
Abstract
Introduction/Background:
There are increasing reports of serious complications related to the air pyelography technique, which raise concerns about the safety of room air (RA) injection into the renal collecting system. Carbon dioxide (CO2) is much more soluble in blood than nitrogen and oxygen and thus considerably less likely to cause gas emboli. Iodinated contrast medium (ICM) is expensive, and supplies may not be as reliable as previously assumed. CO2 pyelography (CO2-P) techniques using standard fluoroscopy and digital subtraction fluoroscopy (CO2 digital subtraction pyelography [CO2-DSP]) are described.
Materials and Methods:
During the endourologic stone cases, 15 to 20 mL of CO2 gas was typically injected into the renal pelvis through a catheter or sheath. Imaging was usually obtained with endovascular CO2 digital subtraction angiography settings using either a traditional fluoroscopy system (TFS) or robotic arm multiplanar fluoroscopy system (RMPFS) (Artis Zeego Care+Clear®; Siemens).
Results:
CO2-P was performed in 22 endoscopic stone treatment cases between March 2021 and August 2022, primarily using digital subtraction settings in 20 cases. CO2-DSP overall provided higher quality images of the renal pelvis and collecting system than CO2-P, but with a relatively higher radiation dose. Following a quality intervention, fluoroscopy doses for CO2-DSP cases were decreased by 81% overall. The use of CO2-P avoided fluoroscopic or intraoperative CT (ICT) artifacts seen with intraluminal ICM.
Conclusions:
CO2-P allows the urologist to obtain imaging of the renal collecting system without ICM and with much lower risk of air embolism compared with RA pyelography. CO2 is a nearly cost-free alternative to ICM. Because CO2 is widely available and the technique is easy to perform, we propose that CO2-P should be favored over traditional air pyelography to improve patient safety.
Introduction
Iodinated contrast medium (ICM) and room air (RA) are the two primary contrast media used during endourologic procedures. RA pyelography distinguishes posterior and anterior calices for needle targeting when obtaining fluoroscopic percutaneous renal access 1 and can substantially decrease radiation exposure with percutaneous nephrolithotomy (PCNL). 2 Problematically, there are multiple reports of serious morbidity attributed to air emboli after RA pyelography performed during stone surgery, including cardiopulmonary arrest, blindness, and paraplegia. 3 –7
A pyelovenous backflow mechanism was proposed in a description of two cases of nonsymptomatic air emboli identified during diagnostic air pyelography. 8 While much more commonly used during endoscopic stone treatment, ICM is expensive and can cause artifacts that can be mistaken for persistent stones. Additionally, the COVID pandemic has revealed that availability may not be as reliable as previously assumed. 9
Carbon dioxide (CO2) can be used as a nearly cost-free contrast medium in quantities typically used for imaging. CO2 pyelography (CO2-P) was previously reported in 1984, but not subsequently. 10,11 There is a more robust body of evidence in vascular surgery for using CO2 as the contrast medium, especially using digital subtraction-enhanced angiography (CO2-DSA). 12,13 Used commonly since the early 1980s, this technique involves storage of an initial image in memory and then removing any common elements (e.g., bone) in subsequent images.
Modern equipment integrates multiple images into textured composite images using stacking software. 14 Additionally, there have been increasing reports of the use of hybrid rooms with advanced imaging equipment for endoscopic kidney stone treatments. 15 –19 This report describes CO2-P, including our preferred digital subtraction (CO2 digital subtraction pyelography [CO2-DSP]) technique, as part of our efforts to improve the quality of imaging and radiation during endoscopic stone treatments.
Materials and Methods
An institutional review board (IRB)-sanctioned quality improvement (QI) initiative for endoscopic stone surgery in a hybrid room was initiated in July 2021 at our VA facility. Advanced pyelography (using ICM or CO2 contrast) was to be optimized for image quality and radiation doses. A retrospective analysis of cases using CO2-P after the intervention began was performed and comparisons were made with preintervention endoscopic stone treatment cases using CO2-DSP; cases treated with CO2-P using a traditional fluoroscopy system (TFS) due to the inability to schedule a hybrid room after the intervention; and cases undergoing ureteroscopy (URS), with stone treatment performed using a TFS in the three calendar months before the intervention (March–June 2021).
