
Abstract
Background:
To study the predictors of sepsis and the progression of sepsis to septic shock in patients after percutaneous nephrolithotomy (PCNL) and to establish and validate predictive models.
Methods:
The patients were assigned to either the development cohort or the validation cohort depending on their hospital. In the development cohort, univariate and multivariate logistic regression analyses were used to screen independent risk factors for sepsis after PCNL and sepsis progression to septic shock. Nomogram prediction models were established according to the related independent risk factors. Areas under the receiver operating characteristic curves, calibration plots, and decision curve analysis (DCA) were used to estimate the discrimination, calibration, and clinical usefulness of the prediction models, respectively. The two sets of models were further validated on the validation cohort.
Results:
In the development cohort, the risk factors for sepsis after PCNL were diabetes, urine nitrite, staghorn calculi, HU value, albumin–globulin ratio, and high-sensitivity C-reactive protein/albumin ratio. The pre- and postoperative white blood cell counts were risk factors for the progression of sepsis to septic shock. The area under the ROC curve value for predicting sepsis risk was 0.891 and that for predicting septic shock risk was 0.981 in the development cohort; in the validation cohort, these values were 0.893 and 0.996, respectively. In the development cohort, the calibration test p values in the sepsis and septic shock cohorts were 0.946 and 0.634, respectively; in the validation cohort, these values were 0.739 and 0.208, respectively. DCA of the model in the sepsis and septic shock cohorts showed threshold probabilities of 10%–90% in the development cohort; in the validation cohort, these values were 10%–90%.
Conclusion:
The individualized nomogram prediction models can help improve the early identification of patients who are at higher risk of developing sepsis after PCNL and the progression of sepsis to septic shock to avoid further damage.
Background
Percutaneous nephrolithotomy (PCNL) is the primary treatment for renal and upper ureteral stones >2 cm. 1 Although PCNL has the advantages of less surgical trauma and high stone clearance efficiency, its postoperative complications also need to be closely monitored. 2 The main postoperative complications of PCNL include postoperative hemorrhage and infection, and infection is the most common complication. 3 However, the probability of infection progressing to severe sepsis or even septic shock after PCNL is low (0.3%–4.7%). 4 When septic shock occurs, the mortality rate of patients can even be up to 50%. 5 Therefore, it is necessary to predict sepsis and septic shock before or early after surgery.
Currently, there is no gold standard for the diagnosis of sepsis. Sepsis is a systemic inflammatory disease caused by the urinary system. The Sepsis-3 Task Force redefined sepsis by the Sequential (Sepsis-related) Organ Failure Assessment (SOFA) score more. 6 However, SOFA is characterized by cumbersome evaluation and poor timeliness and requires a large amount of energy from medical staff. It is not suitable for all PCNL postoperative patients to be evaluated, so it is not able to diagnose sepsis quickly and early. Therefore, quick SOFA (qSOFA) was developed for the early screening of patients at high risk of septic shock. The median time at which the qSOFA score met its cutoff was shorter than that of the SOFA and systemic inflammatory response syndrome scores. 7 Unfortunately, the performance of qSOFA in predicting sepsis onset has been criticized because of the lack of essential high sensitivity. 8 Therefore, it is extremely necessary to effectively predict the occurrence of sepsis before surgery and the progression of sepsis to septic shock within a short period of time after surgery. In the current study, the pre- and postoperative white blood cell (WBC) ratios are instructive for predicting septic shock. 9,10
Some previous studies have summarized the risk factors for sepsis after PCNL. 11 However, most of these studies focused on urinary diseases, such as urinary tract infections, anatomical abnormalities, or stone characteristics. However, the patient's own immune resistance system is also an important factor affecting postoperative infection, for example, tumor patients with low albumin have a higher risk of postoperative infection. 12 In recent studies, the albumin–globulin ratio (AGR) and high-sensitivity C-reactive protein/albumin ratio (hs-CRP/Alb) are effective predictors of postoperative sepsis. 13 –15
All the current prediction models are used to predict postoperative sepsis after PCNL, and no further model has been established to predict the progression of sepsis to septic shock. However, based on the preoperative and postoperative results, this study established a model for predicting sepsis after PCNL and a model for the progression of sepsis to septic shock. When the prediction results suggested that the patient was at high risk of sepsis after PCNL, further examination was conducted in time after surgery to predict the possibility of septic shock according to the pre- and postoperative WBC ratio. The combination of these two prediction models can effectively improve the alertness of medical staff to high-risk patients and reduce the workload of medical staff to a certain extent.
