
Abstract
Objective:
To share our experience in robot-assisted pyeloplasty (RAP) with the Kangduo (KD) surgical robot vs the da Vinci Si (DV) robotic system (KD-RAP vs DV-RAP, respectively).
Methods:
From August 2019 to February 2021, 16 patients with ureteropelvic junction obstruction (UPJO) underwent KD-RAP and other 16 patients with UPJO accepted DV-RAP. All procedures were performed by the same surgeon. The perioperative results and follow-up data were prospectively collected and compared.
Results:
There was no conversion to open or laparoscopic surgery. The mean operation time was significantly longer in the KD-RAP group than the DV-RAP group (141 ± 28 minutes vs 118 ± 31 minutes, respectively, p = 0.04). The time per stitch was significantly longer in the KD-RAP group than the DV-RAP group (1.7 ± 0.5 minutes vs 1.4 ± 0.3 minutes, respectively, p = 0.05). No significant difference was noted in the estimated blood loss and the postoperative length of hospitalization. At a median follow-up of 19 (range 17–21) and 19.5 (range 14–33) months for the KD-RAP and DV-RAP groups, respectively, no difference was noted in the success rates between the KD-RAP and DV-RAP groups (93.75% and 100%, respectively; p = 0.31). Complications were comparable between the two groups (p = 0.54). One (6.3%) patient developed urinary infection, which responded well to oral antibiotics in KD-RAP group and 2 (12.5%) patients suffered from irritation symptoms of bladder, which improved after removal of Double-J stent in the DV-RAP group.
Conclusions:
The RAP with the use of the KD system was feasible, safe, and effective. The DV-RAP group showed advantage in the operation time and the time per stitch.
Introduction
Ureteropelvic junction obstruction (UPJO) is characterized by inhibited urine flow from the kidney to the upper ureter due to a variety of causes. Open Anderson–Hynes dismembered pyeloplasty is considered a technique of choice for long-term excellent success rates for complete resection of the obstructed segment with reanastomosis of the renal pelvis and ureter in a funneled fashion. 1,2 Previous studies have reported that the success rate of laparoscopic pyeloplasty (LP) was comparable to that of open pyeloplasty, although the advantages of LP include decreased morbidity, shorter hospital stay, and quicker recovery. 3 –5 However, LP is accompanied with a steep learning curve due to technically demanding and time-consuming intracorporal suturing, which has limited widespread use.
Robot-assisted LP and conventional LP appear to be equivalent regarding success rates, postoperative urinary leaks, hospital readmissions, and operation time, 6 whereas robotic surgery is advantageous in terms of objective and subjective ergonomics. 7,8 Robotic devices have been recently developed by various manufacturers. 9,10 In China, a new robotic platform, called the Kangduo (KD) surgical robot, was developed by SuZhou KangDuo Robot Co., Ltd. (Suzhou, China). We previously reported the initial application of the KD system for robot-assisted pyeloplasty (RAP) and prolonged follow-up was required to evaluate its efficacy. 11 Furthermore, no study has yet compared the use of KD surgical robot and the da Vinci Si (DV) robotic system in RAP. To the best of our knowledge, this is the first study to compare the outcomes of KD-RAP vs DV-RAP.
Materials and Methods
Patient selection
From August 2019 to February 2021, 16 patients with UPJO underwent KD-RAP and other 16 patients with UPJO accepted DV-RAP. Patient data were prospectively collected in our Reconstruction of the Urinary Tract: Technology, Epidemiology, and Result (RECUTTER) database. The study protocol was approved by the Ethics Committee of Peking University First Hospital (Beijing, China) and all participants were informed of the potential risks before surgery.
The inclusion criteria were (1) UPJO requiring pyeloplasty, (2) age between 18 and 75 years, and (3) signed informed consent. The exclusion criteria included (1) history of abdominal surgery or pyeloplasty, (2) concomitant uncontrolled urinary tract infection, (3) coagulation dysfunction, (4) pregnancy or lactation, (5) relatively high surgical risk or inability to tolerate surgery, and (6) inability or reluctance to cooperate during follow-up.
System introduction
The KD system is a master-slave system consisting of a surgeon console, patient side cart, and vision cart (Fig. 1). According to the three-dimensional image from the vision cart, the surgeon can make surgical decisions with the use of the surgeon console and the surgical instruments of the patient cart simulate and reproduce the surgical procedure.
