
Abstract
Introduction:
Radical nephroureterectomy with bladder cuff excision (BCE) is the standard of care all high-risk upper tract urothelial carcinomas. With continued advancements, robot-assisted segmental ureteral resection can be employed for ureteral tumors for ipsilateral renal preservation. Herein, we are presenting our experience of different techniques classified by the affected ureteral segment, along with perioperative and intermediate to long-term functional and oncologic outcomes.
Methods:
From January 2008 to June 2021, a total of 17 patients underwent robot-assisted renal preserving excisional procedures for ureteral tumors. We collected and analyzed baseline, perioperative and follow-up outcomes parameters from our prospectively maintained institutional database. Eleven patients underwent segmental ureterectomy (SU) with BCE and ureteroneocystostomy with psoas hitch, five patients underwent SU with ureteroureteral anastomosis with/without psoas hitch, and one patient underwent ileal patch interposition after segmental ureteral excision.
Results:
Although majority of the patients had inconclusive or low-grade pathology on initial ureteroscopic biopsies, 73.33% of the patients were found to have high-grade tumors on final pathology report. Median tumor size was 2.7 cm (1–5.5 cm), and the median operative duration was 193 minutes (142–400 minutes). None of the procedures required conversion to open. Overall, only one patient (5.9%) had Clavien–Dindo grade ≥ III complication (pelvic abscess). At median follow-up of 41 months (7–156 months), four patients (26.67%) developed urothelial recurrences out of which only one patient required nephroureterectomy. Overall survival and nephroureterectomy-free survival were 86.67% and 92.31%, respectively.
Conclusions:
Our study provides a comprehensive review of various surgical approaches of robot-assisted renal sparing management for ureteral tumors. These procedures are surgically safe, feasible, and effective with satisfactory oncologic outcomes at intermediate to long-term follow-up. These procedures may be safely employed in select patients with a localized ureteral tumor to salvage the ipsilateral kidney and estimated glomerular filtration rate.
Introduction
Radical nephroureterectomy (RNU) with bladder cuff excision (BCE) is the standard of care for all high-risk upper tract urothelial carcinomas (UTUC) and in select cases of high-volume low-grade urothelial ureteral tumors. But the need to preserve kidney function may influence the decision to take a nephron sparing approach. Patient selection for nephron sparing procedures requires balancing the benefits of maintaining renal function with long-term oncologic outcomes. However, recent studies have highlighted the feasibility of segmental ureterectomy (SU) for localized ureteral tumors, as an alternative to RNU, with acceptable functional and oncologic outcomes. 1 –6
Previously published literature on robot-assisted SU, however, lacked long-term follow-up, been isolated cases, or focused only on distal ureter. This investigation examines a series of proximal and distal ureteral neoplasms managed with different surgical techniques, as one technique does not fit all. We present our experience of various robot-assisted multidimensional reconstructive options after SU for ureteral tumors with a focus on perioperative, functional, and oncologic outcomes.
Materials and Methods
We conducted a retrospective query of our institutional review board-approved robotic surgical database for ureteral surgeries performed for malignancy. From November 2008 to June 2021, a total of 17 patients underwent robot-assisted excisional procedures for ureteral tumors at our center. All procedures were performed using the da Vinci Surgical System by senior author (A.K.H.). We collected and analyzed baseline, perioperative, and follow-up outcome parameters. However, regardless of the surgical procedure adopted, a complete preoperative evaluation is recommended with CT urogram, and if indicated a radioisotope renogram to assess ipsilateral function and/or intraoperative fluoroscopic navigation or molecular imaging using indocyanine green intraluminally or intravascularly. Three-dimensional reconstruction is also helpful in delineating spatial anatomy.
Reconstructive options after SU
Eleven patients (67.4%) underwent SU with complete BCE and ureteroneocystostomy with psoas hitch, five patients (29.4%) underwent SU with ureteroureteral anastomosis with/without psoas hitch, and one patient (5.9%) underwent ileal segment interposition after segmental ureteral excision. All patients also underwent regional lymph node dissection. Double-J stent was placed in all patients at the time of surgery and was removed at ∼4 to 6 weeks postoperatively.
