
Abstract
Introduction:
Simple prostatectomy (SP) and laser enucleation of the prostate (LEP) are treatments for symptomatic benign prostatic hyperplasia (BPH) in men with large glands (e.g., >80 g). The decision between the two operations is often dependent on surgeon preference/experience and equipment availability. As the use of minimally invasive techniques, such as robotic-assisted simple prostatectomy, has increased for the treatment of large gland BPH, studies comparing the outcomes and cost of these modalities in a contemporary cohort are lacking.
Methods:
All-payer data from Healthcare Cost and Utilization Project State Databases from Florida, New York, California, and Maryland from 2016 to 2018 were used to identify adults who underwent SP or LEP for BPH. Patient demographics, facility characteristics, revisit rates, and cost of the index hospitalization were examined. Multivariable logistic and gamma generalized linear regression models were utilized to compare predictors of the operation performed, 30-day revisits, and index hospitalization cost among the two operations.
Results:
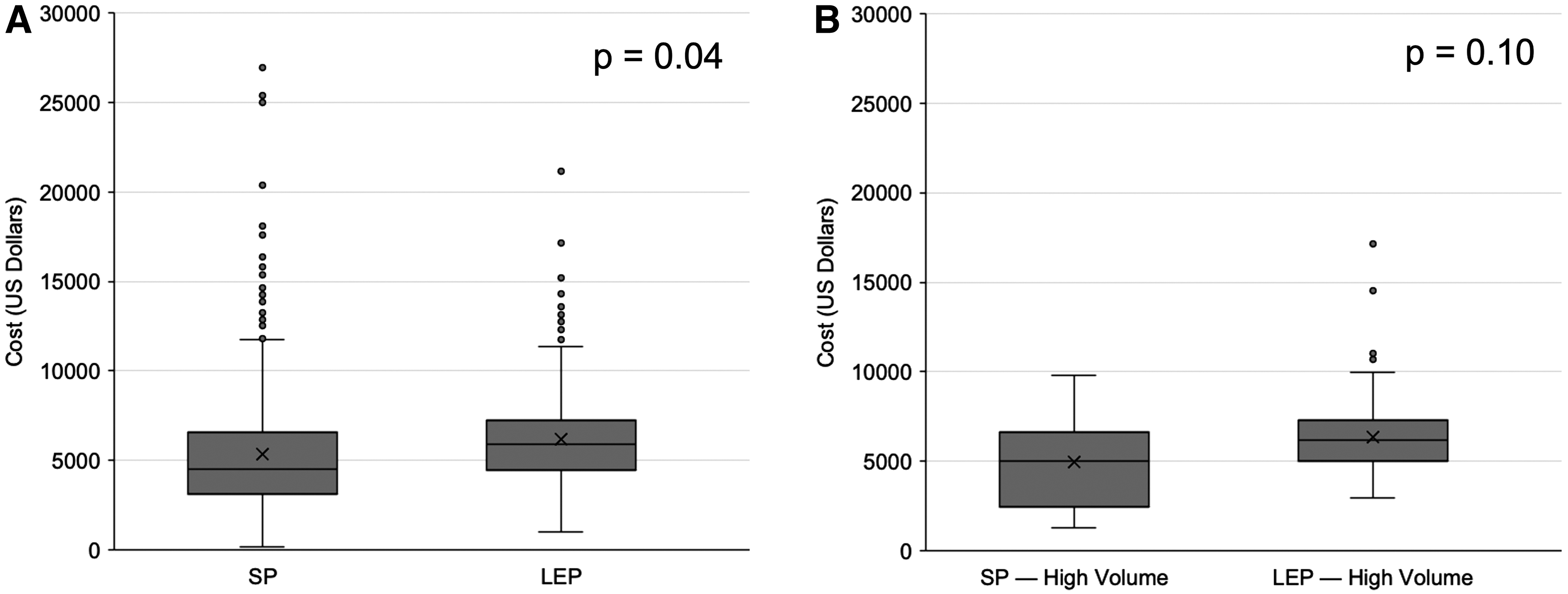
Of the 2032 patients in the cohort, 1067 (46.4%) underwent LEP and 965 (41.9%) underwent SP. On multivariable logistic regression analysis, SP patients were younger, had higher comorbidity scores, and were more likely to be uninsured compared with LEP patients. Thirty-day revisit rates among the operations were equivalent (odds ratio 0.89, 95% confidence interval 0.63–1.27, p = 0.05). The mean adjusted cost of the index hospital stay for LEP was significantly greater than that of SP ($7291 vs $6442, p = 0.04). However, our sub-group analysis examining high-volume centers revealed no significant differences in cost ($6184 vs $5353, p = 0.1).
