
Abstract
Objective:
To compare the clinical efficacy and safety of holmium laser enucleation of the prostate (HoLEP) with bipolar plasmakinetic enucleation of the prostate (BPEP) in the surgical management of obstructive benign prostatic hyperplasia (BPH) at midterm (minimum 3 years) follow-up.
Patients and Methods:
Between June 2016 and January 2018, 181 patients who had bothersome lower urinary tract symptoms or refractory retention of urine due to obstructive BPH (prostate 32–128 g) were randomized to undergo either HoLEP or BPEP using the en bloc technique. Patient's age, associated comorbidities, baseline International Prostate Symptom Score (IPSS), maximum flow rate (Qmax), postvoid residual (PVR) urine, and quality of life (QoL) scores were comparable in both groups. From each group, 86 patients who completed regular follow-up for 36 months were analyzed.
Results:
The mean preoperative prostate volume was comparable in both groups (HoLEP group 61.09 ± 28.25 and BPEP group 62.66 ± 27.37 g). The HoLEP group showed a significantly better enucleation time (27.87 ± 13.18 minutes vs 38.37 ± 14.55 minutes), operative time (30.91 ± 14.82 minutes vs 41.63 ± 16.19 minutes), and enucleation efficiency (1.69 ± 0.28 vs 1.28 ± 0.06 g/min), with a lesser drop in hemoglobin (0.46 ± 0.23 vs 0.87 ± 0.26 g/dL). Bladder irrigation time, catheterization time, hospital stay, and sodium drop were comparable in both groups. One patient in the BPEP group needed clot evacuation. Both groups showed a significant reduction in IPSS, improvement in Qmax, reduction in PVR, and improved QoL scores at 3 months, which was maintained till 36 months. At the 3-year follow-up, two patients in each group needed reintervention for bladder neck contracture.
Conclusions:
HoLEP and BPEP provide comparable safety and efficacy in the treatment of bladder outlet obstruction due to BPH at the immediate and midterm (3–5 years) follow-up. HoLEP has an advantage of being faster with lesser perioperative morbidity.
Introduction
Transurethral resection of the prostate (TURP) is considered the gold standard for surgical management of lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH). A landmark study by Mebust et al 1 in 1989 noted that in over two decades of improvements in the TURP equipment and technique and perioperative care, the mortality rate due to TURP reduced from 2.5% to 0.2%, but the morbidity rate remained unchanged at around 18%. 2
To reduce this morbidity, Gilling and colleagues 3,4 proposed holmium laser enucleation of the prostate (HoLEP) as an alternative. Subsequently, multiple studies confirmed the improved efficiency with reduced morbidity using HoLEP, proposing HoLEP to be the new gold standard for surgical therapy of BPH. HoLEP has a distinct advantage for men with large prostatic adenomas who would otherwise qualify for open prostatectomy. 5
The button electrode, with bipolar energy, is conventionally used for coagulation or vaporization of the smaller prostate. It can also be used for enucleation using classical steps of endoscopic enucleation. 6,7 A single-center noncomparative study suggested that bipolar transurethral enucleation of the prostate (B-TUEP) could be a valid alternative to HoLEP. 8 Easy availability and reduced capital investment to acquire this energy source are added advantages.
There are few studies in literature comparing HoLEP with bipolar plasmakinetic enucleation of the prostate (BPEP). 6,9 This randomized prospective study was conducted to compare the efficacy and postoperative morbidity using HoLEP and BPEP, with a 3-year follow-up.
Methods
Over a period >2 years, from January 2016 to June 2018, 190 men were prospectively randomized to undergo either HoLEP or BPEP. Mandatory institutional review board approval was obtained for the study.
Study population and patient selection
Men older than 50 years, who needed surgical intervention for BPH due to bothersome LUTS or refractory urinary retention, were eligible to participate in the study. The inclusion criteria consisted of indications for surgical intervention for BPH and included (1) an enlarged prostate with LUTS refractory to medical management, (2) International Prostate Symptom Score (IPSS) >15, and (3) peak urinary flow rate (Qmax) <12 mL/s. Patients with a history of pelvic surgery or radiotherapy, urethral stricture, neurogenic bladder dysfunction, hypocontractile detrusor, or biopsy-proven prostate carcinoma were excluded from the study.