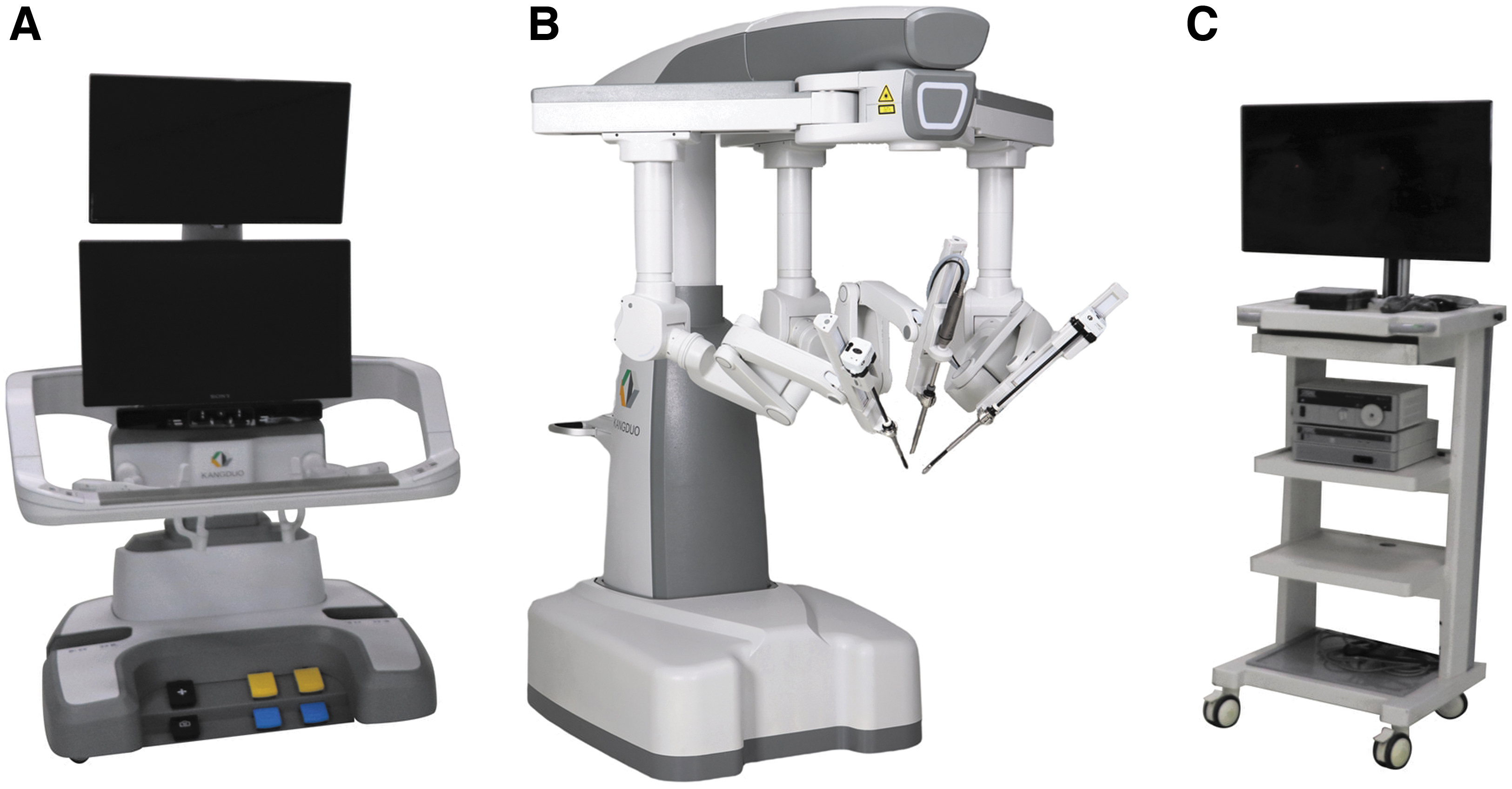
KD robotic system.
Surgical procedures
All patients underwent transperitoneal Anderson–Hynes dismembered pyeloplasty 12,13 by the same surgeon who had performed more than 100 robotic surgeries. The pyeloplasty procedures were similar between the KD-RAP and DV-RAP groups. All procedures were conducted through a transperitoneal approach. The patients were placed in the 45° lateral decubitus position. Three trocars (two operative trocars and one camera trocar) were used for KD-RAP, whereas four trocars (three operative trocars and one camera trocar) were used for DV-RAP. In addition, two assistant trocars were used for suction, retraction, and retrieving sutures with both systems.