Methods
Participants
A total of 1472 adult patients with PCNL were selected for the study. A total of 1045 patients were recruited from the First Hospital of Hebei Medical University, 427 patients were recruited from the Liaocheng People's Hospital from June 2016 to October 2021, and their complete datasets were retrospectively analyzed. The inclusion criteria included the following: (1) patients who were older than 18 years of age; (2) patients who underwent PCNL surgery in our hospital and were followed up; and (3) patients with complete clinical data. The exclusion criteria were as follows: (1) patients with stage 2 or higher PCNL; (2) patients with horseshoe kidney who underwent repeat kidney surgeries and who underwent renal transplantation; and (3) patients on immunosuppressive drugs.
The patient assessments included a physical examination, medical history, and routine preoperative examination. All patients underwent a preoperative CT examination of the urinary tract to determine the position and size of the calculi to help determine the puncture route. Patients without preoperative urinary tract infection were routinely treated with a dose of cefuroxime 30 minutes before the induction of anesthesia and after surgery. Patients with urine nitrite or WBC positivity received antibiotics before surgery until urine reexamination results were normal (urine nitrite normal and urine white blood significant decrease). Sepsis patients were treated with antibiotics according to the results of bacterial culture and drug sensitivity after surgery until routine blood tests, routine urine nitrite tests, urine bacterial culture, and CRP levels were normal.
PCNL procedures
All patients underwent PCNL in the Department of Urology of our hospital. After general anesthesia was administered, a patient was placed in the lithotomy position, and the surgical area was routinely disinfected. A transurethral ureteroscope was placed, along with an indwelling ureteral catheter, which was connected with saline to create artificial hydronephrosis. The ureteral catheter was attached to a three-cavity catheter.
The patient was placed in the prone position with the waist propped up. Under the guidance of B-ultrasound, the renal pelvis was punctured with a 17.5-gauge puncture needle. After clear urine was observed in the puncture needle, a guide wire was placed, and fascial dilators of 10F, 12F, 14F, 16F, and 18F were used to gradually expand the puncture channel along the guide wire. An 8/9.8F ureteroscope was inserted along the sheath to identify the calculi. If the stone volume was large, the puncture channel was expanded to 24F. A 0.9% NaCl infusion was applied at a flow rate of 200–300 mL/min during the operation, and holmium YAG laser or ultrasound lithotripsy was performed. Fragments of the stones were extracted or flushed out. When no significant bleeding or residual stones were detected, the ureteral catheter was withdrawn, a 6F Double-J tube was inserted through the nephrostomy, and a 14F nephrostomy tube was indwelled. If sepsis did not appear postoperatively, the nephrostomy tube was routinely removed 2–4 days after surgery. If the patient developed sepsis after surgery, the nephrostomy tube was not removed until the patient's infection was under control.
Routine blood examination was performed 2 hours after the surgery. Heart rate, blood pressure, respiratory rate, body temperature, and the Glasgow Coma Scale were measured 2 hours after the operation. Stone fragments obtained during the operation were analyzed to determine stone composition, and the results were obtained within 1–2 days postoperatively.
Definition of sepsis and septic shock
Sepsis is defined as a life-threatening organ dysfunction caused by a dysregulated host response to infection. For clinical operationalization, organ dysfunction can be represented by an increase in the SOFA score of 2 points or more. 6
Septic shock was defined as the need for vasopressors to maintain a mean arterial blood pressure >65 mmHg and a suspected urinary tract infection. 6 The observed hypotension could not have any other possible causes, for example, anesthesia-related hypotension. If these criteria were met, the patients were considered “septic shock patients.” Otherwise, the patients were considered to be “normal patients.”