Conclusions:
Across the four states examined, SP and LEP were performed with comparable volume and had similar rates of 30-day revisits. The SP was less expensive than LEP overall; however, among high-volume facilities, the cost of both operations was reduced, such that they were equivalent.
Introduction
Benign prostatic hyperplasia (BPH) is an exceptionally prevalent disease, affecting over 60% of men by 60 years of age. 1 This translates into a significant economic burden, with an estimated annual cost of BPH care of $4 billion in the United States. 2 Historically, men with larger prostates (e.g., >80 g) were treated surgically with open simple prostatectomy (OSP). 3
However, laparoscopic and robotic-assisted simple prostatectomy (RASP), as well as anatomic endoscopic enucleation of the prostate, have been increasingly utilized as each has demonstrated shorter hospital stays and decreased blood loss compared with the OSP approach. 4 –7 Current guidelines recommend simple prostatectomy (SP) or laser enucleation of the prostate (LEP) for larger prostates, depending on surgeon preference, experience, and equipment availability. 8,9
Although studies have compared clinical outcomes of SP and LEP, and found each to be safe and effective, there are few data on the comparative cost of the index operations or on post-operative readmissions. 10,11 In addition, it remains largely undefined whether cost or readmissions vary with operative volume—particularly in the context of a steep learning curve for Holmium LEP (HoLEP) (∼27–50 cases) compared with RASP (∼10–12 cases for experienced robotic surgeons). 12 –15
For example, it is possible that cost and readmission rates are similar among LEP and SP, given their largely similar complication rates; alternatively, these outcomes may vary across operations, potentially due to the inherent differences among transurethral vs robotic, laparoscopic and open surgery, or differences previously seen in clinical outcomes such as length of index hospitalization and blood loss. 10,11 Further, operative volume may impact cost and readmission rates as surgeons overcome each respective operation's learning curve.
In this context, we utilized all-payer claims data to examine utilization, index hospitalization cost, and 30-day revisit rates of SP and LEP. In addition, we evaluated the impact of surgical volume on these outcomes and hypothesized that perioperative outcomes for these surgical approaches are comparable when adjusted for surgeon/facility experience. Our findings provide critical insight into the potential costs and health care utilization implications of these operations, as their use for the treatment of BPH in large prostates evolves.
Methods
Data source
The 2016 and 2018 Healthcare Cost and Utilization Project (HCUP) State Ambulatory Surgery and Services Database (SASD), State Inpatient Database, and State Emergency Department Database from Maryland (MD), California (CA), Florida and New York (NY) were used to identify patients. These administrative databases are maintained by the Agency for Healthcare Research and Quality (AHRQ) and contain encounter-level data on hospital-affiliated and/or -owned facilities. 16 A limited number of state datasets contain de-identified linkage numbers that allow identification and tracking of individuals with multiple health care encounters within the same year.
Study population
Using Current Procedural Terminology (CPT) codes, we identified patients ≥18 years of age who underwent LEP or SP and had an International Classification of Diseases-10th Revision (ICD-10) diagnosis code for BPH (Supplementary Data). Baseline patient characteristics consisted of age, race, insurance status, residence, distance to treating hospital, county-level median household income quartile, comorbidity using the Elixhauser modification of the Charlson Comorbidity Index, and education.
