
Abstract
Introduction and Objective:
With introduction of the da Vinci single-port (SP) system, we evaluated which multiport (MP) robotic skills are naturally transferable to the SP platform.
Methods:
Three groups of urologists: Group 1 (5 inexperienced in MP and SP), Group 2 (5 experienced in MP without SP experience), and Group 3 (2 experienced in both MP and SP) were recruited to complete a validated urethrovesical anastomosis simulation using MP followed by SP robots. Performance was graded using both GEARS and RACE scales. Subjective cognitive load measurements (Surg-TLX and difficulty ratings [/20] of instrument collisions camera and EndoWrist movement) were collected.
Results:
GEARS and RACE scores for Groups 1 and 3 were maintained on switching from MP to SP (Group 3 scored significantly higher on both systems). Surg-TLX and difficulty scores were also maintained for both groups on switching from MP and SP except for a significant increase in SP camera movement (+7.2, p = 0.03) in Group 1 compared to Group 3 that maintained low scores on both. Group 2 demonstrated significant lower GEARS (−2.9, p = 0.047) and RACE (−5.1, p = 0.011) scores on SP vs MP. On subanalysis, GEARS subscores for force sensitivity and robotic control (−0.7, p = 0.04; −0.9, p = 0.02) and RACE subscores for needle entry, needle driving, and tissue approximation (−0.9, p = 0.01; −1.0, p = 0.02; −1.0, p < 0.01) significantly decreased. GEARS (depth perception, bimanual dexterity, and efficiency) and RACE subscores (needle positioning and suture placement) were maintained. All participants scored significantly lower in knot tying on the SP robot (−1.0, p = 0.03; −1.2, p = 0.02, respectively). Group 2 reported higher Surg-TLX (+13 pts, p = 0.015) and difficulty ratings on SP vs MP (+11.8, p < 0.01; +13.6, p < 0.01; +14 pts, p < 0.01).
Conclusions:
The partial skill transference across robots raises the question regarding SP-specific training for urologists proficient in MP. Novices maintained difficulty scores and cognitive load across platforms, suggesting that concurrent SP and MP training may be preferred.
Introduction
Robotic laparoendoscopic single-site surgery was first described in 2008 performed through a single abdominal incision to expedite postoperative recovery. 1 Early attempts at modifying the docking procedure of the da Vinci Xi or Si, where all instruments are inserted through a single incision, were hindered with significant external arm clashing and limited internal mobility. 2 In 2018, the da Vinci single-port (SP) Surgical System (Intuitive Surgical, Sunnyvale, CA), designed specifically for SP surgery, was approved by the FDA for urologic use. This system consists of a single robotic arm that independently controls an 8 mm articulating camera and three strategically placed 6 mm robotic instruments, all of which are introduced through a single 2.5 cm multichannel port eliminating external arm clashing. The unique double-joint instrument design and 7-degree of freedom of movement allows for intracorporeal triangulation.
Since approval, multiple studies have demonstrated effective use of the da Vinci SP for prostatectomy, 3 nephrectomy, 4 and partial nephrectomy. 5
The introduction of the da Vinci S in the early 2000's prompted research into skill transfer from minimally invasive laparoscopic approaches to robotic surgery given the difference in technology. 6,7 Similarly, the unique nature of the SP platform, lack of information regarding natural transfer of skill, and increased interest in utilization of the SP platform by robotic surgeons (including those with vast multiport [MP] experience) warrant a need for investigating skills and the transfer of skills across both platforms to ensure a safe and smooth transition and define training needs.
Although the Xi and SP share similar surgeon consoles, they behave differently due to the SP's single pivot point approach, presence of an extra clutch (to control the camera angle independently), movement of the robotic arms as a single unit, close proximity of the robotic arms (increasing the likelihood of internal collisions), and the absence of EndoWrist instruments. We aim to evaluate in a realistic simulated environment whether skills developed during MP robotic surgery are directly applicable and/or transferable to SP surgery in three groups of urologists that vastly differ in their experience using both robotic platforms.