Statistical analyses
SPSS 24.0 and R software 3.6.3 were used for all statistical analyses. Student's t test or the Mann–Whitney U test was used to detect differences between continuous variables. The chi-square test or Fisher's exact test was used to compare categorical variables. The initial cutoff value based on the Youden index of the receiver operating characteristic (ROC) curves showed the highest sensitivity and specificity. Univariate and multivariate regression analyses were used to determine independent risk factors for sepsis and septic shock development. The regression coefficients were then proportionally converted to 0–100 subscales to generate the predictive nomogram. The predictive performance of the nomogram was measured by its calibration, discrimination, and clinical usefulness. 16 The Hosmer–Lemeshow (HL) test was used, and when the result was insignificant, the correction effect was good. The clinical usefulness of the nomogram was evaluated by decision curve analysis (DCA) by assessing the net benefit at different threshold probabilities. The discriminative performance was assessed by the area under the ROC curve (AUC). A p-value <0.05 was considered significant.
Results
In the development cohort, the medical records of 1045 patients who underwent PCNL were retrospectively collected and analyzed. Of the 1045 PCNL patients, 86 patients had sepsis, and 24 of the sepsis patients developed septic shock. The demographic characteristics and clinical information of the normal patients, sepsis patients, and septic shock patients are presented in Tables 1 and 2. There were significant differences in sex, diabetes status, HU of hydronephrosis, AGR, hs-CRP/Alb ratio, staghorn calculi, urinary WBC counts, urinary nitrite levels, urinary culture results, stone composition, and pre- and postoperative WBC ratio between PCNL patients with and without sepsis. There was a significant difference in the pre- and postoperative WBC ratio between sepsis patients with and without septic shock.
The Demographic Characteristics and Clinical Information of the Normal Patients and Sepsis Patients
AGR = albumin–globulin ratio; BMI = body mass index; hs-CRP/Alb = high-sensitivity C-reactive protein/albumin ratio; SD = standard deviation; WBC = white blood cell.
The Demographic Characteristics and Clinical Information of the Sepsis Patients and Septic Shock Patients