Technique for accessing pelvic ureter
Pelvic ureter is most reliably accessed in low lithotomy with steep Trendelenburg position, similar to robotic prostatectomy. After creating the pneumoperitoneum, port placement is done using the established standard principles. 7 Port placement can be tailored based on the location of the pathology.
Ureteroneocystostomy
The ureter is identified at the level of crossing of iliac vessels and is completely mobilized till the vesicoureteral junction. The medial umbilical ligament (superior vesical artery) is encountered while dissecting the ureter and is an important landmark. As we proceed distally, the ureter should be clipped and divided immediately proximal to the diseased segment (also ensuring adequate margin) during mobilization to prevent tumor spillage proximally. After identification, the bladder cuff is excised with at least 5 mm margin circumferentially and repaired after taking stay sutures and completing a two-layered bladder closure with absorbable suture. The specimen is then collected with an Endo-catch bag. As needed, the contralateral medial umbilical ligament maybe divided to adequately mobilize the bladder, thus allowing for reduced tension on the ipsilateral side, which is particularly important while performing ureteroneocystostomy with psoas hitch.
To perform the psoas hitch, 1-0 Polydioxanone sutures or ethibond are placed 1 to 2 cm apart to fix the ipsilateral bladder dome with the psoas muscle/tendon, while taking care to identify and preserve the genitofemoral nerve. Another tension-releasing suture may be applied to the periureteral tissue and psoas muscle. We prefer a nontunneled extravesical ureterovesical anastomosis to the bladder dome, on the ipsilateral side, after adequately spatulating the ureter. This is done using 4-0 or 5-0 Monocryl running suture in two hemi-circles in a tension-free manner. Double-J stent is placed after completing one hemi-circle of ureterovesical anastomosis in a retrograde manner intracorporeally.
Technique for accessing proximal ureter
The location and length of the involved ureteral segment drives the approach used to access the proximal ureter. For more distally located tumors, access is preferred as explained earlier. For proximal tumors, a full flank position and robotic port configuration as reported by us previously is preferable. 6,7 Ipsilateral colon is mobilized, and the dissection is continued medially until the ureter is identified; if a percutaneous nephrostomy tube is present then indocyanine green can be utilized. After identification of the diseased segment, early clipping is completed both proximally and distally. Intraoperative frozen sections can assess if adequate margins are achieved after SU.
Ureteroureterostomy
The ureteral ends are spatulated and end-to-end anastomosis is performed using 5-0 Monocryl suture after adequate mobilization of the ureter (both proximal and distal) with traction sutures at 6 and 12 o’ clock. We prefer the placement of pure robotic antegrade intracorporeal Double-J stent, once after completion of the back wall of the anastomosis. A Double-J stent loaded over the guidewire with floppy end emerging through the end hole is advanced through the assistant port and distally toward the bladder. Efflux of urine through the side holes ensures adequate placement of the stent into the bladder. At this point the guidewire is removed and loaded back through the side hole of the stent, which is then advanced proximally toward the kidney. Anchoring the stent with the third robotic arm may aid in this step to prevent displacement.