Methods
Participants
Within the Department of Urology at the University of Rochester Medical Center, five residents with limited robotic MP cases (<10) and no prior SP experience were recruited into Group 1. Five urology surgeons with >5-years of experience and >250 cases of robotic MP cases but with no SP experience were recruited into Group 2. Five urologic robotic surgeons with similar experience in MP (>250 cases) as well as SP (>50 cases) were recruited into Group 3. This categorization was based on data defining the learning curve for RARP. 8
Model
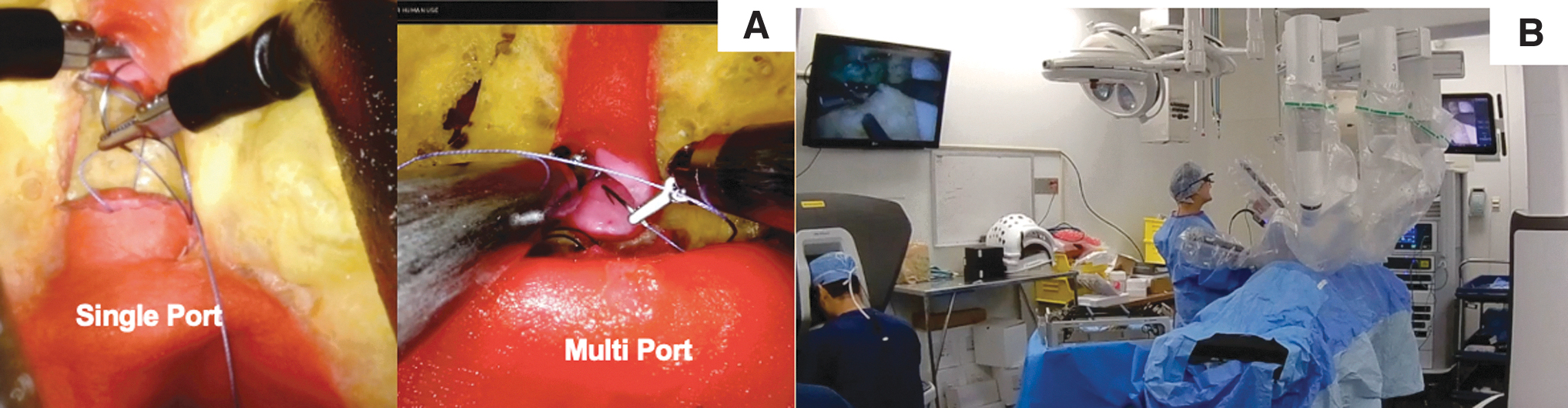
A partial task trainer was designed by isolating the urethrovesical anastomosis (UVA) portion of a previously validated robot-assisted radical prostatectomy hydrogel model fabricated by injecting a hydrogel into 3D printed casts to replicate realistic tissue texture. 9 The simulation model consisted of a bladder, urethra, and surrounding connective tissue anatomically aligned within a 3D printed pelvis (Fig. 1A). Notably, the prostatic urethra was absent at the start of the procedure. The model was placed on an angled base to mimic patient Trendelenburg positioning and secured inside an abdominal trainer to replicate operative setup (Fig. 1B). An assistant was available during the simulations to only pass Vicryl sutures and cut suture.
Study design
Participants first completed a UVA simulation using the MP robot and then repeated it within 2 weeks using the SP robot. Review of the steps of UVA using a prerecorded narrated video was given to Group 1 due to their limited experience. Groups 1 and 2 (limited exposure to SP) completed an online module on the manufacturers' website and oriented to the differences in surgeon consoles and movement types at the start of the SP simulation by a urologist who regularly utilizes the SP robot.
To ensure familiarity with the model, all groups received an orientation to the model before the start of the simulation and were allowed to practice on a separate UVA model without feedback before completing the simulated UVA that was to be graded. For each simulation (MP and SP), the endoscopic video feed was recorded, after which each surgeon completed a subjective cognitive load scale (SURG-TLX/100) 10 and rated the difficulty of several categories, including camera movement (/20), EndoWrist movement (/20), and avoiding instrument collisions (/20).