A collinearity diagnosis was made with the above impact factors, and the variance inflation factors of the above independent risk factors indicated that there was no multicollinearity. Since this prediction model was a preoperative prediction model, postoperative predictors were excluded, and multivariate analysis indicated that diabetes, HU of hydronephrosis >6.0, AGR <1.705, hs-CRP/Alb >0.065, staghorn calculi, and urinary nitrite positivity were independent risk factors for the development of sepsis after PCNL. The results are shown in Table 3. Multivariate analyses indicated that the pre- and postoperative WBC ratios were different between sepsis patients with and without septic shock (p < 0.05, Table 4).
Multivariate Logistic Regression of Predictors for Postoperative Urosepsis After Percutaneous Nephrolithotomy
CI = confidence interval; OR = odds ratio; SE = standard error.
Univariate and Multivariate Logistic Regression of Predictors for Septic Shock from Urosepsis Patients
Based on these factors, we established two individualized nomograms to predict sepsis after PCNL and the progression of sepsis to septic shock (Fig. 1). From the nomograms, we calculated the score for each risk factor separately and added all the scores together to obtain the total score. The probability corresponding to the total score is the probability of developing sepsis after PCNL and the progression of sepsis to septic shock.
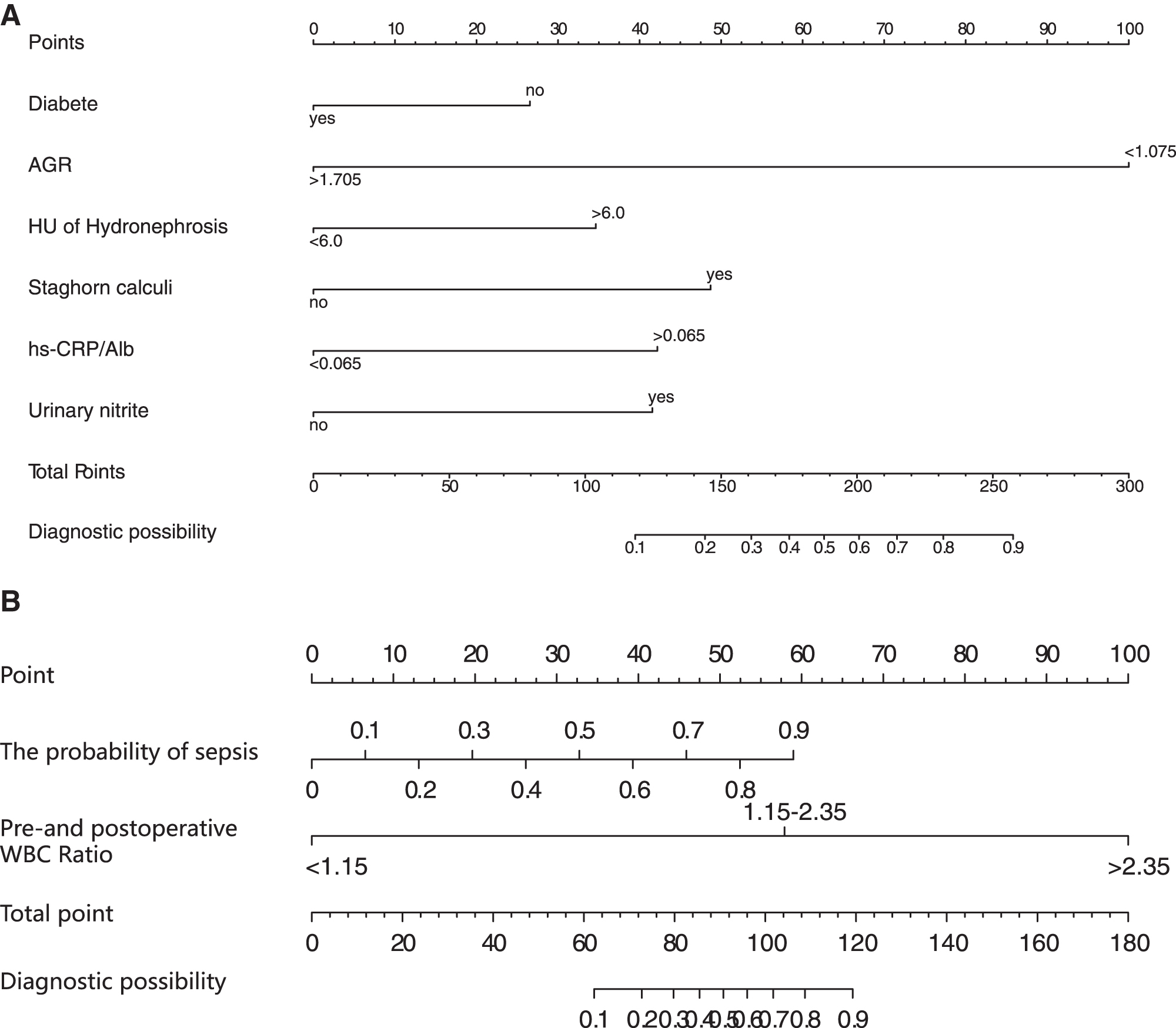
Nomograms to predict urosepsis after PCNL
We validated the identification, calibration, and clinical usefulness of the models in the development cohort and the validation cohort through area estimation under the subject operating characteristic curve, calibration diagram, and DCA, respectively. In the development cohort, the AUC value of the ROC curves for predicting sepsis risk was 0.891, and that for predicting septic shock risk was 0.981, in the validation cohort, which of the two different prediction models were 0.893 and 0.996, suggesting that the nomogram has good discriminative ability (Fig. 2). In the development cohort, the p values of the calibration test in the sepsis cohort and septic shock cohort were 0.946 and 0.634, respectively, and in the validation cohort, were 0.739 and 0.208, which showed good fitting of the model with no statistical significance in the HL test (Fig. 3). DCA of the model in the sepsis cohort and septic shock cohort showed threshold probabilities of 10%–90% in the development cohort and 10%–90% in the validation cohort (Fig. 4). The predictive model was able to identify patients at risk of developing sepsis after PCNL and the progression of sepsis to septic shock.
