
Abstract
Inguinal lymph node status is the single most important prognostic factor for survival in patients with carcinoma penis. Various modifications and alternatives to open inguinal lymph node dissection have been developed as the same is associated with high postoperative morbidity such as wound infection, skin flap necrosis, lymphorrhea, and lymphedema. Robot-assisted video endoscopic inguinal lymph node dissection (RA-VEIL) has the potential to accomplish thorough inguinal lymph node dissection with definitively reduced postoperative morbidity. In this video, we demonstrate our technique of RA-VEIL: The fascia lata first approach and highlight our technical modifications of the conventionally described procedure.
Featured Video
https://stream.cadmore.media/player/a5bf6d28-878a-4578-baa0-e6aeb8fdc25b
Indications
Robot-assisted video endoscopic inguinal lymph node dissection (RA-VEIL) can be utilized in the following manner: As a To perform
Preoperative Preparation
Clinical examination of the penile tumor, bilateral inguinal regions, and abdomen are of paramount importance. Imaging in the form of CT/MRI of the inguinal region is obtained in patients where clinical examination may be unreliable (obese individuals/previous groin surgery or radiation/groin edema). In patients with palpable/enlarged inguinal lymphadenopathy, the site/size/number/mobility/relationship to skin and deeper tissues are to be documented. In addition, fine needle aspiration cytology from palpable nodes is done to confirm metastatic involvement.
A written informed consent with details pertaining to the disease status, expected prognosis, and available surgical approaches (open/laparoscopic/robot assisted) is taken. Additional risks and potential complications of the said procedure such as wound infections, skin flap necrosis, postoperative lymphorrhea/lymphedema and need for long-term follow-up are clearly explained. RA-VEIL can be safely combined with penectomy or may be performed as a separate procedure. First generation cephalosporin (cefazolin) is administered at induction.
Patient Positioning
All procedures are performed under general anesthesia with epidural analgesia using the Da Vinci Xi system (Supplementary Video). The patient is positioned securely on the operating table in low lithotomy position with 10- to 20-degree Trendelenburg tilt. The pressure points are padded adequately and shoulder supports applied. The hips are placed in slight extension, external rotation, and abduction with flexion at the knee joint and legs supported by Allen Stirrups. Such positioning (Fig. 1) allows for performing bilateral groin dissections without repositioning the patient or robotic cart and, in addition, aids in marking of the femoral triangle by making the tendon of the adductor longus taut. After hair clipping, the operative field (abdomen till knee joints) is prepped and draped. Surface marking of the femoral triangle and Daseler's quadrangle (DQ) are marked palpating the bony and soft tissue landmarks (Fig. 2).

Depiction of patient positioning for RA-VEIL. The patient is laid in low lithotomy position with 10- to 20-degree Trendelenburg tilt with the hips in slight extension, abduction, and external rotation and legs flexed and supported by Allen Stirrups. RA-VEIL = robot-assisted video endoscopic inguinal lymph node dissection.
