of fat, thin capsule, and do not bleed like human kidneys. 23 Third, renal function was not evaluated before or after RAPN. To overcome these limitations, our findings should be confirmed in a large prospective randomized multicenter clinical study. Future studies might use calf models because of their close similarity to the human kidney, and a systematic evaluation of renal function, kidney damage on long-term necrosis, and resection bed healing should be performed in a survival study.
Conclusions
In this preclinical randomized controlled trial, the topical hemostatic sealant GATT-Patch was found to be a valid alternative to standard double-layer renorrhaphy, guaranteeing optimal, fast, and durable hemostasis and urine sealant effects after RAPN in porcine models. The reduction in warm-ischemia time, total procedure time, and healthy parenchyma loss has the potential to make renorrhaphy obsolete and reduce the steepness of the RAPN learning curve. Further research is required to translate these findings into clinical practice.
Footnotes
Authors' Contributions
R.F.: conceptualization, data curation, investigation, methodology, validation, writing (original draft), writing (review & editing). R.D.G.: conceptualization, data curation, formal analysis, investigation, methodology, validation, writing (review & editing). P.Z.: conceptualization, data curation, formal analysis, investigation, methodology, validation, writing (review & editing). M.P.: investigation, visualization, writing (original draft), writing (review & editing). E.R.: conceptualization, data curation, funding acquisition; methodology, project administration, visualization, writing (review & editing). S.H.: conceptualization, data curation, funding acquisition, methodology, project administration, visualization, writing (review & editing). L.S.: investigation, validation. C.B.: investigation, validation. A.M.: investigation, validation. S.P.: investigation, validation. P.D.B.: investigation, validation. G.D.N.: supervision, writing (review & editing). A.M.: conceptualization, investigation, methodology, project administration, supervision, validation, writing (review & editing).
Ethical Approval
All procedures performed in studies involving animal participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Patient Summary
GATT-Patch is a hemostatic agent that can stop bleeding faster than suturing after resection of portions of the kidneys in pigs. It might be tested as an alternative to suturing in patients undergoing PN for kidney cancer.
Author Disclosure Statement
The authors declare that E.R. and S.H. are full-time employees of GATT Technologies B.V. (Nijmegen, The Netherlands). All other authors have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this article.
Funding Information
This study was funded by GATT Technologies B.V. (Nijmegen, The Netherlands).
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.