A robotic arm multiplanar fluoroscopy system (RMPFS) (Artis Zeego Care+Clear; Siemens Medical Solutions, Melvern, PA) was used in a hybrid room, or TFS (Veradius Unity, Philips Healthcare, Andover, MA) was used otherwise. The CO2-DSP technique was similar to a published description for CO2-DSA, 20 using endovascular pulsed fluoroscopy CO2-DSA settings to visualize the collecting system. After aspirating urine from the renal pelvis, brief apnea was induced, and CO2 was injected for 0.5 to 1 second after initiating pulsed fluoroscopy.
A 20-mL high-pressure syringe (Monoject™; Cardinal Health, Dublin, OH) was filled with CO2, emptied to avoid air contamination, refilled with 15 to 20 mL of CO2, and then injected. To prevent direct flow of gas, two high-capacity Marquis® stopcocks (Merit Medical, South Jordan, UT) were serially connected between the conduit to the upper tract (e.g., catheter) and arterial pressure tubing (ICU Medical, San Clemente, CA) from the CO2 source (Fig. 1). Endoscopy then proceeded in standard manner using saline irrigation.
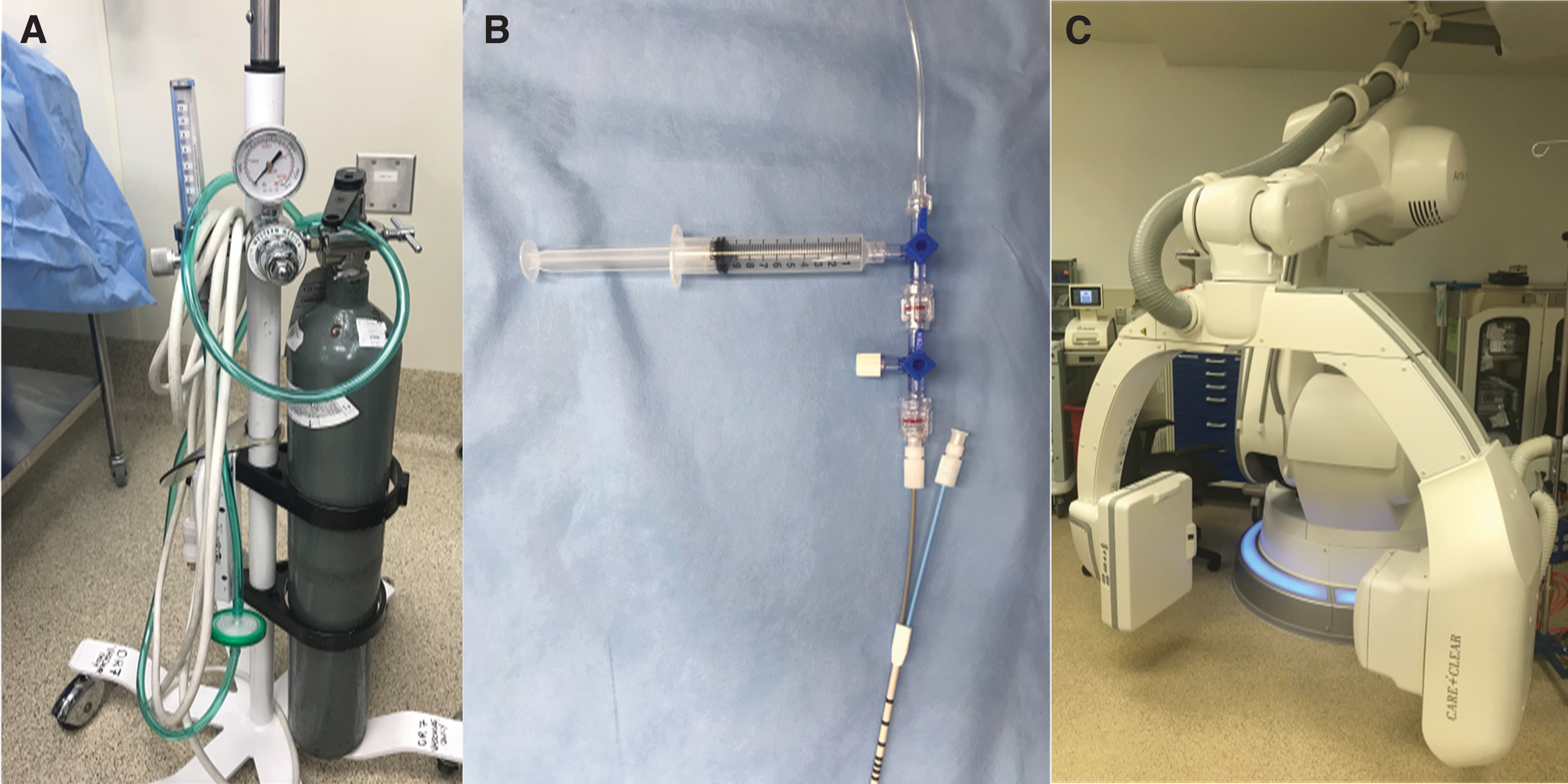
External equipment.