Ileal patch (a single anecdotal case report)
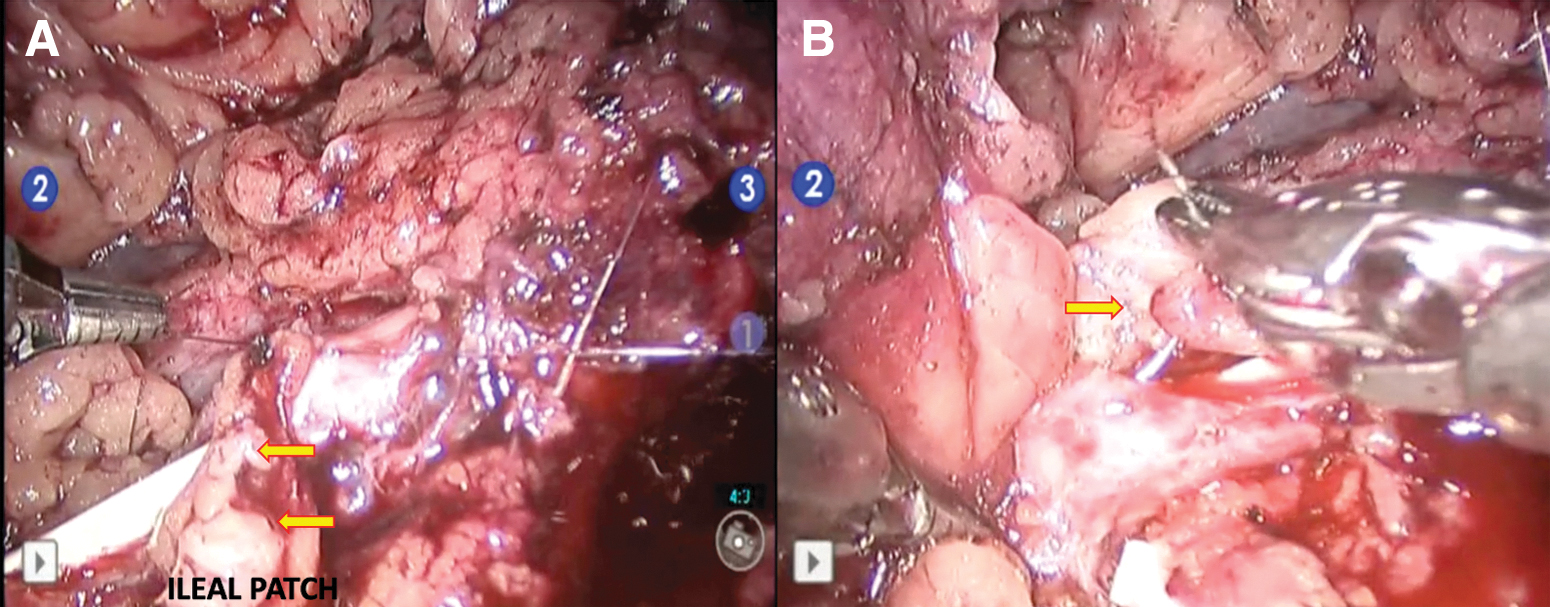
A 40-year-old female patient with stage IIIC endometrioid adenocarcinoma was found to have low-grade papillary urothelial carcinoma in the proximal ureter. She underwent robot-assisted SU to preserve the kidney given the patient's poor baseline renal function and the need to undergo systemic chemotherapy for her gynecologic malignancy. Retrograde pyelogram before surgery demonstrated a 3 cm segment of left proximal ureter affected by tumor (Fig. 1). After excision of the diseased segment using the technique as outlined earlier, a small defect (0.5 cm) was observed while performing tension-free anastomosis. After placing the Double-J stent as outlined earlier, the novel solution to this challenging scenario was to use a wedge of ileum to patch the defect (Fig. 2). Postoperatively, the patient experienced full return of bowel function and no evidence of urine leak.

Baseline and perioperative variables
Variables such as age, gender, baseline creatinine (with estimated glomerular filtration rate [eGFR]), Charlson comorbidity index, body mass index, symptoms, smoking status, the presence of hydronephrosis on preoperative imaging, tumor location, tumor size, and pathology at ureteroscopic biopsy were noted. Perioperative parameters such as operative duration, estimated blood loss, length of hospital stay, and final pathologic analysis were also recorded. Thirty-day postoperative complications were noted and classified, based on the Clavien–Dindo classification.
Follow-up
Patients were followed up at 3 months, 6 months, and then annually with symptom assessment, clinical examination, creatinine (eGFR), cystoscopy, conventional imaging (CT or MRI) and ureteroscopy (on a case-by-case basis).
Statistical analysis
Descriptive statistics were used to summarize the data set. Mean, median, and ranges are reported for continuous variables, whereas proportions and frequencies are reported for categorical variables.
Results
Categorical baseline variables are depicted in Table 1. Preoperatively, most of the patients either had low-grade (n = 8) or inconclusive findings (n = 4) on initial ureteroscopic biopsy with majority of the tumors located in the distal ureter (77.78%). The most common symptom at presentation was flank pain (55.6%) followed by hematuria (27.8%). Other baseline, perioperative, and follow-up continuous variables are depicted in Table 2.
Baseline Variables
BCE = bladder cuff excision; HG = high grade; LG = low grade; SU = segmental ureterectomy; UC = urothelial carcinoma.
Other Baseline Variables, Perioperative, and Follow-Up Outcomes
BMI = body mass index; CCI = Charlson comorbidity index; eGFR = estimated glomerular filtration rate; SD = standard deviation.