Randomization was performed as per a table of random numbers. Patients were included in the final analysis if they met the following criteria: (1) consented to participate in the trial after surgery, (2) completed all the required questionnaires during the follow-up, and (3) histopathology of the surgical specimen did not show prostate cancer (Fig. 1).
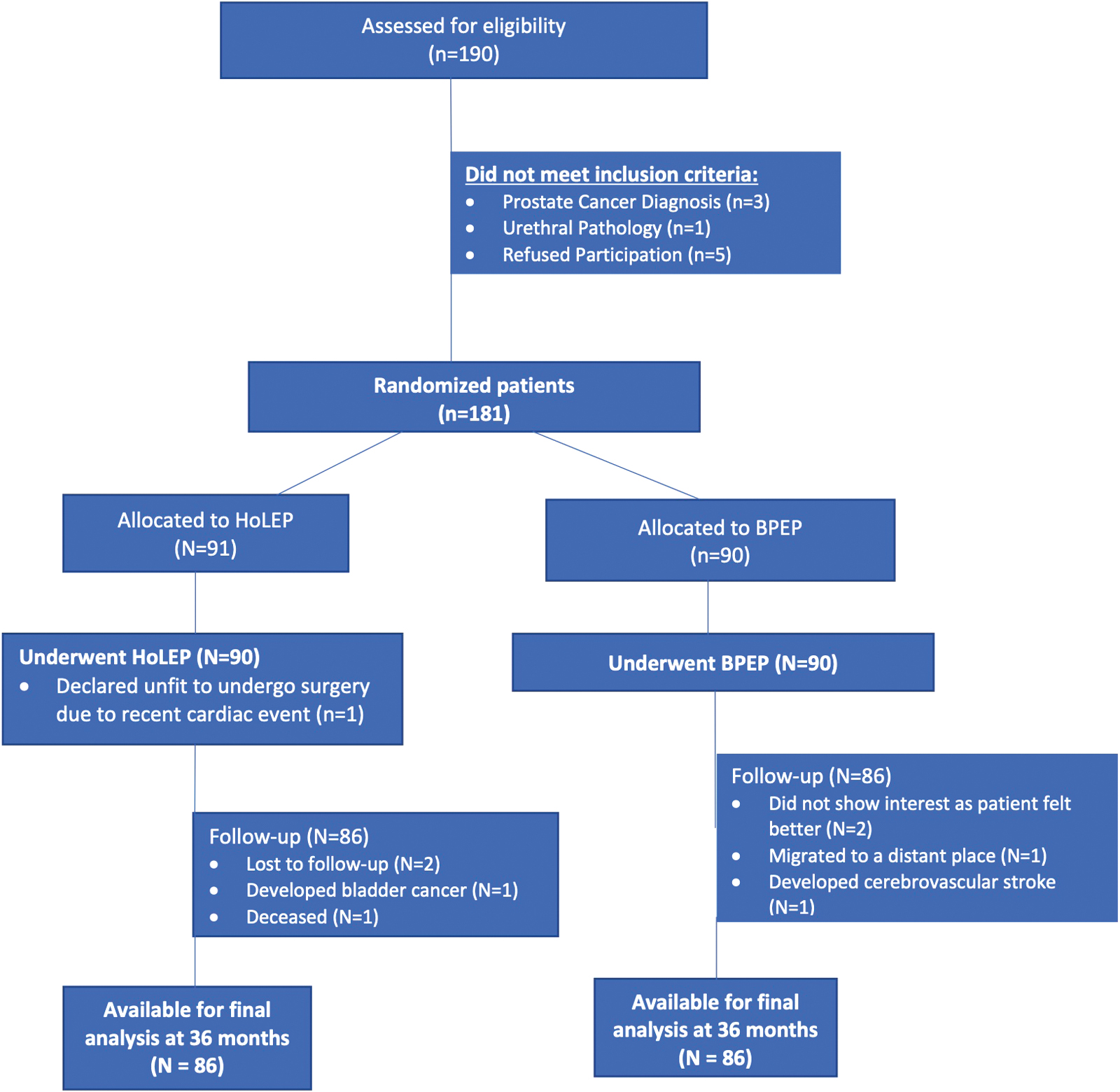
CONSORT diagram showing randomization, treatment, and follow-up. One hundred eighty-one patients were randomized at the beginning of the study. Finally, 86 patients in each group completed the study with minimum 36 months of follow-up. BPEP = bipolar plasmakinetic enucleation of the prostate; HoLEP = holmium laser enucleation of the prostate. Color images are available online.