CO2-P was subjectively assessed by the surgeon from native images obtained with CO2-DSP or performed separately with spot images using a Likert scale (5 = outstanding; 4 = excellent; 3 = very good; 2 = good; 1 = marginal; and 0 = poor). The effective radiation dose (ERD) was estimated using Monte Carlo simulation techniques with National Cancer Institute dosimetry system for Radiography and Fluoroscopy (NCIRF) software. 21
Statistical analyses, for example, the Kruskal–Wallis rank sum test, were performed using R/RStudio (4.0.3). 22,23
IRB protocol: COMIRB 21-3896
The Colorado Multi-Institutional IRB (COMIRB) reviewed our protocol for a QI project intended to optimize imaging techniques (specifically including CO2-P and intraoperative CT [ICT] imaging), reduce the radiation dose, and decrease the rate of second-stage surgeries. (COMIRB 21-3896). They determined that this project qualified as QI rather than human research. Therefore, additional patient consent was not required.
Publications related to the project were authorized by the IRB. Findings may not be generalizable to other patients and facilities.
Results
Between March 2021 and August 2022, CO2-P was performed in 22 endoscopic stone treatment cases, including digital subtraction (CO2-DSP) in 20 cases. Three CO2-DSP imaging cases (RMPFS = 1 and TFS = 2) preceded the hybrid room QI intervention. Seventeen cases (RMPFS = 8 and TFS = 9) occurred after an international contrast shortage (ICS) 9 prompted facility ICM conservation measures. TFS cases involved smaller stones (7–15 mm) without planned ICT (Fig. 2).
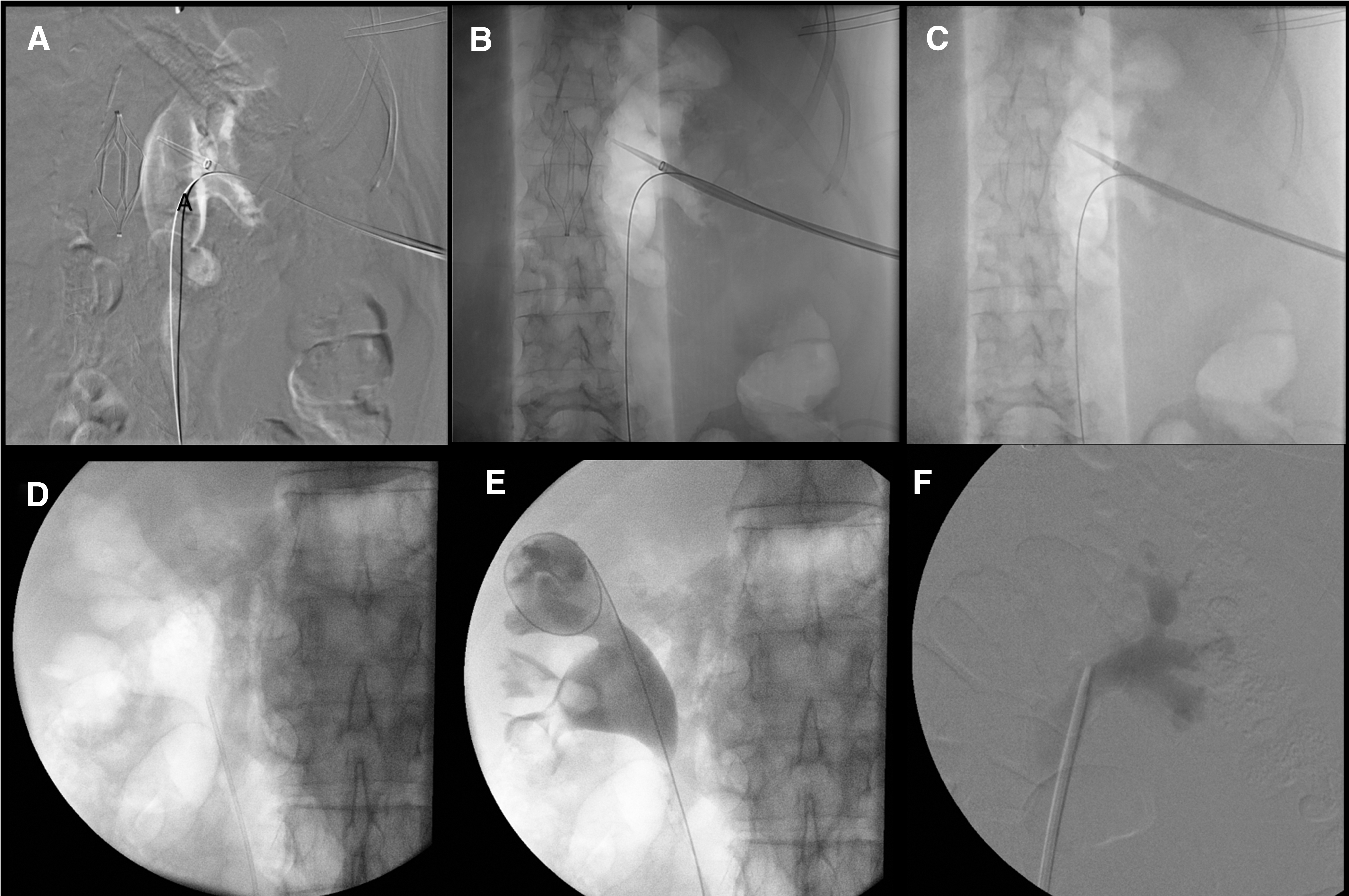
Intraoperative imaging before the QI intervention. Note prominence of the IVC filter medial to the renal pelvis with DSA settings
Primarily, ultrasound-guided access was used in all three percutaneous surgeries (Table 1). A retrospective TFS cohort comprising 22 URS cases without the CO2 contrast was also identified for dose comparison, with ICM pyelography performed in 17 (77%) cases (Table 2). An effective outcome was a significant reduction in fluoroscopic radiation dose after the intervention, while maintaining sufficient image quality to clearly distinguish the collecting system using CO2 (Fig. 3).