Data analysis
Two experienced reviewers, blinded on surgeon experience, randomly reviewed the recorded MP or SP intraoperative videos and assigned GEARS 11 and RACE 12,13 scores for each attempt. A subjective measure of cognitive load Surg-TLX was correlated with difficulty ratings specific to robotic surgery. All metrics were compared within and between MP and SP simulations for each group.
Statistical analysis
Descriptive statistics and t-tests were completed using SPSS. Inter-rater reliability was calculated to confirm agreement between reviewers. Since no participants were given feedback during the actual task, a score of 5 was assigned to the GEARS subscore “autonomy.”
Results
GEARS and RACE scores
When using the MP robot, surgeons with >250 MP cases (Groups 2 and 3) achieved mean scores above the published benchmark to identify expert proficiency (>25) for GEARS [10] (27 ± 3.2, 27 ± 3.6) and RACE scores (26.9 ± 3.8, 25.7 ± 5.9) (Fig. 2). 12 When using the SP robot, surgeons with >250 MP cases, Group 3 achieved a not significant higher mean score for GEARS (25, 24.1 p = 0.65) and RACE scores (26.9, 25.7 p = 0.38). Group 1 achieved significantly less mean GEARS (17.3 ± 3.62) and RACE (15.9 ± 2.33) scores failing to reach the reported expert benchmark (Table 1).

GEARS and RACE scores comparing mean participant scores in Groups 1, 2, and 3 comparing multiport and single-port performances. GEARS = Global Evaluative Assessment of Robotic Skills; RACE = robotic anastomosis competency evaluation. Color images are available online.
Surg-TLX, Difficulty, GEARS, and RACE Evaluations in Groups 1, 2, and 3 Comparing Multiport and Single-Port Performances
Denotes significance (p ≤ 0.05) between MP and SP.
MP = multiport; RACE = robotic anastomosis competency evaluation; SP = single-port.
Group 1 (Novices in both MP and SP)
Group 1 mean performance ratings of GEARS and RACE remained consistently low without significant difference across MP and SP platforms. On subscore analysis, the only significant decrease occurred for knot tying RACE subscore for SP vs MP performance (2.1 vs 3.3, −1.2 pts). Surg-TLX and difficulty scores were of the highest reported scores, but without significant differences across MP vs SP platforms (31.6 vs 35.6). Participants reported higher mean difficulty ratings (/20) during SP simulations compared to MP simulations for EndoWrist manipulation (15.2 vs 17, +1.8), collision avoidance (13 vs 18.6 + 5.6), and camera movement (8.2 vs 15.4, +7.2 pts). The latter (camera movement) demonstrated the most significant difference for SP vs MP performances.
Group 2 (MP experts without SP experience)
Group 2's performance ratings significantly decreased during SP compared to MP, measured by GEARS (27 vs 24.1, −2.9) and RACE (26.9 vs 21.8, −5.1) scores. On subanalysis, mean GEARS subscores for force sensitivity (4.4 vs 3.7, −0.7) and robotic control (4.4 vs 3.5, −0.9) significantly decreased during SP performance, while subscores of depth perception (4.5 vs 4.5, −0), bimanual dexterity (4.5 vs 3.8, −0.7), and efficiency (4.2 vs 3.6, −0.6) were maintained. Mean RACE subscores of needle entry (4.6 vs 3.7, −0.9), needle driving (4.3 vs 3.3, −1), tissue approximation (4.7 vs 3.7, −1), and knot tying (4.7 vs 3.7, −1) significantly decreased during SP performance, while subscores of needle positioning (4.5 vs 4.0, −0.5) and suture placement (4.1 vs 3.4, −0.7) were maintained.