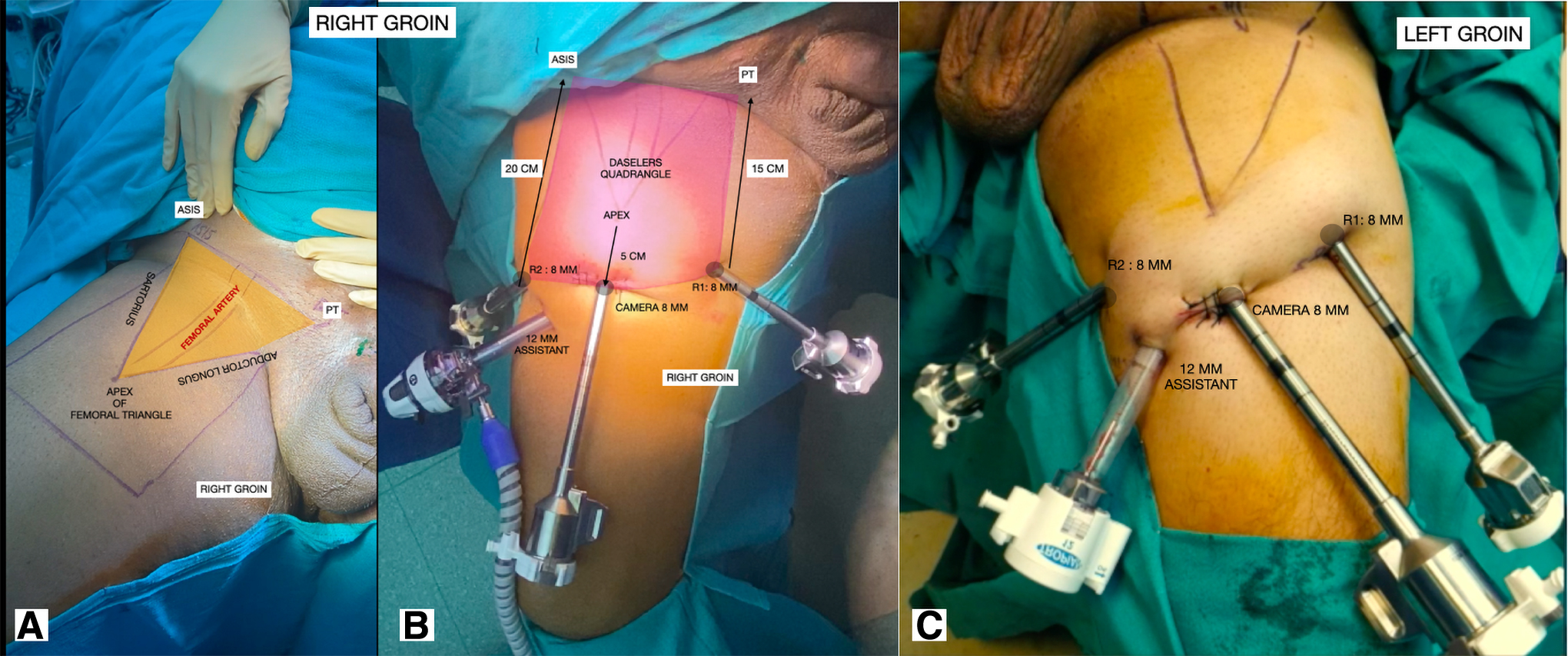
Bony and soft tissue landmarks used for marking the femoral triangle and Daseler's quadrangle for the right groin
Port Placement
The port position is as shown in the Figure 2. The 8 mm camera port is placed 5 cm distal to the apex of the femoral triangle. A 4 cm transverse incision is given centered at the camera port site. The incision is deepened via the fatty Camper fascia and the membranous Scarpa fascia (SCF). The conventionally described procedure 1 advocates development of sub-Scarpal plane by blunt finger/balloon dissection. We have found that this potential plane is difficult to dissect and develop uniformly, and thus, we use the fascia lata first (FLF) approach. The fascia lata (FL) is an easily identifiable tough layer of the thigh, and the superficial inguinal lymph nodal (SILN) tissue is easily and uniformly lifted off this layer. Finger dissection alone or combined with balloon dilatation can be used to create adequate space for port placement.
The two remaining 8 mm robotic ports are placed at ∼8 cm distance from the camera port under finger guidance. The 12 mm assistant port is placed between the camera port and the left-hand instrument port for both sides such that the assistant is seated to the right of the patient's right leg during right video endoscopic inguinal lymph node dissection (VEIL) and in between the legs for left VEIL (Fig. 2). Finally, the camera port site incision is closed with interrupted sutures around 8 mm port, and the pneumoderma is created by insufflating carbon dioxide at 8 to 10 mm Hg connected to the 12 mm assistant port.
Docking and Instrumentation
The Da Vinci Xi system is side docked as shown in Figure 3. The procedure begins by using the 0-degree telescope. The Monopolar scissor is taken on the right-hand side and the fenestrated bipolar in the left hand.

Side docking for the Da Vinci Xi patient cart. Three arms configuration is used and choice of arms depending on the side of dissection. Bilateral inguinal dissections can be accomplished without repositioning either the patient or patient cart.