Study variables
All patients had their demographic and baseline characteristics assessed, including age, comorbidities, IPSS, medications if any, maximum urinary flow rate (Qmax), prostate-specific antigen (PSA), postvoid residual (PVR) urine, prostate volume (PV) by transrectal ultrasound (TRUS), and quality of life (QoL) and International Index of Erectile Function (IIEF) scores.
Operative outcomes included operation time (from cystoscope insertion to catheter placement), enucleation time (from first laser incision to completion of enucleation), enucleation efficiency (weight of tissue enucleated divided by the time taken for enucleation), morcellation efficiency (weight of tissue morcellated divided by the time taken for morcellation), irrigation volume and postoperative bladder irrigation time, and drop in sodium and hemoglobin levels.
Postoperative catheter duration and hospital stay were not assessed as our institution has a fixed protocol for time of catheter removal and discharge from the hospital. Intra/perioperative complications (if any) and postoperative outcomes were recorded over 3 years (at 3, 6, 12, 24, and 36 months). Efficacy outcomes (IPSS, QoL score, Qmax, PVR volume, and PV by TRUS) were recorded at all follow-up visits. Serum PSA was measured at 3, 6, and 12 months of follow-up as a surrogate marker for completeness of the procedure.
Surgical technique and procedures
All surgeries were performed by a single surgeon (A.D.B.) with >18 years' experience in anatomic endoscopic enucleation of the prostate (AEEP). HoLEP was performed using a 26F Karl Storz (Tuttlingen, Germany) continuous-flow resectoscope with a laser working element and high-power holmium laser (100 W VersaPulse® PowerSuite™ Ho: YAG laser). A 550 μm SlimLine™ PowerSuite end-firing laser fiber (Lumenis) with energy settings of 2 J × 40 Hz (80 W) was used. Most procedures in the HoLEP group were performed using the en bloc HoLEP technique. 10
Bipolar enucleation was performed using the Olympus SurgMaster UES-40 bipolar generator, the OES-Pro bipolar resectoscope, saline continuous-flow irrigation, and button-type vaporesection electrodes (Olympus Europe, Hamburg, Germany). The modified en bloc bipolar enucleation technique was used in this study. 11 Morcellation was performed using the Wolf morcellator (Piranha; Richard Wolf GmbH, Knittlingen, Germany).
At the end of the procedure, continuous irrigation with physiologic saline was initiated using a three-way Foley catheter and continued for 3 to 4 hours in the recovery room. Irrigation was stopped once the urine was clear. Catheter removal was done on the third postoperative day. Patients were discharged the next day once they voided satisfactorily after catheter removal.
Statistical analysis
The sample size was calculated as 86 patients in each group, with significance level α = 0.05, β = 0.20, and a desired statistical power level of 80%. All data were entered into Microsoft Excel. Descriptive statistics were calculated for each analyzed variable and consisted of frequency, mean, percentage, and standard deviation. Statistical analysis was conducted using SPSS statistical software (SPSS, version 26.0, Chicago, IL).