Distance to the treating hospital was defined using the great circle distance and categorized as very near (<12.5 miles), near (12.5–49.9 miles), or far (≥50 miles). 17 Facility-level characteristics included location, operative volume, and total episode-related charges converted to costs via the HCUP cost-to-charge ratio files. Facilities in the top quartile by annual SP and LEP volume were defined as “high-volume,” as previously described. 17 The CA does not report charges within SASD; these cases were excluded from our cost analysis (n = 767). All encounters with missing covariates (n = 106) were considered missing at random, as we control for all observable variables affecting the probability of missingness. 18
Statistical analyses
Our primary outcome was receipt of SP or LEP. Secondary outcomes were 30-day revisit rates, defined as any emergency department encounter or hospital admission, and index hospitalization costs. Bivariate comparisons among categorical and continuous variables between groups were examined using Pearson's chi-square and the Wilcoxon rank sum tests, respectively.
Multilevel logistic regression models adjusted for the abovementioned covariates as fixed effects and facility clustering as a random effect were used to identify factors associated with undergoing SP or LEP, as well as 30-day revisits. Gamma generalized linear mixed regressions with a log link adjusted for facility clustering were employed to compare costs between procedures. Sensitivity analyses were performed with patients stratified by facility volume, as well as testing interaction effects between the procedure performed and facility volume and travel distance.
Lastly, we utilized 2-stage least-squares regression to perform an instrumental variable analysis in an effort to account for both observed and unobserved variables that influence perioperative outcomes (e.g., cost and 30-day revisit). 19 We identified travel distance as a potential instrument for our analysis, as previously described in the urology literature. 20 Before conducting the second stage of our 2-stage least-squares regression model, we explored the validity of travel distance as an instrument; F-statistics (p = 0.4) did not demonstrate endogeneity between travel distance and procedure type. Therefore, we elected to simply adjust for travel distance in our multivariable models.
All analyses were performed using STATA 14 MP (STATA Corp, College Station, TX), with a two-sided significance level set at p < 0.05. The Institutional Review Board at the University of North Carolina at Chapel Hill determined this study exempt.
Results
Patient demographics
A total of 2032 patients met inclusion criteria, of whom 1067 (52.5%) underwent LEP and 965 (47.5%) underwent SP. Univariate comparisons between individuals treated with LEP and SP are shown in Table 1. Patients who underwent LEP were older (71 vs 62 years, p < 0.001). Length of stay was longer for LEP vs SP, at 0.32 vs 0.25 days (p < 0.001), although whether this is a clinically meaningful difference is debatable considering both were <1 day. The LEP patients were more likely to be treated in a high-volume center, live closer to the operative facility, reside in a large metropolitan area, and have white race (Table 1). Regarding insurance status, Medicare was the most common payer in each group, but comprised a larger proportion of LEP patients at 71% compared with 44% of SP patients (p < 0.001). There were significant differences among the groups in geographic distribution, with a greater proportion of LEP patients residing in CA and NY (p < 0.001).
Patient and Facility Characteristics According to Procedure Type
Cells with <10 individuals are suppressed per HCUP reporting requirements.
High volume defined as top quartile by annual facility volume.
Distance to the treating hospital was defined using the great circle distance (distance in miles between the patient's reported residence and the hospital that reported the case)—defined as very near (<12.5 miles), near (12.5–49.9 miles), and far (≥50 miles).
County-level median household income quartiles.
CA = California; FL = Florida; IQR = interquartile range; LEP = laser enucleation of the prostate; MD = Maryland; NY = New York; SD = standard deviation; SP = simple prostatectomy.
Predictors of procedure type
The results of our multivariate logistic regression model predicting receipt of SP compared with LEP are shown in Table 2. Older age was negatively associated with receipt of SP (odds ratio [OR]: 0.91, 95% confidence interval [CI]: 0.90–0.93, p < 0.001). Significant predictors of undergoing SP were higher comorbidity score (0 vs ≥3: OR 2.58, 95% CI: 1.67–3.99, p < 0.001) and being uninsured compared with privately insured (OR 13.14, 95% CI: 5.15–33.65, p < 0.001). We again saw geographic differences, with patients residing in MD more likely to undergo SP compared with the three other states examined. Travel distance, facility operative volume, race, income, and urban/rural status did not significantly predict odds of undergoing SP or LEP (Table 2).