Surgical Steps
Step 1. Defining the surgical landmarks and defining dissection boundaries
Blunt and sharp dissection is used to lift off the SILN packet (at the roof) from the FL (at the floor) within the boundaries of the DQ. The assistant can guide the surgeon through this step by use of digital indentations on the skin surface or by using a needle. Also, the muscle fibers may sometimes be visible through the deep fascia itself guiding the surgeon. Frequently, cutaneous perforators from the underlying femoral vessels may be encountered, which may be safely clipped and divided.
Unlike the conventionally described technique, where the great saphenous vein (GSV) is seen on the floor, here, it is seen at the roof and guides the surgeon toward the saphenofemoral junction (SFJ). Once the SFJ is identified, dissection then proceeds cranial on both sides of the SFJ till the spermatic cord (seen medially), the inguinal ligament, and external oblique aponeurosis are visualized (Fig. 4).
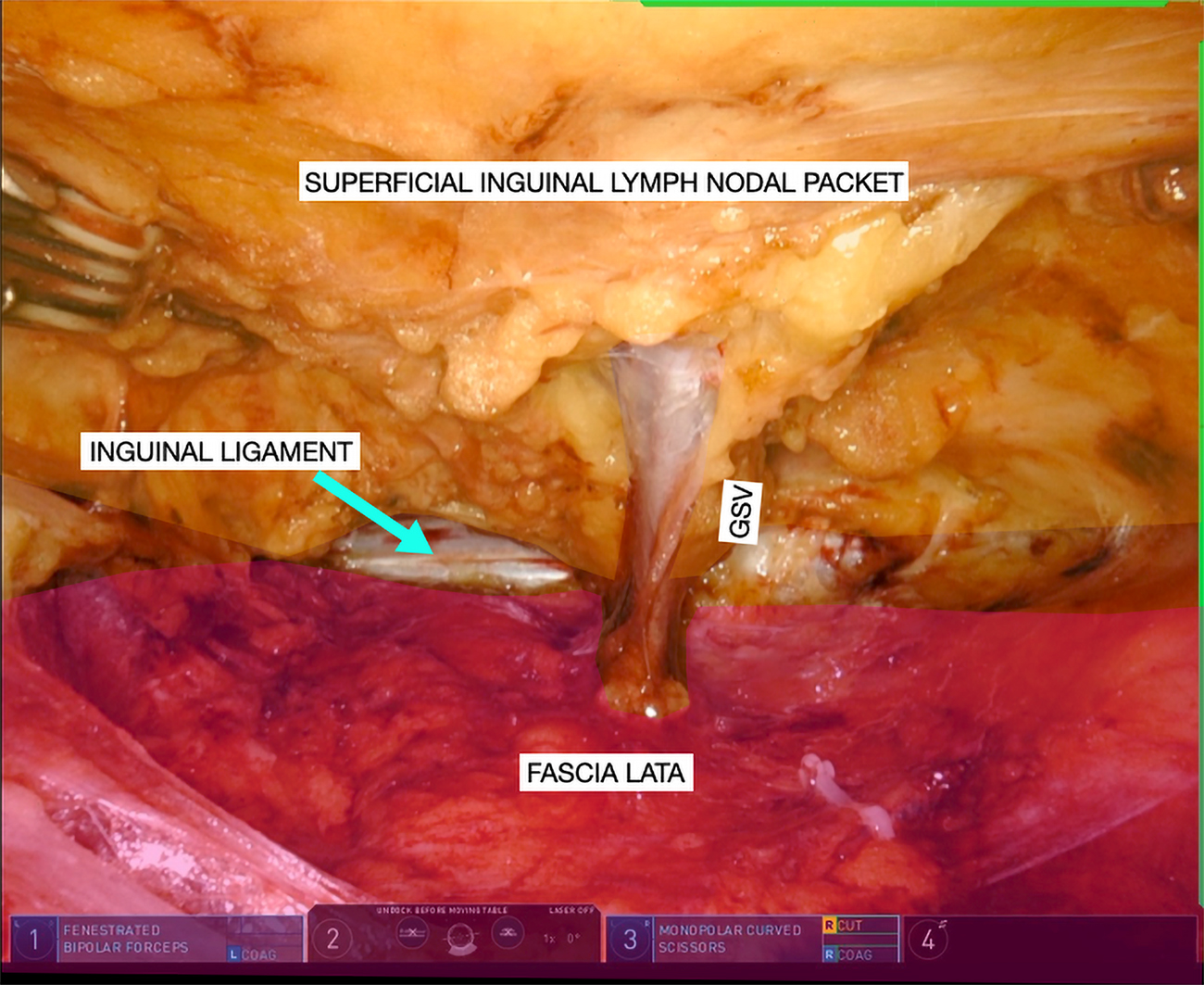
The superficial inguinal lymph nodal packet (depicted in yellow) has been lifted off the fascia lata (depicted in magenta) from the apex of the femoral triangle to the inguinal ligament (blue arrow). The GSV is seen draining into the femoral vein. GSV = great saphenous vein.