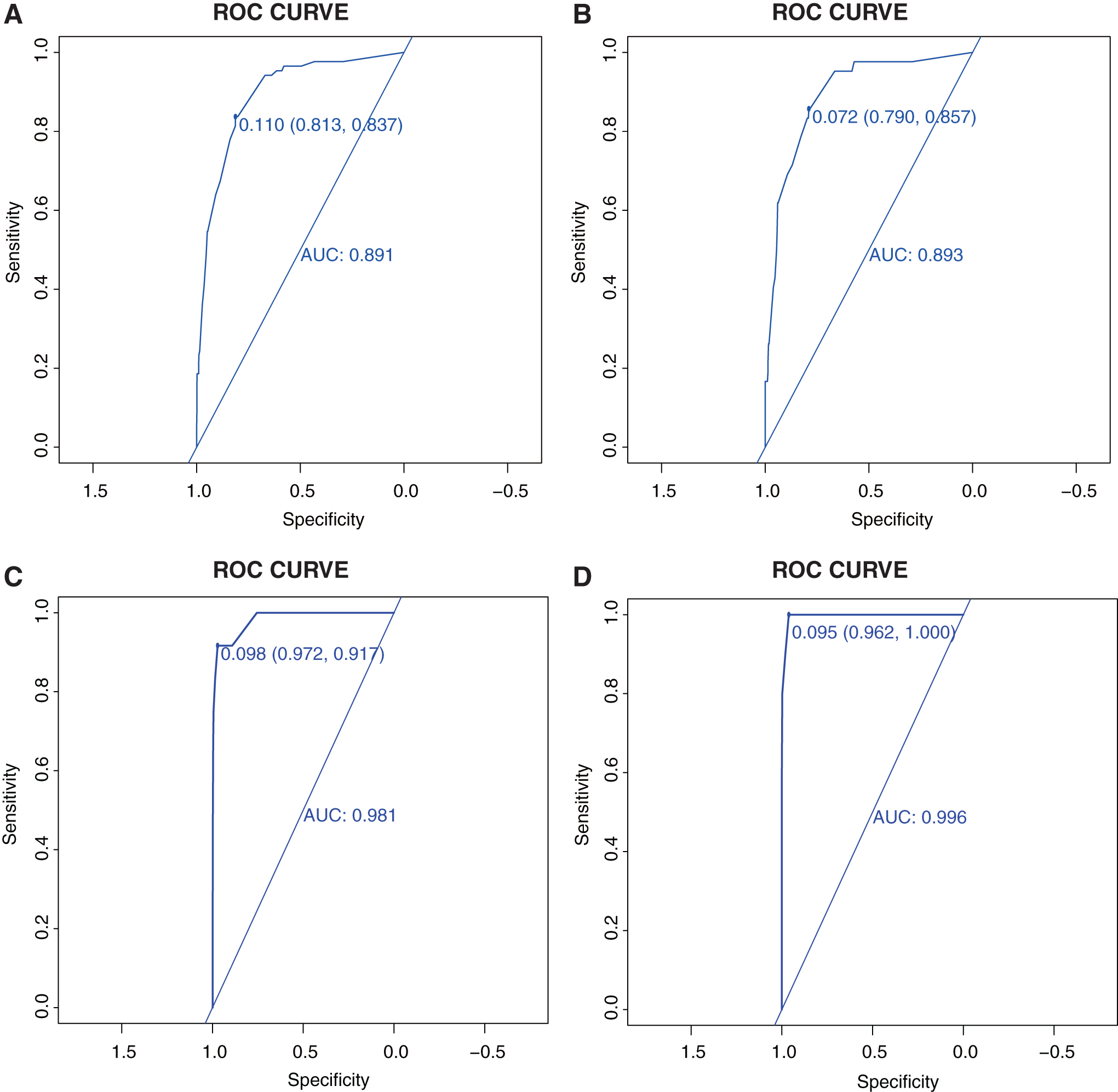
ROC curves for validating the discrimination power of the nomograms.