Quantitative variables were analyzed using Student's t-test. Fisher's exact test was used when the expected frequency was <5. The chi-square test was performed to compare categorical data (comorbidities and complications, etc.) in both groups. A general linear model was applied to assess changes in postoperative parameters within a group as well as between groups. p-Value <0.05 was considered statistically significant.
Results
As depicted in Table 1, baseline characteristics and clinical parameters were comparable in both the HoLEP and BPEP groups (p > 0.05). Of the 190 enrolled patients, 172 completed the study protocol at the 36-month follow-up. Patients were initially evaluated in the outpatient department by a transabdominal ultrasound, but on the day of surgery, TRUS was performed to record precise PV in every patient.
Baseline Demographic and Clinical Characteristics
BPEP = bipolar plasmakinetic enucleation of the prostate; HoLEP = holmium laser enucleation of the prostate; IIEF = International Index of Erectile Function; IPSS = International Prostate Symptom Score; LUTS = lower urinary tract symptoms; PSA = prostate-specific antigen; PVR = postvoid residual; Qmax = maximum flow rate; QoL = quality of life; SD = standard deviation; TRUS = transrectal ultrasound.
The size of the prostate was comparable (p = 0.458) in both groups. Nearly half of the patients, in both groups, had one or more associated comorbidity. Baseline urinary parameters such as IPSS, Qmax, serum PSA levels, QoL, and PVR scores were comparable (p > 0.05) in both groups.
The total operative time (HoLEP: 30.91 ± 14.82; and BPEP: 41.63 ± 16.19 minutes; p = <0.05), enucleation time (HoLEP: 27.87 ± 13.18; and BPEP: 38.37 ± 14.55 minutes; p = <0.05), enucleation efficiency (HoLEP: 1.69 ± 0.28; and BPEP: 1.28 ± 0.06 g/min; p = <0.05), and drop in hemoglobin (HoLEP: 0.46 ± 0.23; and BPEP: 0.87 ± 0.26 g/dL; p = <0.01) were statistically significantly better in the HoLEP group. Bladder irrigation time, catheterization time, and hospital stay were similar in both groups (Table 2).
Perioperative Variables in Holmium Laser Enucleation of the Prostate and Bipolar Plasmakinetic Enucleation of the Prostate Groups
Transient urinary incontinence (<2 weeks) occurred in four (4.6%) patients in the BPEP group and in three (3.4%) in the HoLEP group. Only one BPEP group patient had persistent incontinence beyond 3 months. None of the patients in either group required blood transfusion. Prolonged hematuria needing bladder irrigation beyond 8 hours was observed in seven (8.1%) patients in the BPEP group, while only two (2.3%) in the HoLEP group. One patient from the BPEP group required cystoscopic clot evacuation. There was no incidence of transurethral resection syndrome (TUR syndrome) or bladder/ureteral orifice injury in either group.
Postoperative complications recorded in the study are outlined in Table 3. For stricture urethra, one HoLEP group patient needed cystoscopy and visual internal urethrotomy intervention, while two patients in each group were managed by urethral dilatation only. Two patients in each group who had bladder neck contracture required bladder neck incision. None of the patients needed a second-stage procedure for incomplete enucleation.
Perioperative Complications in Both Holmium Laser Enucleation of the Prostate and Bipolar Plasmakinetic Enucleation of the Prostate Groups
TUR syndrome = transurethral resection syndrome; UTI = urinary tract infection.
Pertinent clinical data at baseline and follow-up period/time points for both HoLEP and BPEP groups are outlined in Table 4. The IPSS, Qmax, PVR, and QoL scores for both patient groups showed significant (p < 0.05) improvement for as long as 3 years of follow-up (Fig. 2). No statistically significant differences were observed in IPSS, QoL, Qmax, and PVR scores between the two treatment groups (p > 0.05), confirming similar long-term efficacy in both groups. Serum PSA levels showed significant (p < 0.05) reduction at the 1-year follow-up in both groups.

Line diagram (2D) depicting baseline and follow-up data, comparing HoLEP and BPEP.