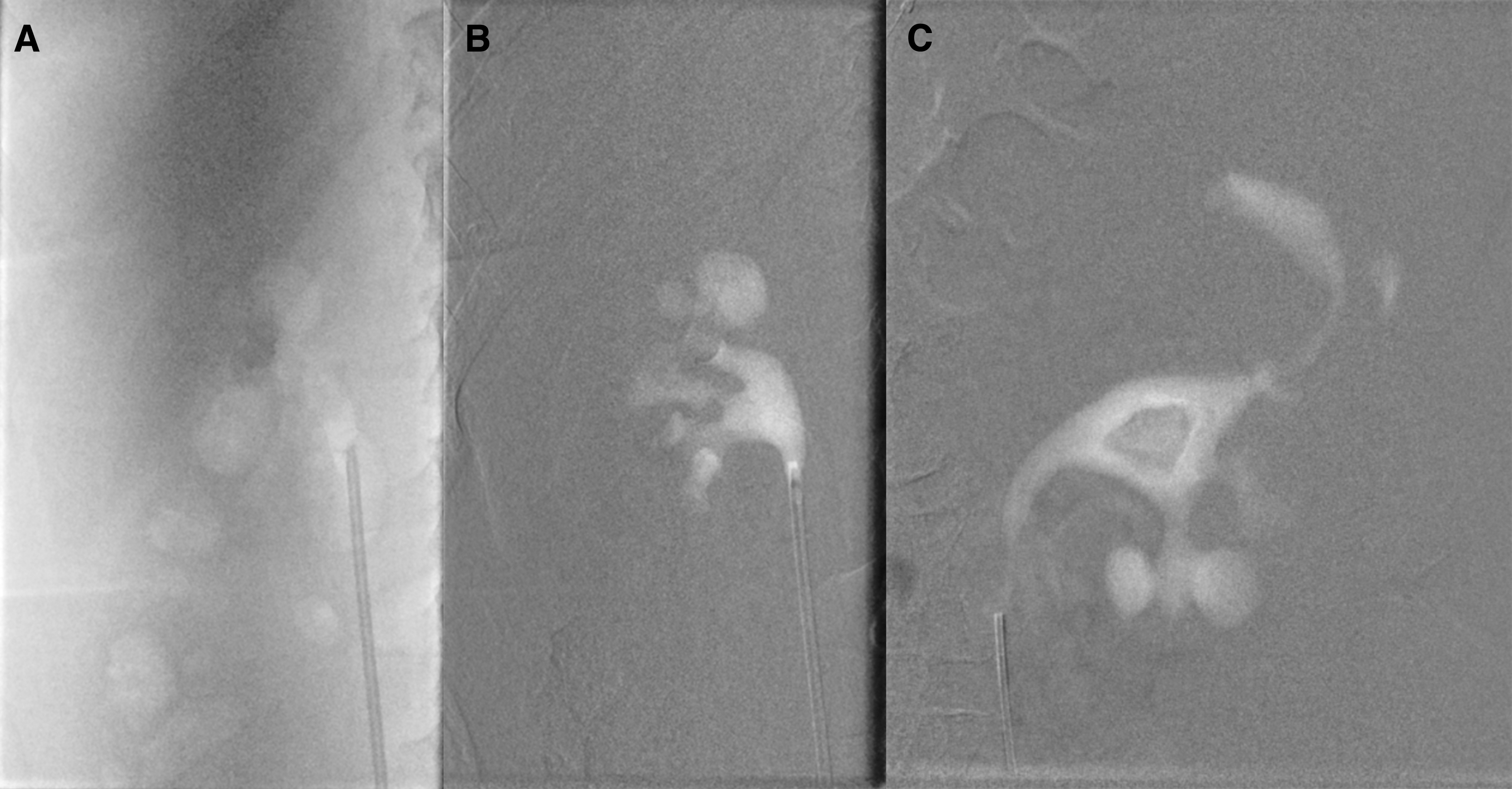
Reduced-dose RMPFS CO2-DSP imaging protocols after QI intervention.
Endoscopic Stone Treatment Cases Using Carbon Dioxide Contrast
BMI = body mass index; CA = contrast allergy; CO2 = carbon dioxide; CO2-DSP = CO2 digital subtraction pyelography; CO2-P = CO2 pyelography; cysto = cystourethroscopy; DAP; DSA = digital subtraction-enhanced angiography; ECIRS; ERD = effective radiation dose; ICM = iodinated contrast medium; ICS = international contrast shortage; ICT = intraoperative CT; LL = laser lithotripsy; NA; NS; PCNL = percutaneous nephrolithotomy; PT; RMPFS = robotic arm multiplanar fluoroscopy system; TFS = traditional fluoroscopy system; URS = ureteroscopy.
Preintervention Ureteroscopy Cases Without Carbon Dioxide Contrast
Adequate imaging of the renal pelvis and calices was achieved in all fluoroscopy cases using CO2. The gas typically dissipated rapidly (<1 minute) and did not negatively impact endoscopy or ultrasound imaging. CO2-P provided a two-dimensional image with the system appearing white. Compared with either ICM pyelography or CO2-DSP, it was generally more difficult to distinguish CO2 in the collecting system from gastrointestinal-related gas.