After identification of the ureteropelvic junction (UPJ) (Figs. 2A and 3A), an oblique incision was made to the lower pole of the pelvis above the stricture site of the UPJ (Figs. 2B and 3B). Then, the first suture was placed between the ureter and the lowest corner of the renal pelvis, and an anastomosis was performed with the use of running sutures from the point of the first suture after clipping the connection between the UPJ and renal pelvis (Figs. 2C and 3C). Afterward, a 7F Double-J stent was inserted into the distal ureter (Figs. 2D and 3D), the strictured segment of the UPJ was removed, and the redundant renal pelvis was sheared, whereas the margin was continuously sutured to complete the dismembered pyeloplasty (Figs. 2E, F and 3E, F). For UPJO concomitant with renal calculi, intraoperative ureteroscopy was used to extract the calculi.
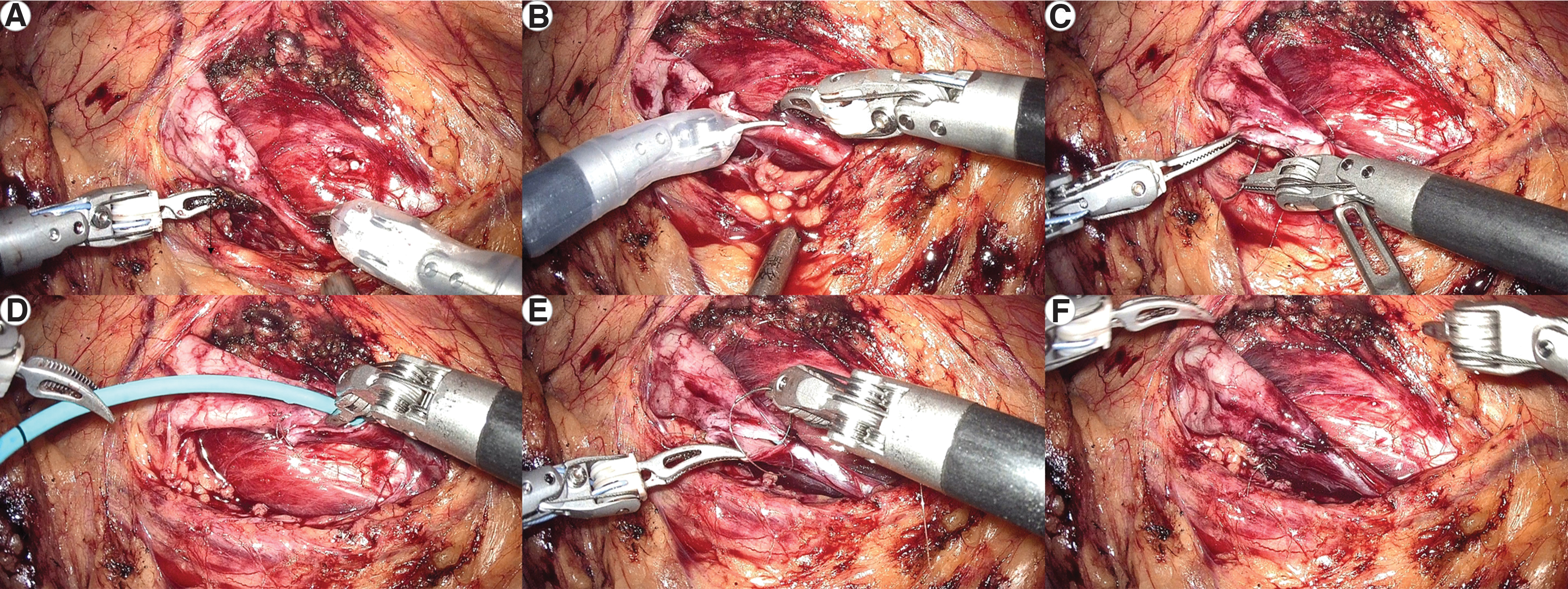
Pyeloplasty using the KD system.