Mean Surg-TLX scores were lower than those reported in Group 1, but higher than Group 3. During SP simulations, mean Surg-TLX (26.1 vs 13.1, +13 pts) and difficulty ratings for camera movement (1.4 vs 13.2, +11.8 pts), EndoWrist movement (1.8 vs 15.4, +13.6 pts), and avoiding instrument collisions (1.8 vs 15.8, +14 pts) were significantly higher compared to MP platform simulations.
Group 3 (MP experts with SP experience)
Group 3 maintained higher mean performance across both SP and MP platforms evaluated by GEARS (27 vs 25, −2 pts) and RACE (25.7 vs 23.7, −2 pts) scores with no significant differences in any subscores. Mean Surg-TLX and all difficulty scores were the lowest reported among the Groups. When comparing SP to MP simulation performances, a nonsignificant increase was reported on Surg-TLX (9.6 vs 19, +9.4 pts) and all difficulty scores during SP performances.
Discussion
In this study, we attempted to identify inherent differences in the skills necessary to execute a complex suturing task when utilizing an established vs a newly adopted robotic platform. Utilizing a validated partial task trainer that replicates the UVA step of the radical prostatectomy procedure, surgeons inexperienced on both systems (Group 1) performed poorly and were outperformed by surgeons experienced on both MP and SP systems as expected, proving the adequacy of the study design. However, surgeons experienced in MP approaches without any SP experience (Group 2) provided the most accurate insight in transferability of skills between systems. Urologists in this group were able to effectively transfer technical skills in depth perception, bimanual dexterity, efficiency, needle positioning, and suture placement naturally, but did not demonstrate the same natural transference for force sensitivity, robotic control, needle entry, needle driving, tissue approximation, and knot tying from MP to SP platforms.
Furthermore, despite the higher mean SP performance scores in Group 2 vs Group 1, the perceived difficulty ratings were comparable among both groups (Surg-TLX 35.6 vs 26.1 p = >0.001). This suggests that partial, not complete skill transfer occurs from MP to SP in expert surgeons. This also suggests that trainees with less robotic experience have the mental capacity to concurrently learn both approaches simultaneously as they are not required to struggle with sifting from a learned skill to a newly adopted skill. The differences in the functionality of the two types of robots require adaptation of surgical technique, and therefore the development of new skills specific to the platform. 3
The SP robotic instruments provide less torque and grasping strength, which can explain the overcompensation seen within the inexperienced surgeons, leading to low scores on force control. The replacement of the MP EndoWrist instruments' capability decreases the range of motion and affects needle driving due to the loss of the “elbow” movement. However, the SP camera is multijointed and can be articulated like the instruments, allowing for increased maneuverability and complexity, which attempts to make of for the loss of mobility. This difference in robotic maneuverability is seen by Group 1 who reported the camera movement as being significantly more difficult. The reported difficulty indicates the need for further camera training as the camera control is one of the most novel aspects of the SP platform.
Training for minimal invasive surgery has progressed over the years as laparoscopic surgeons have adopted robotic surgery. Currently standard training to use the SP system consists of a half-day dry laboratory and full-day wet laboratory session. Continual practice after this point is limited to SP Virtual Reality (VR) simulation modules in SimNow (Intuitive Surgical), an add-on to the surgeon console that allows completion of virtual-reality exercises. Exercises include Camera pose match (participant matches the camera pose to one shown in the navigator), Ring obstacle course (participant navigates rings along a rail with various obstacles), and Workbot transport (participant retrieves “workbots” from glass modules and load them to a train transport).
Unfortunately, the current library of exercises is quite limited and does not include any SP suturing tasks or procedural simulations. This leads to limited opportunity to improve needle entry, needle driving, and knot tying skills, which are the specific skills that did not transfer from MP to SP. The exercise “Camera Pose Match” is meant to help with learning camera movement, “Ring Obstacle” is meant to help with arm movement and counteract instrument collisions, and “Workbot Transport” helps put these skills together, which may help to learn robotic control, but nothing specifically focuses on force control. In addition, these exercises provide no insight in the difference required in surgical approaches. While these exercises present an introduction to the basics, they are far from extensive enough to prepare for a task such as UVA or to a complete robotic surgical procedure.