Complications
No case required conversion to open surgery and only one patient developed Clavien–Dindo ≥ III complication (pelvic abscess) postoperatively (Table 3), which required percutaneous drain placement under local anesthesia. One patient had symptomatic culture proven urinary tract infection, which required antibiotics, and two other patients had self-reported low-grade fever after discharge, which was managed with antipyretics.
Complications (Clavien–Dindo Grading)
Pathologic findings of surgical specimen
Two patients were found to have nonurothelial pathologies, of which one patient had metastatic clear cell carcinoma (primary lesion in the contralateral kidney, subsequently developed spinal metastasis; received ipilimumab with nivolumab, currently off immunotherapy because of toxicity) and the other patient had Hodgkin's lymphoma. Rest of 15 patients had UTUC on final pathologic analysis (Table 4) and 73.33% of these patients were found to be harboring high-grade disease including 5 patients who reportedly had ≥ T2 disease. One patient was also found to have lymph node metastasis. None of these patients were found to have positive surgical margins.
Preoperative and Final Pathology of the Surgical Specimen
AE = anti-cytokeratin antibodies; BCG = Bacillus Calmette-Guerin; CIS = carcinoma in situ; RCC = renal-cell carcinoma; RNU = radical nephroureterectomy; UTUC = upper tract urothelial carcinoma.
Functional and oncologic outcomes
The average change in eGFR of our patients with UTUC managed with renal sparing procedures (after excluding deceased patients) was found to be 10.4 ± 8.14 mL/min/1.73 m2 (preoperatively and on follow-up: 56.06 ± 10.40 and 47.7 ± 9.83 mL/min/1.73 m2, respectively). Interestingly, a significant drop in eGFR was noticed in these patients (p = 0.032). Stratification of this patient cohort based on chronic kidney disease stages at baseline and at follow-up have been highlighted in Table 5.
Stratification of Study Cohort Based on Chronic Kidney Disease Stages (Patients with Upper Tract Urothelial Carcinoma on Final Pathology)
On follow-up, two patients with UTUC in their final pathology analysis died secondary to nonurothelial carcinoma-related causes. One patient died secondary to metastatic endometrioid adenocarcinoma and other because of medical comorbidities. At median follow-up of 41 months (7–156), the overall survival of our study cohort is 86.67% (after excluding patients with nonurothelial malignancy on final pathologic analysis). Four patients (26.67%) developed urothelial recurrences, including two patients who developed ipsilateral upper tract recurrences on follow-up, of which one patient received definitive nephroureterectomy.
The other patient was found to have upper tract along with bladder recurrence and after initial endoscopic management followed by intravesical Bacillus Calmette-Guerin (lost to follow-up for >2 years; managed at a different facility), subsequently developed pulmonary metastasis, and received pembrolizumab, currently on enfortumab. The overall nephroureterectomy-free survival is 92.31% in patients with urothelial malignancy. The other two patients with bladder recurrences were managed by transurethral resection and intravesical therapy protocol, as their disease was nonmuscle invasive.
Discussion
There is growing body of evidence in support of SU for ureteral tumors, even in high-risk urothelial carcinoma. 1 –6 A number of studies have found no differences in the oncologic outcomes of SU when compared with RNU in appropriately selected patient populations. 1 –5 With the evolution of robotic surgery, and the obvious advantages of a minimally invasive approach, robot-assisted management of UTUC is gradually emerging as the standard of care. 7,8 With continued advancements, robot-assisted SU can be employed for ureteral tumors for renal preservation. We have previously published our initial experience with robot-assisted ureteral reconstruction in patients with ureteral tumors. 9
In this study, we are reporting our most updated series of patients with isolated ureteral tumors who were managed exclusively with robot-assisted reconstructive approaches after SU. We found that robot-assisted renal-sparing management for ureteral tumors is surgically feasible with several reconstructive options based on tumor location. Majority of the patients (64.7%) in our study cohort underwent distal ureterectomy (with BCE) and ureteroneocystostomy with psoas hitch. We found excellent nephroureterectomy-free and overall survival in our study cohort. Table 6 summarizes the results of previously published studies focused on robot-assisted SU (ureteral reimplantation and ureteroureteral anastomosis).