Relative to TFS, RMPFS has more robust image stacking capabilities, and CO2-DSP provided an enhanced three-dimensional appearance of the collecting system. Additionally, RMPFS automatically applied postimage processing (Artis syngo iFlow®) to generate colorized composite images indicating the time for contrast opacification of a given location (Fig. 4). In a single RMPFS case (case 1), in which we attempted to use CO2 as a negative contrast agent to enhance stone identification for ICT, the gas dissipated too quickly to be useful.

Artis syngo iFlow™ reconstructed images demonstrate the time for contrast filling of a given location in seconds.
Using the RMPFS, CO2-DSP was rated 5 (outstanding) in two imaging studies of the preintervention case and subsequently 4.5 (range: 1–5) in eight imaging studies (seven cases) with proper technique. By comparison, CO2-P images were rated 4 (excellent) for two preintervention cases and 3 (very good) overall (range: 0–4) in nine postintervention studies (eight cases). CO2-P imaging could not be evaluated for two cases because the CO2-DSP native images were not separately archived.
TFS CO2-DSP was rated as 4 in both the two cases before the intervention and eight cases after the intervention (3–4), with one case limited by poor technique. However, TFS CO2-P was typically only rated 1 (marginal) overall (0–4) in seven assessable studies after the intervention. Overlying bowel gas and stacking effects typically explained the rating differences between the two techniques. Mild extravasation was noted in two cases with rapid injection, but gas dissipated quickly without injury, observed endoscopically.
The median ERD for all fluoroscopy procedures was 1.73 mSv (0.68–37.4) in the initial three CO2-DSP cases. The highest dose operation was the initial RMPFS mini-PCNL case, involving two extended runs (29 seconds) using standard endovascular CO2-DSA settings. After the QI intervention, the fluoroscopy ERD in CO2-DSP cases was reduced by 81% to 0.33 mSv (p = 0.02) by consistently using low-dose digital subtraction settings with short runs (≤3 seconds). In the six most recent RMPFS cases, the even flow low-dose DSA protocol (6–10 frames/sec) was used with collimation to further reduce the dose. In the two RMPFS cases using low-dose CO2-P before ICT, the fluoroscopy ERD was even lower (0.075 mSv).
The ERD was 0.21 mSv in TFS cases using low-dose CO2-DSA settings (4 frames/sec), almost identical to the historical URS group without CO2 contrast (0.20 mSv) (Table 2). The fluoroscopy ERD was higher at 0.51 mSv for RMPFS CO2-DSP cases. However, confounding factors include much larger stone burdens (33.5 vs 9 mm, p < 0.001) and higher pulse rates (6–10 vs 4 frames/sec).
Paradoxically, fluoroscopy times were significantly lower with RMPFS than TFS (0.1 vs 0.5 minutes, p < 0.001). However, even in the retrospective URS group, the correlation between radiation dose and fluoroscopy time was low (r = 0.15).
Discussion
The first description of the CO2-P technique since endourology's infancy is presented. CO2 is safer than RA within the vasculature due to blood solubility that is 54 times greater than nitrogen and 28-fold greater than oxygen. 20 Venous air embolism (VAE) is a potentially fatal risk factor for patients undergoing PCNL, with two documented deaths, although neither involved RA pyelography. 24,25 However, most cases of VAE occurring with PCNL have been associated with the imaging study, with one near fatality reported in 1997. 3
In a review of 30,666 PCNL procedures, Basiri et al. identified 11 serious neurologic events, including four cases of paraplegia, all in cases involving the RA contrast. 5 Despite difficulty in performing timely imaging, at least two cases had echocardiogram-confirmed gas within the cardiac chambers after RA pyelography. 7,26
CO2 contrast was previously reported for percutaneous renal surgeries, including a clinical trial involving 32 patients at the University of Minnesota. 10,11 Similar to our series, two cases had extravasation into the soft tissues, which rapidly diffused away without adverse effects. Because it dissipates quickly, CO2 does not impact ultrasound imaging during renal access.