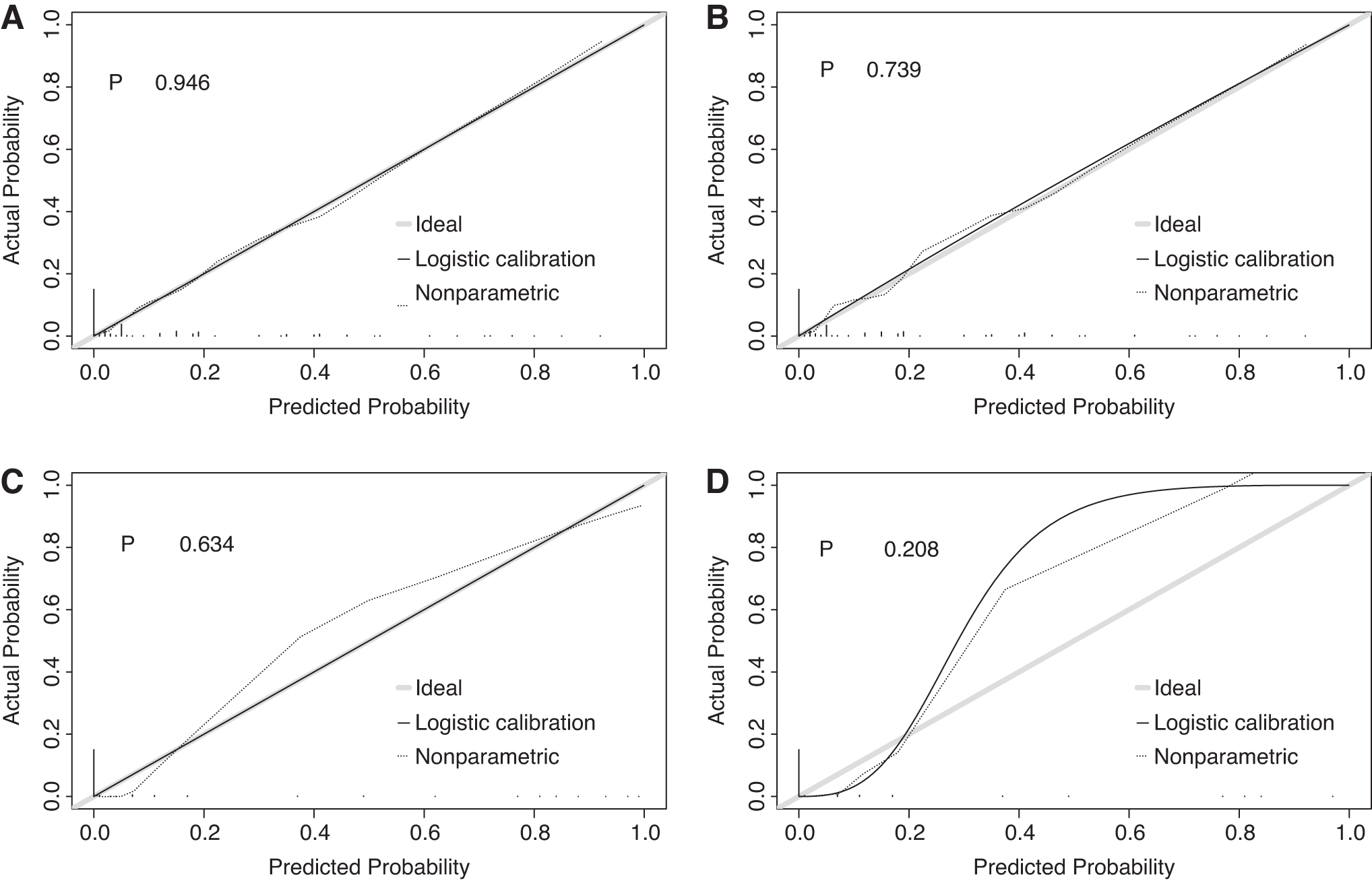
Calibration plot for assessing internal calibration of the nomograms.
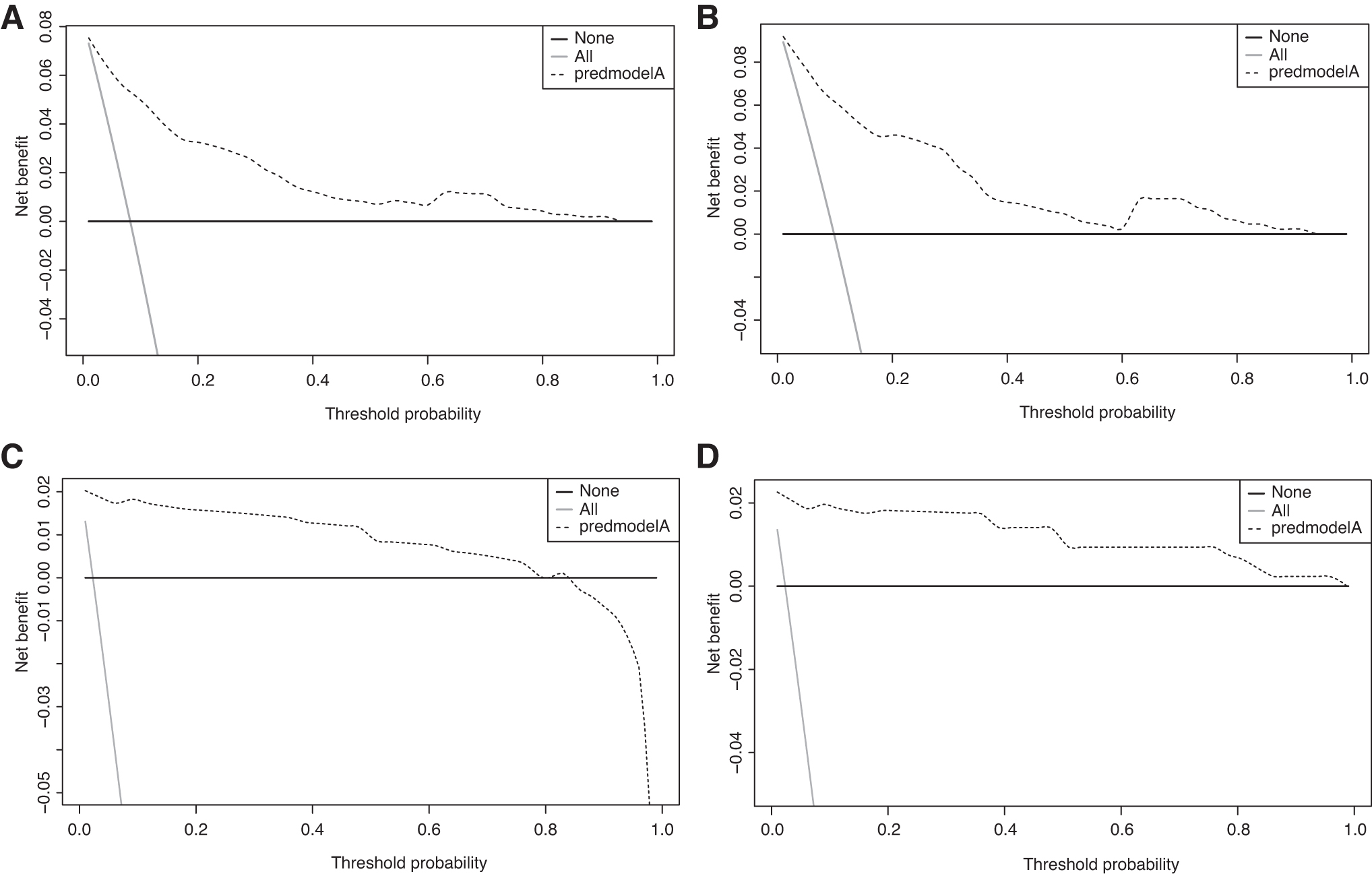
DCA.
Discussion
In recent years, PCNL has been widely used in the treatment of upper urinary calculi due to its high rate of stone removal. 17 However, PCNL also has some disadvantages, and infection is one of its most common complications. In this study, the preoperative predictors of sepsis after PCNL infection included diabetes, HU of hydronephrosis >6.0, AGR <1.705, hs-CRP/Alb >0.065, staghorn calculi, and urinary nitrite positivity. Diabetes has been reported to be an independent risk factor for sepsis, which is consistent with the findings of this study. 18 In this study, abnormal urine routine was defined as high WBCs or positive nitrite in urine routine. Although urine culture is recognized as the gold standard for the diagnosis of urinary tract infection, this method is time-consuming and delays the treatment to a certain extent. Therefore, urine culture was not used as the main diagnostic basis for abnormal urine routine in this study. In a recent study, urine nitrite showed a better clinical net benefit than urine culture and WBC, 19 –21 and the above conclusions are consistent with this study. Some patients have complicated urinary calculi with infection, and it is difficult to completely eliminate urine WBCs after conventional anti-infective treatment.
Therefore, in this study, it is believed that the normal indicators of routine urine reexamination after the application of antibiotics in patients with urinary tract infection are nitrite negative and that urinary WBCs are greatly reduced.