Step 2. SILN dissection
For this step, a 30 degree up telescope is used. The saphenous vein is dissected free from the SILN packet and dropped down from the apex of the femoral triangle till the SFJ. This maneuver serves two roles. First, it helps identify the overlying SCF early and, second, makes the dissection around the SFJ easy. Any tributaries draining into the GSV are clipped and divided close to the saphenous vein.
In the conventional technique, 1 when the SILN packet is first released from the SCF, additional assistance is required to lift it while the surgeon dissects it free from the FL. With the FLF approach, the downward traction applied by the fenestrated bipolar is countered by the insufflated carbon dioxide, which lifts the skin flap upwards (Fig. 5a). This makes it easy to release the SILN packet without assistance and enables preservation throughout the dissection boundaries, which translates into uniform skin flap thickness and lesser wound-/flap-related complications in the postoperative period. The bedside assistant can also guide about flap thickness by assessing the transillumination (Fig. 5b).
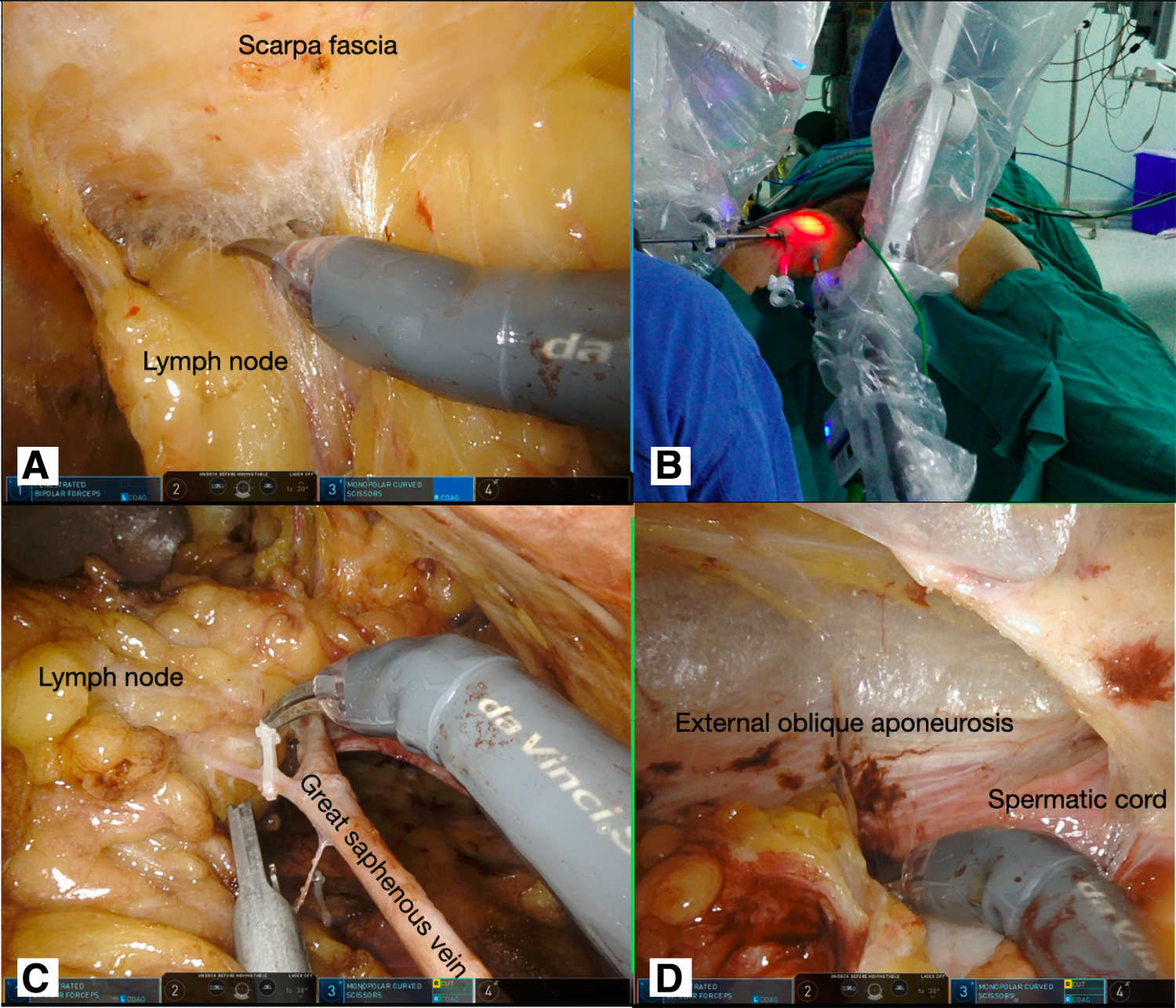
Depicts key steps during superficial inguinal lymph node dissection. Using a 30 degree optic with up orientation, the lymph node packet is dissected free from the Scarpa fascia
The GSV should be preserved whenever feasible as this has been shown to reduce the incidence of postoperative lymphorrhea/lymphedema (Fig. 5c). However, in cases where nodal clearance is hampered by the GSV, it should be sacrificed. It is preferable to clip lymphatics where possible to reduce postoperative lymphorrhea. The completely dissected SILN packet is delivered via the camera port incision site and sent for frozen section analysis. If positive, deep inguinal lymph node dissection is commenced after redocking the robot.
Step 3. Deep inguinal lymph nodal dissection