Previously Published Studies on Robot-Assisted Segmental Ureterectomy
Upper tract urothelial carcinoma.
High grade.
Low grade.
Carcinoma in situ.
NA = not available.
In the current cohort, although the majority of the ureteroscopic biopsies were either inconclusive or low grade (Table 4), final pathologic analysis suggested significant discordance between the initial and final pathology reports as 73.33% of our cases ultimately were found to have high-grade pathology. This highlights the well-known limitation of ureteroscopic biopsies and illustrates that the ureteroscopic biopsy findings should be approached with caution. The functional and oncologic outcomes despite high-grade final pathology in our study encourages to salvage ipsilateral kidney. While considering SU, a close review of cross-sectional imaging, ureteroscopic biopsy findings, and patient's factors with a shared decision-making process are important and can be employed in appropriately selected patients with isolated ureteral tumors.
Overall, the complication rate of our study cohort was 23.5%. Only one patient had Clavien–Dindo grade IIIa complication (pelvic abscess). Palagonia et al recently reported their experience with robot-assisted SU with psoas hitch ureteral reimplantation in 11 patients. They reported an overall complication rate of 36.4% including one patient who had grade III complication. 18 Previously, Campi et al reported a significantly higher overall complication rate (53.3%) in their multi-institutional analysis; 15 were in the robotic SU group of which 2 developed a grade III complication. 17
Our median follow-up was 41 months (range 7–156 months). Overall, four urothelial recurrences (26.67%) were found, two in the bladder and two at the renal pelvis of ipsilateral kidney (including one patient with both bladder and upper tract recurrence). Only one patient received nephroureterectomy and the other patient developed metastatic disease. Palagonia et al reported four (36.4%) recurrences at median follow-up of 25.5 months (12–53 months); three of which were intravesical. 18 Conversely, Campi et al reported a total of seven (46.67%) recurrences (four intravesical and three ipsilateral upper tract) in their multi-institutional cohort at median follow-up of 21 months (14–38 months). 17 Two patients required salvage open RNU in their study.
These findings need to be highlighted as only 33.33% patients in our study cohort had ≥ T2 disease on final pathology analysis of SU surgical specimen, whereas the study by Palagonia et al reported 27.27% patients with ≥ T2 disease. In their multi-institutional analysis, Campi et al reported a significantly higher number of patients with ≥ T2 disease (66.67%). In our study, a significant decline in eGFR was noted (p = 0.032), despite the nephron sparing approach, perhaps because of low eGFR at baseline, advancing age, and medical comorbidities, which is an indirect testimony of medical reasons. Our decision to salvage the ipsilateral kidney was driven by these factors. In contrast, a significantly higher drop in eGFR would have been expected if these patients were subjected to RNU.
Our study of robot-assisted kidney sparing approaches reports the longest follow-up ever reported after SU classified by the affected ureteral segment. We highlight our techniques to ensure tension-free ureteral reconstruction as it applies to individual ureteral segments and our experience with a unique case in which an ileal patch was used to bridge a significant defect. Our study is limited in its retrospective nature and small sample size as SU is likely underutilized in the general population and only employed in rare cases requiring renal sparing measures. An additional limitation is the heterogenous nature of the data set in terms of reconstructive methods. Given the individualized approach required to manage each case, our study provides a realistic and comprehensive review of the various surgical approaches, as the feasibility of one reconstructive option prevails over the other, based on the tumor location.
Conclusions
Robot-assisted renal sparing management for ureteral tumors is surgically safe, feasible, and effective with several surgical options based on the tumor location. To execute desired technique, multimodal imaging is imperative to precisely assess location and ipsilateral function. Our series demonstrate satisfactory oncologic outcome at intermediate to long-term follow-up. These surgical procedures may be considered in the management of localized ureteral malignancy to salvage the ipsilateral kidney as a patient's tailored approach with shared decision-making process taking all factors into consideration.
Footnotes
Authors' Contributions
Methodology, data collection, formal analysis, investigation, and writing—original draft by S.S. Investigation, data collection, and writing—review and editing by V.L. Writing—review and editing by R.A.P. Conceptualization, methodology, supervision, writing—assisting in original draft, review, and editing by A.K.H. (senior surgeon)
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received for this article.