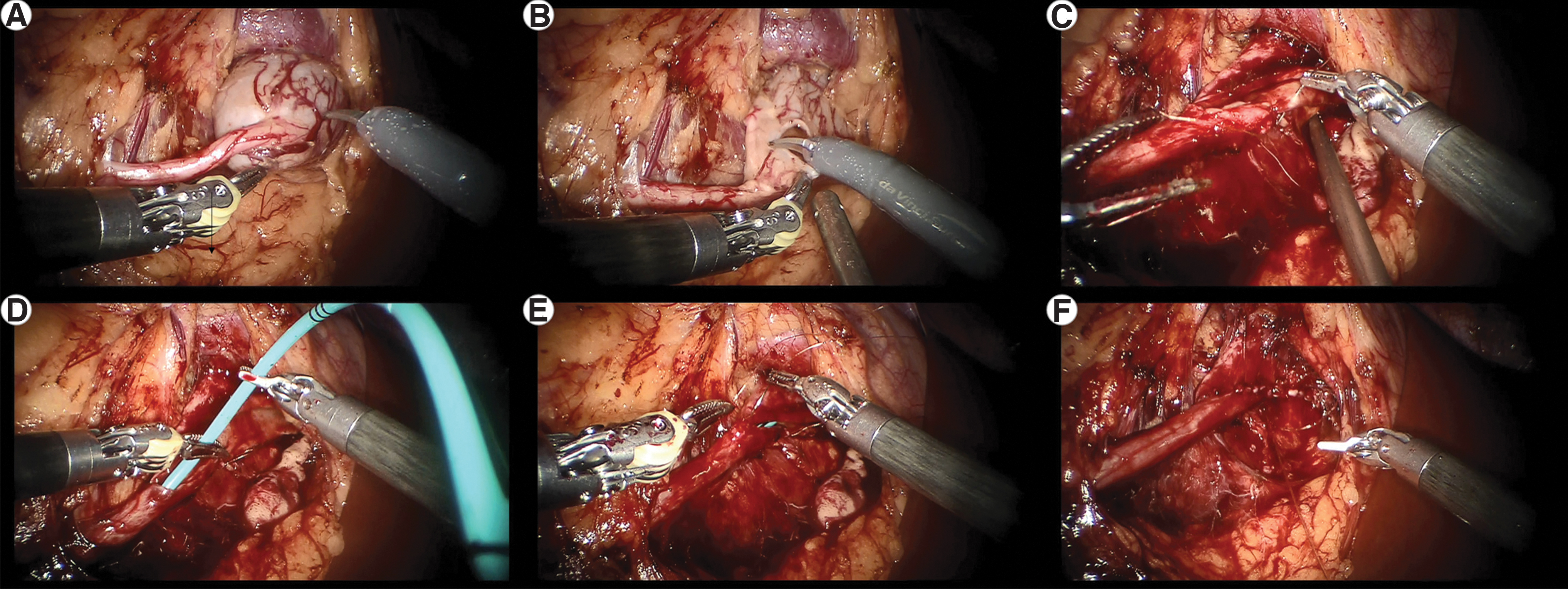
Pyeloplasty using the DV system.
Data collection and statistical analyses
Perioperative results and follow-up data were prospectively collected and compared. The demographics, radiographic data, intraoperative details, and surgical outcomes were obtained prospectively. Imaging examinations consisted of urological ultrasonography, diuretic renography, computerized tomography urography, three-dimensional reconstruction, and so on. Intraoperative details included the total operation time, estimated blood loss, perioperative complications, and conversion rate. The operation time was calculated from the time of the skin incision for the first port to suturing of the last port, and the time for extracting the renal calculi was removed from the operation time. The suturing time was calculated as the total time required for suturing of the UPJ.
All patients were closely monitored and all ureter stents were removed at 2 to 3 months after the surgery. The Clavien–Dindo classification system was used to grade all intraoperative and postoperative complications. 12 Complete success was defined as resolution of both clinical symptoms and obstruction on radiographic evaluation.
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corporation, Armonk, NY). Categorical variables are presented as frequencies and percentages. The Fisher's exact test or χ 2 test was used to compare percentages between the two groups. Quantitative variables were compared with the t-test or nonparametric test and are presented as the mean or median. A two-sided probability (p) value of <0.05 was considered statistically significant.