Multivariate Logistic Regression Analysis Predicting Receipt of Simple Prostatectomy vs Laser Enucleation of the Prostate
Distance to the treating hospital was defined using the great circle distance (distance in miles between the patient's reported residence and the hospital that reported the case)—defined as very near (<12.5 miles), near (12.5–49.9 miles), and far (≥50 miles).
High volume defined as top quartile by annual facility volume.
County-level median household income quartiles.
CI = confidence interval; OR = odds ratio.
Predictors of revisit
The overall 30-day revisit rate was not significantly different among LEP and SP at 12.37% vs 11.07% (p = 0.05). The results of our multivariate logistic regression model predicting 30-day revisits are shown in Table 3; again, no difference in odds of revisit was seen between LEP and SP (OR 0.89, 95% CI 0.63–1.27, p = 0.05). Higher comorbidity burden (0 vs ≥3: OR 4.47, 95% CI: 2.78–7.17, p < 0.001), Hispanic compared with White race (OR 2.02, 95% CI 1.31–3.10, p < 0.001), and geographic location were associated with greater odds of a revisit. No other factors examined, including sensitivity analyses testing for interaction effects, were significantly associated with 30-day revisits.
Multivariate Logistic Regression Analysis Predicting 30-Day Revisit
Distance to the treating hospital was defined using the great circle distance (distance in miles between the patient's reported residence and the hospital that reported the case)—defined as very near (<12.5 miles), near (12.5–49.9 miles), and far (≥50 miles).
High volume defined as top quartile by annual facility volume.
Procedural costs
Figure 1A displays the unadjusted costs of SP and LEP. The overall mean adjusted cost of the index hospitalization for LEP was significantly greater than that of SP ($7291 vs $6442, p = 0.04, Table 4). Figure 1B displays the impact of high operative volume on the cost of each operation. The sub-group analysis of high-volume centers revealed no significant differences in costs among LEP and SP ($6184 vs $5353, p = 0.1). The sub-group analysis of low/medium volume centers revealed a significant difference in costs ($7228 vs $6339 for LEP vs SP, respectively, p < 0.001, Supplementary Table S1). The test for interaction between travel distance and procedure was significant, with greater travel distance conferring greater cost across both procedure groups (p < 0.05 for both procedures, Supplementary Table S2).
Mean Adjusted Cost Associated with Surgical Encounter
Discussion
This study examined all-payer data across four states and found that a comparable number of SP and LEP operations were performed for BPH. On multivariable logistic regression, SP patients were younger and had higher comorbidity scores. Overall, the mean adjusted cost of the index surgical encounter for LEP was nearly $850 greater than RASP. However, when stratified by facility operative volume, higher volume facilities saw decreased cost for both operations, and the cost difference between the two was no longer statistically significant. There was no difference in 30-day revisit rates on multivariable logistic regression among the two groups. Taken together, this study suggests that although SP may be less expensive than LEP overall, with surgeon and facility experience the costs of both operations are reduced, such that they are equivalent at high-volume centers.
The cohort examined herein appears largely similar to previously published reports. For example, prior work on the utilization of BPH surgery also demonstrated that SP and LEP are performed with comparable frequency; specifically, SP accounted for about 3% of BPH operations compared with 4%–5% for HoLEP. 21 Further, regarding patient characteristics, at least one other study also found that RASP patients were younger and had higher comorbidity scores compared with those undergoing HoLEP. 11
Nevertheless, our study expands on prior work examining the utilization and clinical outcomes of SP and LEP by demonstrating the cost differences of the index surgical episodes. Further, we show that high-volume centers can reduce the costs of each operation, such that cost differences are eliminated. Previous work comparing HoLEP with OSP found that HoLEP was on average less expensive. 22 Others have compared costs of RASP to OSP and found operating room charges were greater with RASP; however, RASP was less expensive when considering higher costs of post-operative hospitalization for OSP. 23,24
Similarly, prior work has shown that post-operative complications after SP increase in-hospital charges. 25 Considering that minimally invasive SP has demonstrated lower transfusion and complication rates compared with the open approach, a reduction in the cost of post-operative care for RASP compared with OSP is not surprising. 6,7 Although we were unable to differentiate RASP from OSP in this study, due to limitations of CPT coding in the dataset used, previous work has shown increasing utilization of RASP compared with OSP, which could be a driver of the cost savings seen in this study. 26
The reduction in costs seen when evaluating high-volume centers is notable and remains consistent with published literature on the relationship between volume and cost in urologic surgery. For example, the cost of robot-assisted laparoscopic radical prostatectomy decreases with higher surgical volume (surgeon and hospital volume). 27 As described by Kordan et al, the use of a greater number of robotic instruments for RASP may increase intraoperative charges, and in this way surgeon experience and technique may directly affect costs. 28 In regard to HoLEP, higher costs have been seen while surgeons are on the operation's learning curve, potentially driven by conversion to resection and longer enucleation times. 29 Collectively, these results suggest that the steeper learning curve for HoLEP compared with RASP may translate to the higher costs seen at lower-volume facilities; however, with greater surgical volume both operations are associated with reduced, and largely similar costs.