The FL is now opened starting from the SFJ till the apex of the femoral triangle to expose the femoral vessels. Lymphatics anterior to the femoral artery and anteromedial to the femoral vein are dissected to expose the underlying pectineus fascia (Fig. 6). Dissection lateral to the femoral artery is avoided to prevent injury to the femoral nerve and the profunda femoris artery. The cranial limit of deep dissection is the inguinal ligament. Dissection then moves to removal of the lymph node of Cloquet that lie medial to the femoral vein. The pneumoderma pressure is now reduced to 5 mm Hg to check for hemostasis. Once confirmed, the ports are removed, and the deep lymph nodal packet is retrieved from the camera port wound. The wounds are closed over suction drains and compression dressing applied.
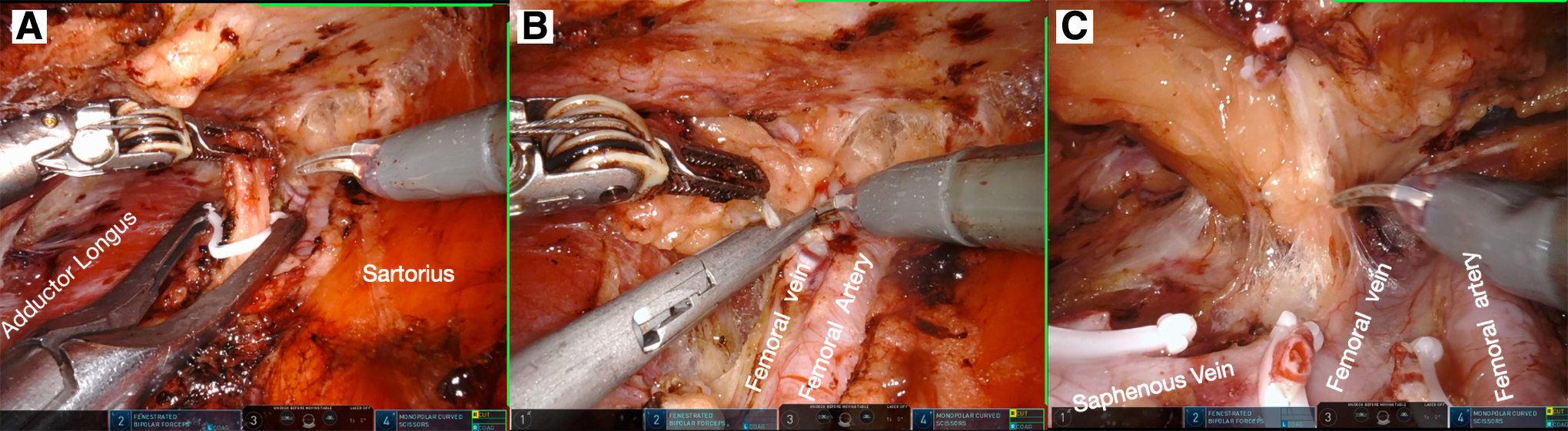
Depicting key steps during deep inguinal lymph node dissection. The lymphatics are clipped at the apex of the femoral triangle and divided
Step 4. Technical modifications
RA-VEIL in patients with proven inguinal lymph nodal metastasis
In these patients, once the plane superficial to the FL is created as described in Step 1, the fascia is opened and deep inguinal lymph node dissection is performed as described earlier. Once this is completed, the deep inguinal lymph node packet is now attached to the SILN packet, both of which are now dissected off the SF as described above and removed in toto.
Step 5. Postoperative care
The patient is allowed orally in the evening of surgery and early ambulation is encouraged. We do not usually use postoperative anticoagulation. The patient and caregivers are educated regarding drain care and daily drain output monitoring. Compression stockings are to be worn during daytime and can be removed at bedtime.
Drains are removed once output is <50 mL/day for 3 or more days. Till the time drains are in situ, the patient receives oral antibiotics (cefuroxime/amoxicillin + clavulanic acid). The patient is advised to visit the emergency in case he develops fever, groin pain, or swelling.
Step 6. Troubleshooting