Studies evaluating the SP SimNow are at their infancy; however, even existing multiport VR robotic simulators lack real-life characteristics and realistic haptic feedback, 14,15 limiting their use to basic psychomotor exercises. Furthermore, the automated metrics generated from VR simulators lack the procedural relevance that is required for effective training. 16 –18 A notable study demonstrated a significant association between clinical performance measured by GEARS scores graded videos of endopelvic fascia dissection during a robotic radical prostatectomy surgery and simulator scores that included performance on eight VR da Vinci surgical skills simulator tasks (q = 0.805, p < 0.001) and four inanimate Fundamentals of Robotic Surgery tasks (q = 0.833, p < 0.001). 19 Each individual task and daVinci surgical skills simulator task score also demonstrated a significant correlation with intraoperative performance, with the exception of Energy Switcher 1 exercise (p = 0.063).
However, most studies on existing VR systems have found no significant difference in performance scores between VR-trained and untrained groups. A study examined the effect of a robotic simulator curriculum on the ability of trainees to perform a suturing task on a live porcine model and found that there was no difference in live performance for the simulation based training group compared with the group undergoing a standard robotic system orientation, 20 another found no difference in live patient hysterectomy performance posttraining. 21
Others, including an international randomized controlled trial across 10 countries, found that simulation urology training did not statistically improve initial learning curve (measured as surgeon's general proficiency). 22 Also, VR metrics often fail at distinguishing competent from noncompetent surgeons. 23,24 Significant differences were only found when novice cohorts consisted of trainees with no robotic experience rather than learners with minimal surgical experience to be considered proficient. 20,25 Others found significant differences but only in post hoc comparisons after combining intermediate and expert surgeons against beginners. 26
Several centers of excellence have created an initial body of clinical evidence for the SP system. While these centers presently represent high-volume clinical settings with experienced minimally invasive surgeons, this initial development mirrors that of the MP platforms. Generally similar perioperative outcomes, intraoperative complication rates, and operative times to comparable MP operations were reported in reconstructive urology, 27,28 radical cystectomy, 29 and radical prostatectomy. 30,31 While these represent a heterogenous range of operations from experienced robotic surgeons with small patient sample sizes, it appears that most complex robotic operations may be safely performed with the SP platform. However, long-term oncologic results will require additional follow-up beyond these initial reported case series.
Of note, positive surgical margins for prostatectomy were noted to range between 20% and 33% in initial case series, which may reflect the initial learning curve for this technology. 30 –32 One potential concern of the SP platform is a perceived increase in surgical complexity, as some authors have noted an increased number of steps and operative time in donor nephrectomy despite improved visualization over their standard single-site laparoscopic nephrectomy technique. 33 These studies provide some evidence, ultimately comparative studies will be required to evaluate perioperative and long-term outcomes between SP and MP platforms.
This study is not without its limitations. There was a limited availability of urologists with experience in both MP and SP platforms at our institution where performance of a subgroup may have been highly influenced by their performance. However, using this limited number, our study was still capable of identifying several skill sets that are not naturally transferred when experts are shifting from one platform to the other that are essential to development of specific training resources. Our results were based on an evaluation of a complex suturing task, which may not representative of a comprehensive robotic skill assessment and therefore a similar analysis for a range of full procedural simulation to generalize our results for the transferability of skills.
Conclusions
For experts proficient in MP, specific SP training should be developed due to partial skill transference. Cognitive load remained steady for novices across robots, suggesting that concurrent SP and MP training may be possible. Training resources for SP robots need to be expanded before training curricula can be implemented.
Footnotes
Authors' Contributions
A.G was involved in study design, data collection, data analysis, and article writing/editing. N.S and P.S were involved in study design, data collection, data analysis, and article writing/editing. T.H., A.S., K.Y., K.D., E.E., W.T., J.B., and H.R. were involved in data analysis. N.K. and J.J. were involved in study design and article review.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this article.