Clinical Data at Baseline and Follow-Up for Holmium Laser Enucleation of the Prostate and Bipolar Plasmakinetic Enucleation of the Prostate Groups
Discussion
BPH can lead to varying degrees of bladder outlet obstruction and eventually compromise the QoL of most patients. 12 In recent years, AEEP has shown superiority over standard resection techniques. Although the concept of transurethral enucleation was first proposed by Hiraoka in 1983, 13 the use of the holmium laser for enucleation was popularized by Gilling and colleagues in 1998. 3,4 Lasers have been used extensively for AEEP due to its precise cutting and excellent hemostasis. A recent large study (1476 patients) with an 18-year follow-up has strongly demonstrated the safety, efficacy, and durability of HoLEP. 14
AEEP can also be performed by nonlaser energy sources such as bipolar electrocautery. The European Association of Urology Guideline Panel for management of non-neurogenic male LUTS and benign prostatic obstruction (BPO) has proposed AEEP as the procedure of choice for large glands, irrespective of the energy source used. 15 This was mainly based on results of two meta-analyses involving randomized control trials (RCTs), which compared open prostatectomy with either HoLEP or bipolar enucleation of the prostate (BipoLEP). 16,17 Consequently, a laser-based treatment, HoLEP, and the electrocautery-based BipoLEP treatment are considered as viable options for management of BPO. 18
This randomized prospective study was planned to directly compare the two enucleation techniques, that is, HoLEP and BPEP. Three years of follow-up data present optimum parameters for assessing the durability of any surgical procedure. This study demonstrated that the midterm efficacy in both treatment groups was comparable, with no significant differences in the outcomes.
Most published studies have compared enucleation procedures with either bipolar or monopolar TURP, or open prostatectomy. There is scant literature that directly compares bipolar enucleation with holmium laser enucleation. Several RCTs have compared other laser energy sources such as the diode laser 19,20 (diode laser enucleation of the prostate, diode LEP) or thulium laser (ThuLEP) with bipolar enucleation of the prostate. 21 Diode LEP, ThuLEP, and PKEP were found to be valid treatment options for men with mild-to-moderately enlarged prostates. The patient outcomes and complication rates were comparable with other endoscopic BPH procedures.
Gilling and his group, the pioneers of HoLEP, were the first to compare the safety and efficacy of HoLEP with PKEP as early as 2006. 6 They used the Gyrus bipolar radiofrequency device with a finely coiled axipolar cystoscope electrode and found it to be technically feasible and safe. The only problem was that the plasmakinetic energy generated a lot of vaporization bubbles that obscured vision and prolonged the operative time. The authors considered the holmium laser as an optimal energy source for enucleation and bipolar energy a viable option for surgeons experienced with HoLEP.
Even our initial experience in 2008 with the plasmakinetic enucleation technique using a needle electrode was similar. Due to the problem of vaporization bubbles, we moved from needle electrode to button electrode. The sharp edge of the vaporizing button electrode could effectively cut the tissue and be used for mechanical enucleation as well as blunt dissection. The rounded electrode surface was used for coagulation and vaporization.
Giulianelli and colleagues in their single-center experience of treating 50 patients with B-TUEP using a button electrode and plasmakinetic energy found this technique to be safe and effective. 8 The results were maintained over a 5-year follow-up. Gu and colleagues, 22 in their meta-analysis, concluded that the early efficacy and safety profiles of bipolar and laser treatments are comparable. Patients treated with the laser had a lesser drop in hemoglobin (Hb), shorter catheter duration, and reduced hospital stay. However, the lower reduction in Hb with the laser did not translate into reduced transfusion requirement. Significant heterogeneity was also noted in the published studies on this topic.