Results
The characteristics of the two groups of patients are summarized in Table 1. In total, 16 patients (7 males and 9 females; mean age, 31 ± 14 years) underwent KD-RAP and 16 (10 males and 6 females; mean age, 27 ± 10 years) underwent DV-RAP. The mean body mass index (BMI) of patients in the KD-RAP and DV-RAP groups was 23 ± 5 and 22 ± 4 kg/m2, respectively. Overall, 44% (7/16) of patients in the KD-RAP group and 25% (4/16) in the DV-RAP group had right ureteral strictures. In the KD-RAP group, three patients had concomitant renal calculus, one had a horseshoe kidney, and one had a solitary kidney. In the DV-RAP group, one patient had a horseshoe kidney, one had concomitant renal calculus, and two had varicoceles. There were no significant differences in the ratio of males to females, age, BMI, UPJO laterality, and comorbidity between the two groups.
Demographics of the Kangduo Robot-Assisted Pyeloplasty and da Vinci Si Robot-Assisted Pyeloplasty Groups
BMI = body mass index; DV = da Vinci Si; KD = Kangduo; RAP = robot-assisted pyeloplasty; SD = standard deviation.
All procedures were performed successfully without conversion to open or laparoscopic surgery. As shown in Table 2, the mean operation time was significantly longer in the KD-RAP group than the DV-RAP group (141 ± 28 minutes vs 118 ± 31 minutes, respectively, p = 0.04). There was no significant difference in suturing time (46 ± 16 minutes vs 43 ± 14 minutes, respectively, p = 0.62) or the number of stitches (27 ± 9 vs 32 ± 10, respectively, p = 0.23) between the KD-RAP and DV-RAP groups, whereas the time per stitch was significantly longer in the KD-RAP group than the DV-RAP group (1.7 ± 0.5 minutes vs 1.4 ± 0.3 minutes, respectively, p = 0.05). There was no significant difference in the median estimated blood loss between the KD-RAP and DV-RAP groups (8 [range 5–50] vs 10 [range 5–50] mL, respectively, p = 0.11) or the postoperative length of hospitalization (4.3 ± 1.5 days vs 4.2 ± 1.6 days, respectively, p = 0.91). No patient required a blood transfusion.
Operative and Follow-Up Outcomes of the Kangduo Robot-Assisted Pyeloplasty and da Vinci Si Robot-Assisted Pyeloplasty Groups
EBL = estimated blood loss; LOS = length of stay.
At a median follow-up of 19 (range 17–21) and 19.5 (range 14–33) months for the KD-RAP and DV-RAP groups, respectively, no difference was noted in the success rates between the robotic and laparoscopic groups (93.75% vs 100%; p = 0.31). For the one failed case in the KD-RAP group, the patient complained about right flank pain preoperatively and the flank pain reoccurred at a follow-up of 17 months postoperatively. Additionally, the postoperative urinary CT showed no significant relief in hydronephrosis.
Regarding complications, 1 (6.3%) patient developed urinary infection, which responded well to oral antibiotics (Clavien–Dindo grade І) in KD-RAP group and 2 (12.5%) suffered from irritation symptoms of the bladder, which improved after removal of Double-J stent (Clavien–Dindo grade І) (p = 0.54). No severe complications (Clavien–Dindo grade ≥III) were observed.
Discussion
UPJO is defined as restricted urine flow from the renal pelvis to the ureter. If left untreated, UPJO can lead to progressive impairment of renal function. Open surgery has been considered the gold standard for UPJO in adults with success rates exceeding 90% in long-term studies. 1,2,13 –16
Minimally invasive surgery has revolutionized the field of urology. LP for adults was first reported by Schuessler et al. 17 Since then, LP has been confirmed as a minimally invasive intervention with comparable success rates to open surgery. 5,18 Furthermore, LP offers the advantages of decreased postoperative pain, shorter length of hospitalization, and reduced postoperative recovery time. 4,18
However, LP is associated with several disadvantages, including relatively limited motion of the laparoscopic instrumentation through fixed entrance sites, unfamiliar hand–eye coordination, and poor ergonomic position, whereas intracorporeal suturing is especially problematic because it is technically challenging for the surgeon and leads to an extended learning curve. 19
The DV system (Intuitive Surgical, Mountain View, CA), which was developed to overcome the difficulties associated with conventional laparoscopic surgery, 20 translates the hand movements of the surgeon through a console to robotically manipulate the instruments in the operating field. The three-dimensional view of the operative field with 10-fold magnification and the seven degrees of freedom of the EndoWrist® instrument is ideal for precise manipulations required for intracorporeal suturing. 21,22 For patients with UPJO, RAP appears to achieve comparable perioperative results to LP, although RAP can decrease the suturing time and hospital stay. 23 In addition, the learning curve associated with intracorporeal laparoscopic suturing is shorter with a robotic system than conventional laparoscopy. 24
To date, various competing products have been developed, including the TELELAP ALF-X surgical system (SOFAR S.p.A., ALF-X Surgical Robotics Department, Trezzano Rosa, Milan, Italy) and the Revo-i® robotic platform (Meere Company, Inc., Hwaseong, South Korea). Both robotic platforms are master–slave systems that allow the surgeon to control the console and operate the patient cart with instruments. Notably, the TELELAP ALF-X surgical system, which features an eye-tracking camera control system, haptic feedback, and total arm independency, has been confirmed as both feasible and safe for gynecologic procedures 25,26 and has been successfully applied for partial nephrectomy with the use of a pig model. 9 The Revo-i robotic platform is reportedly safe and useful for partial nephrectomy with the use of a pig model. 10
The KD system developed in China was confirmed as both technically feasible and safe for partial nephrectomy with the use of a pig model. 27 Furthermore, the KD system is comparable to other systems from an operative perspective, but with advantages from an ergonomic perspective as compared with laparoscopic surgery. 27 Our initial experience supported the feasibility and safety of the KD system for RAP. 11 This is the first prospective clinical study to compare outcomes of KD-RAP vs DV-RAP.