The only other urologic publication advocating the use of CO2 contrast was by Turillazzi et al. who experienced a VAE-related death with PCNL. Although not actually using RA pyelography in the case or citing examples of CO2-P, they nevertheless strongly advised that urologists use CO2 instead of RA for pyelography. 24
Safety precautions should be considered when working with pressurized CO2 gas. The lowest possible flow rate should be used to fill the syringe; and the syringe piston should be directed in a safe direction with counterpressure maintained, for example, using the thumb. The double-stopcock technique is intended to mitigate the potential for injection of large volumes of CO2 into the patient, while minimizing potential RA contamination. Other surgeons favor CO2 filling of the syringe under water, which also allows advance preparation at the back table before starting. 27
The endovascular surgeon coauthor (J.E.) recommended CO2-DSA settings to perform CO2-P in our initial case, which continues to be our preference. Based on our experience to date, we would suggest injecting 15–20-mL aliquots of CO2 at a slow–moderate rate using pulsed abdominal low-dose DSA settings. Because intensive image processing can cause a slight delay, urologists should take care not to overdistend the system.
Digital subtraction often mitigates intrusive overlying bowel gas and provides higher quality imaging overall, with a tradeoff of a relatively increased radiation dose. However, radiation doses were reduced by four-fifths after the QI intervention. While further study would be required, the RMPFS Artis syngo iFlow postimage processing could improve understanding of individual flow patterns in the kidney and ureter.
The two most common indications for CO2-P in our cases were the intent to avoid ICM artifacts during ICT and limited ICM availability during ICS. ICT to assess residual stone fragments following percutaneous stone treatment has been described by several groups since 2017, 17 –19 and our group is now routinely performing ultralow-dose ICT for treatment of larger stones. 28
Ritter et al. assessed various ICM concentrations in a phantom model and concluded that 20% ICM concentration was optimal to distinguish stones from contrast, which was assessed with ICT in a single patient before PCNL treatment. 15 However, we advocate using CO2 contrast instead of ICM before ICT when feasible.
There are limitations to this report. First, as a QI project, our findings may not be generalizable to patients at other facilities. Second, the assessment of imaging quality is subjective. Third, our comparisons were based on retrospective analyses of patients before and after a quality intervention and there were potentially confounding differences between cohorts.
Conclusions
CO2 is an inexpensive and reasonable alternative to ICM for endoscopic stone surgeries, which effectively eliminates the risk for VAE seen with RA contrast. CO2 pyelography (CO2-P/CO2-DSP) techniques should be preferable to improve safety of percutaneous fluoroscopic access for urologists using RA pyelography during fluoroscopic access. Finally, CO2 avoids contrast artifacts that could be mistaken for stone fragments on fluoroscopy or ICT.
Footnotes
Acknowledgment
The authors would like to thank their endovascular surgical nurse coordinator, Debbie Kreppein, RN, for her significant support in making this project possible.
Authors' Contributions
M.D.S. was involved in conceptualization; methodology; investigation; software; formal analysis (lead); writing—original draft (lead) and revision (lead); visualization; project administration; and supervision. A.H. was involved in investigation and writing—original draft and review of revision. S.D.H was involved in conceptualization (hybrid room PCNL) and writing—review of original draft and revision. D.R.B. was involved in conceptualization (CO2-P) and writing—review of original draft and revision. J.C.E. was involved in conceptualization (CO2-P); methodology; and writing—review and editing of original draft and revision. E.B.L. was involved in methodology; investigation; formal analysis; and writing—original draft and editing of revision.
Author Disclosure Statement
M.D.S. is a consultant/speaker for Laborie/PrimeSight. S.D.H. is Founder/Executive Officer/Shareholder for Virtuoso Surgical and additionally Founder/CMO/Shareholder for EndoTheia, Inc. Siemens has provided technical training and support related to the robotic arm multiplanar fluoroscopy system (RMPFS), including developing customized lower radiation dose CO2 pyelography protocols, but did not attempt to influence the project or manuscript and did not review it before submission.
Funding Information
No external funding was received.