A randomized controlled study conducted by Habib et al 9 compared HoLEP with BPEP for a large-volume BPH (>80 mL) with a 12-month follow-up. In their study, BPEP required a longer operative time and prolonged need for a catheter. In contrast, Pallauf and colleagues, 23 in their recent review article, found BipolEP to be 16.72 minutes faster than HoLEP, but the odds for blood transfusion were threefold higher. Our results are in line with most published literature and we also found the enucleation and operative times to be shorter in the HoLEP group (p < 0.05). 24
Recently, Boeri and his group from Italy 25 did a comparative study of HoLEP and B-TUEP in patients on anticoagulant or antiplatelet agents and concluded that both the procedures are safe in this select group of patients, with a slight increase in hospital stay and catheterization time in the B-TUEP group.
In the present study, 22 (25%) patients from the BPEP group and 26 (30%) patients from the HoLEP group were on antiplatelet or anticoagulant agents. Although comparison of this subgroup was beyond the scope of the present study, none of the patients in either group needed blood transfusion. Seven patients in the BPEP group did have prolonged hematuria requiring bladder irrigation beyond 8 hours.
Gilling, in his recent editorial, 26 stressed the importance of the pulsed nature of the holmium laser, which makes it a more versatile endoscopic tool. The plane of enucleation is easier to develop and follow, and visibility seems to be superior compared with other energy sources. Even in our study, we found dissection to be easier in the HoLEP group. Clinically insignificant capsular perforation was seen in three patients in the BPEP group and none in the HoLEP group. This may be due to higher depth of penetration of plasmakinetic energy and overdependence on mechanical force for enucleation during BPEP. Capsular perforations can be more frequent during the initial learning curve and in patients who have chronic prostatitis or multinodular adenomas. The pulsed holmium laser energy is more precise and less likely to cause capsular violation. This precision of the holmium laser is particularly useful in separating the adenoma at the antero-apical region and helps preserve continence. 27
In this study, the incidence of temporary stress urinary incontinence (<2 weeks) was similar for both the procedures. None of the patients were incontinent beyond 6 months. Modifications in the technique (en bloc enucleation) could reduce operation time and complications. Reduced resectoscope movement and smaller force during manipulation minimize urethral sphincter damage and prevent postoperative urinary incontinence. 28,29
The results of this study may not reflect the real-world scenario as all the procedures were done by a single surgeon with extensive experience in performing AEEP. Analysis of factors affecting the learning curve for bipolar enucleation was beyond the scope of our study. Based upon personal experience, we hypothesize that as finding proper planes for enucleation with mechanical force or plasmakinetic energy needs experience, the learning curve for bipolar enucleation may be steeper than for holmium laser enucleation. It is important to overcome the learning curve for enucleation using the bipolar button electrode to increase adoption of BPEP. The lower capital and maintenance costs of a bipolar generator are strong motivating factors for its more prevalent use. Furthermore, the same generator can be used to resect, vaporize, or enucleate the prostate adenoma. Properly designed prospective studies comparing the learning curves of HoLEP and BPEP should add to existing knowledge.
The versatility of the high-power holmium laser in urology is widely recognized, but higher initial capital investment precludes its use for enucleation procedures by many urologists. A cost analysis for both these enucleation techniques was beyond the scope of this study as it involves multiple complex factors. The results also signify that bipolar plasmakinetic energy (using the button electrode) is a viable alternative source that can be used for transurethral enucleation of the prostrate.
Conclusions
The holmium laser is a validated and versatile option for performing enucleation. Its efficacy and durability have been reconfirmed in many studies. Our study also documents the excellent safety profile and efficacy of HoLEP. However, BPEP has also been proven to be safe and effective, as well as durable in the medium term.
There is no convincing evidence on the superiority of one energy source over the other in experienced hands. Multicentric trials, with long-term prospective data, are required to establish the equivalence or superiority of one energy source over another for enucleation of prostatic adenoma.
Footnotes
Acknowledgments
The authors are grateful to Dr. Chetan Popat, MD, Tutor in the Department of Community Medicine, Medical College, Vadodara, Gujarat, India, for his guidance and assistance in statistical analysis of data and Dr. Manasi Parikh, MBBS, MD, Clinical Instructor, Boston University, USA, for her help in manuscript editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.