In this study, all surgeries were completed and no case required conversion to either open or standard laparoscopic surgery, which indicated its feasibility. The conversion rate of both the KD-RAP and DV-RAP groups was not inferior to that in a previous report. 6 Both groups had a success more than 90% and no significant difference was noted in success rate between the two groups, which illustrated effectiveness of KD-RAP. With regard to safety, there were no severe perioperative complications (Clavien–Dindo grade ≥III) or equipment-related adverse events, similar to a previous study. 6
Although there were no significant differences in suturing time, the total number of stitches per ureter, and estimated blood loss, both the operation time and the time per stitch were significantly longer in the KD-RAP group than the DV-RAP group. There are several possible reasons for the longer operation time and the longer time per stitch. First, the DV system has four arms, including three instrument arms and one camera arm, whereas the KD system has three arms, including two instrument arms and one camera arm. The additional arm of the DV system provides an optimal visual operative field to simplify suturing. Second, the surgeon had performed more than 100 robotic surgeries with the DV system, while experience with the KD system was relatively limited. Although the longer time per stitch is a disadvantage, the KD system is an alternative for minimally invasive surgery.
The postoperative hospitalization stay was comparable between the two groups, but slightly longer than reported in a previous study, 6 which might be related to nonmedical sociodemographic and economic factors.
Both the KD and DV systems are master–slave systems. As compared with the DV system, the main difference lies in the open surgeon console, which relieves neck fatigue, and the suspended surgical arm to facilitate position adjustment. Both systems lack a tactile feedback system, although the three-dimensional screen of the working field of the surgical console allows precise tissue identification and estimation of the suture tension.
There were some limitations to this study that should be addressed, especially the limited size of the cohorts and the relatively short follow-up period. In addition, randomization was not used to reduce the impact of potential confounding variables. While this was a preliminary study to describe our early experiences, the strength of this study is the prospective design and the minimal operator variability, as all procedures were performed by the same surgeon. A prospective, randomized trial with prolonged postoperative surveillance is warranted to evaluate the application of this new robotic surgery system.
Conclusions
The RAP with the use of the KD system was feasible, safe, and effective. The DV-RAP group showed advantage in the operation time and the time per stitch.
Footnotes
Authors' Contributions
S.F.: Conceptualization; Formal analysis; Project administration; and Writing—original draft.
S.X.: Data curation; Formal analysis; and Writing—original draft.
Z.L.: Data curation; Investigation; and Project administration.
X.D.: Investigation and Project administration.
J.W.: Data curation and Investigation,
G.H.: Data curation and Investigation.
X.L.: Data curation and Investigation.
S.C.: Data curation and Investigation.
C.Y.: Data curation and Investigation.
C.M.: Data curation and Investigation.
K.Y.: Conceptualization and Writing—review and editing.
L.M.: Conceptualization; Resources; and Writing—review and editing.
X.L.: Conceptualization; Resources; and Writing—review and editing.
L.Z.: Conceptualization and Resources.
Acknowledgments
The authors are grateful to Xiao Zhang and Yue Wu who helped in the preparation of this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the Horizontal Subject of Peking University First Hospital (5001703).