Some studies have shown that with increases in the size and number of stones, the probability of infection after PCNL also increases. 22 In this study, univariate and multivariate analyses indicated that the presence of a staghorn calculus was an independent risk factor for sepsis development after PCNL. Due to the large volume of staghorn stones, the operator often continues to expand the puncture channel to 24F to expand the surgical field, resulting in greater damage to the kidney and mucosa. Surgeons often need to adjust the angle of the sheath to further remove the calculi of each calix, which can easily cause tearing of the renal cortex, open blood vessels, and increase absorption of the perfusion fluid, which leads to an increased risk of infection. 23
Postoperative infection is closely related not only to the operation situation, but also to the general physical condition of the patient. The basic condition of the patient can be evaluated according to the nutritional status of the patient, and serum albumin concentration is an effective assessment of nutritional status. Some studies have found that patients with low levels of albumin have a higher risk of postoperative infection. 24 Globulin is the stress product of patients to resist inflammation when the patient's nutritional status is poor or under inflammatory stress; a decrease in albumin or an increase in globulin can lead to a decrease of AGR. When the patient is in a state of systemic inflammation before surgery, the possibility of postoperative infection is increased. 13,15 CRP is an acute-phase reactant produced by hepatocytes, and hs-CRP is a sensitive marker of systemic low-grade inflammation. The hs-CRP/Alb ratio has been shown to be a predictor of patient prognosis. 25 Combined with recent reports and the results of this study, we believe that the AGR and the hs-CRP/Alb ratio are predictors of postoperative urinary tract infection. 13,14,18
Pyonephrosis refers to infected hydronephrosis, and it is considered a urological emergency that can rapidly progress to sepsis and septic shock. Therefore, rapid diagnosis and treatment of pyonephrosis are essential to prevent sepsis. At present, some studies distinguish pyonephrosis from hydronephrosis by measuring the HU value of the fluid in the dilated renal collecting system. 26 The extended renal pelvis can be easily measured by HU because of routine preoperative CT examination. Some studies have proven that patients with sepsis have a higher HU value, which is consistent with our study, 27 so the HU value can be used as a potential predictor of urinary tract sepsis.
The most serious complication after PCNL is septic shock, which has a mortality rate of up to 50%, and the mortality rate increases by 6% every hour that septic shock treatment is delayed. 28 Therefore, early prediction of sepsis progression to septic shock is of great significance. At present, there are few studies on septic shock after PCNL. According to Wu's study, the WBC count of patients with septic shock reached the lowest value 2 hours after surgery, and then the WBC count gradually increased. 10 The reason for this phenomenon may be that the inflammatory factors produced by endotoxin activate the systemic inflammatory reaction, leading to a large consumption of WBCs. According to Cheng's study, the WBC ratio performed better than absolute numbers because it eliminated the baseline variance. 9 The results of this study are consistent with the above studies. When the pre- and postoperative WBC ratios were higher than 1.5, the probability of septic shock in patients with sepsis was significantly increased. Therefore, the sepsis prediction model combined with the pre- and postoperative WBC ratios can effectively and quickly predict the progression of sepsis to septic shock.
The formation of struvite stones is directly related to urease-producing bacteria. During PCNL, bacteria and endotoxins in struvite stones are released into the systemic circulation, leading to postoperative infection, so in some studies, struvite is an independent risk predictor of infection-related complications in PCNL patients. 29 In this study, preoperative factors were used to predict sepsis development, while HU cannot accurately predict struvite 30 and obtaining stone composition analysis results required 1–2 days after the operation; thus, struvite was not an independent predictor. In univariate and multivariate analyses, struvite stones were not associated with the progression of sepsis to septic shock.
This study has some limitations. First, this study was a retrospective study with potential selection bias. Second, the present study did not further analyze the correlation between bacterial species and infection. Third, prospective studies with large samples are still needed to further verify the efficacy of the two prediction models.
Conclusions
Early recognition and treatment of sepsis and septic shock is critical. We established a predictive model of the development of sepsis after PCNL based on diabetes, HU of hydronephrosis, AGR, hs-CRP/Alb ratio, staghorn calculi, and urinary nitrite positivity. Furthermore, a new prediction model was established by combining the model mentioned above with the pre- and postoperative WBC ratios to predict the probability of the progression of sepsis into septic shock. These two prediction models help improve the early identification and screening of high-risk patients.
Footnotes
Acknowledgment
The authors are very grateful to Dr. Changying Li of Tianjin Medical University, for statistical help.
Authors' Contributions
X.H.: protocol development, data collection, and article writing. X.W.: project development, data collection, and data analysis. H.W.: data collection. H.D.: data collection. S.Z.: article editing. L.W.: data analysis. Z.L.: data collection. H.Y.: article editing.
Ethics Approval and Consent to Participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional and/or National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of The First Hospital of Hebei Medical University.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.