Importantly, we did not find a significant difference in 30-day revisit rates among the operations. This is not surprising given that prior work has demonstrated largely similar complication rates. 10,11 One study examining outcomes of BPH operations across 5 years saw a difference in readmissions in 1 year only, with HoLEP having lower readmissions than OSP and several transurethral BPH procedures. 21 In addition to the implications of this finding for patient experience and health care utilization, it is reassuring that any potential differences in cost of post-operative care outside of the index hospitalization, which were not examined in this study, would likely not be driven by readmissions.
Our study does have several limitations. First, our population represents four states and may not reflect national trends. Nevertheless, within these states we captured all patients regardless of payer status or hospital affiliation. 16 Second, there may be unmeasured differences among patients not completely captured by administrative data, for example, clinical differences such as prostate size, prostate specific antigen, operating time, surgeon experience, etc. To account for this, we included broad patient characteristics in our modeling.
Further, we performed an instrumental variable analysis attempting to adjust for unmeasured confounders. Third, we could only examine index hospitalization costs, and we could not investigate the drivers of these costs at a granular level; however, index hospitalization costs are arguably most relevant as they encompass the operation and inpatient post-operative recovery. Fourth, we were unable to differentiate OSP from RASP, or the various energy sources for LEP, due to limitations of CPT codes used for these procedures.
Fifth, our data are from 2016 to 2018, and costs will likely evolve over time, particularly as new technologies and techniques are introduced. For example, recent advancements in laser technology have facilitated some centers to implement same-day discharge after HoLEP, resulting in decreased costs. 30 Despite these advances, such technologies are relatively new and still being disseminated; therefore, at present, many HoLEPs nationwide are likely not performed as outpatient surgery, particularly in larger glands. Lastly, this analysis does not examine costs of capital investments needed to perform these operations, such as the purchase of a robotic surgery platform, tissue morcellator, high-power laser, etc.; the value of these investments depends, in part, on utilization and is outside the scope of this study.
Despite these limitations, our findings have implications for payers, urologists, and patients. For payers considering coverage, our finding that among current, guideline-based surgical options for men with large prostates both SP and LEP have similar cost at high-volume centers suggests that these operations should be viewed equivalently. The decision to pursue one option over another should be left to the patient and their surgeon based on shared decision making.
For urologists, the finding that costs of SP and LEP are successfully reduced at high-volume centers suggests that lower volume surgeons may be able to adopt cost savings measures through sharing of best practices with centers of excellence. Lastly, the equivalent 30-day revisit rate among SP and LEP is a reassuring outcome for men considering surgical treatments of a large prostate.
Moving forward, a nuanced examination of the drivers of costs for each operation may be beneficial in identifying areas for savings. As the feasibility of outpatient surgery for large prostates is further refined, an analysis of updated data will be informative in this constantly evolving space. Ultimately, if other modalities gain widespread acceptance in this patient population, such as Prostatic Artery Embolization or Aquablation, investigations including these procedures will be warranted.
Footnotes
Authors' Contributions
S.R.H., W.F., H.K., and D.F.F. contributed to conception and design. D.F.F. contributed to acquisition of data. All authors contributed to analysis and interpretation of data, drafting and/or revising the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
D.F.F. was funded by an American Urological Association Research Scholars Grant.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.