Loss of pneumoderma is a frequent occurring that makes dissection difficult due to lack of exposure. To avoid this, skin incision at the port sites should be just enough to snugly admit the trocar. A practical tip to assess this is that rotation of the port also causes the port site skin to rotate along. In addition, the incision at the camera port site should be closed with closely placed interrupted (simple/vertical mattress) sutures such that the camera port does not easily get displaced.
Subcutaneous emphysema is also a frequent occurrence that can sometimes reach up to the neck. It may also lead to carbon dioxide retention. We have observed that pneumoderma pressures of 8 to 10 mm Hg are sufficient for dissection and are seldom associated with subcutaneous emphysema.
Small bleeders may be coagulated or clipped. If required, suture ligation can also be done. Major vascular injury intraoperatively is a relatively rare event. If significant vascular injury obscures vision, conversion to open should be done, but this is a very rare event.
Step 7. Outcomes
Several studies comparing the oncology and functional outcomes of RA-VEIL with the gold standard open approach have been published. Results from 3 such large studies 2 –4 are summarized in Table 1. These studies concluded that the lymph nodal yield was comparable to the open approach with significantly reduced rates of wound infection/flap necrosis and morbidity. The role of RA-VEIL in high-burden disease is yet evolving.
Summarizing Key Results from Large Series Comparing Open with Robot-Assisted Video Endoscopic Inguinal Lymph Node Dissection for Inguinal Lymph Node Dissection for Patients with Carcinoma Penis
Includes laparoscopic video endoscopic inguinal lymph node dissection cases as well.
RA-VEIL = robot-assisted video endoscopic inguinal lymph node dissection.
Step 8. Alternate approaches
Other approaches to minimally invasive inguinal lymph dissections have been described such as the lateral approach 5,6 and the antegrade hypogastric approach. 7,8 Uniform preservation of SCF with meticulous lymph node dissection with liberal clipping of lymphatics remain the key principles irrespective to the approach. We believe that our technical modifications make the procedure reproducible and easy to perform with minimal assistance.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.