
Abstract
Purpose:
We proposed a new technique, single-position complete retroperitoneoscopic radical nephroureterectomy (SCRNU), which proved to be efficient for the treatment of upper urinary tract urothelial carcinoma (UTUC).
Materials and Methods:
In this study, we retrospectively evaluated 86 patients diagnosed with UTUC at our hospital from June 2013 to June 2021. The patients who underwent traditional retroperitoneoscopic nephroureterectomy (TRNU) (n = 28) and SCRNU (n = 58) were consecutively enrolled. Demographic characteristics, perioperative parameters, and follow-up data were collected and compared between the two groups.
Results:
Both procedures were performed effectively in 86 patients without converting to open surgery. The mean follow-up time was 45.4 months for the SCRNU group and 39 months for the TRNU group. All follow-up patients survived without incidence of bladder incision tumor. Further, the follow-up results showed that there was no significant difference in the recurrence rate of bladder tumor between the two methods. SCRNU group was superior to TRNU group because of shorter operating time, fewer perioperative complications, less postoperative pain, lower recurrence rate, and cheaper medical expenditure.
Conclusions:
The SCRNU technique is less invasive, have fewer complications, and has a better cosmetic outcome.
Introduction
Upper urinary tract urothelial carcinoma (UTUC) accounts for 5% to 10% of urothelial carcinomas. 1 In patients with multifocal tumors and a high recurrence rate, radical nephroureterectomy combined with bladder cuff excision is considered the “gold standard” for the surgical management of UTUC. 2 The conventional method, open radical nephroureterectomy involves complete resection of the kidney, the ureter and the bladder cuff through lumbar and abdominal incision. With the development of a newer, minimally invasive technique, open nephroureterectomy is gradually replaced by laparoscopy for reasons of clearer surgical vision, less surgical trauma, and fewer complications. 3,4
It is a common practice to combine retroperitoneoscopic nephrectomy with open distal ureterectomy due to easier access for bladder cuff excision. In this study, we describe traditional retroperitoneoscopic nephroureterectomy (TRNU) as a surgical procedure, in which the patient needs to be repositioned from a lateral position to a supine position, a large incision in the lower abdomen for bladder cuff resection is required, combining both laparoscopy for nephrectomy and open surgery for the excision of the bladder cuff. 5 Here, we report a modified technique for the surgical management of UTUC using the retroperitoneal approach and three trocar ports placement without an additional large incision, which we will refer to as single-position complete retroperitoneoscopic radical nephroureterectomy (SCRNU) with bladder cuff excision. In this study, we aim to compare and contrast the overall surgical outcome and tumor recurrence rate of SCRNU with TRNU.
Materials and Methods
Patients and data collection
In this retrospective cohort study, we managed to enroll UTUC patients who underwent TRNU and SCRNU from June 2013 to June 2021 at Peking University Aerospace Center Hospital. A total of 86 UTUC patients receiving surgery were consecutively enrolled and the relevant data were collected. A nonrandom allocation was used. Fifty-eight patients received the modified technique and 28 patients underwent the traditional approach. Informed consent for the surgical procedure was obtained from all patients and the study was conducted according to the principles of the Declaration of Helsinki. This study was approved by the Institutional Ethics Committee of Aerospace Center Hospital.
Detailed clinical history and preoperative examinations were evaluated. CT, fluorescence in situ hybridization, urinary cytology, and ureteroscopy were evaluated if necessary. Study participants' demographic characteristics and relevant information were retrospectively collected through our hospital database, including age, sex, and body mass index. Other variables were used as a proxy for evaluating the safety of the surgery, including the operating time, estimated intraoperative blood loss, open surgery conversion rate, and clinical pathologic characteristics. Postoperative variables such as catheter and surgical drain indwelling time, postoperative pain score, postoperative complication, length of hospital stay, and the total follow-up time were collected and analyzed.
In our retrospective cohort, none of the included study participants reported severe cardiopulmonary insufficiency or other absolute contraindications that could potentially act as confounding factors that could influence the surgical outcome before the procedure. A visual analog scale was used to evaluate the degree of pain at 1-, 12-, and 24-hour postoperatively. 6
SCRNU technique
The patient is placed in lateral decubitus position, allowing adequate access for trocar placement. Three lines will be used as landmarks for guiding the trocar placement as seen in Figure 1. The first line (line b) is made by drawing a vertical line starting from the anterior superior iliac spine. The second line (line a) and the third line (line c) are drawn by making a parallel line dorsally and ventrally ∼5 cm from line b. Based on the patient's physique, line a can be estimated to be overlapping around the midaxillary line, whereas line b is located around the anterior axillary line. Three 1 to 2 cm incisions are made with respect to the anatomical landmark of the anterior superior iliac spine.

Trocar ports distribution. Line b is made by drawing a vertical line starting from the anterior superior iliac spine. Line a and line c are drawn by making a parallel line dorsally and ventrally ∼5 cm from line b. Based on patient's physique, line A can be estimated to be overlapping around the midaxillary line, whereas line b is located around the anterior axillary line. Three 1 to 2 cm incisions are made with respect to the anatomical landmark of the anterior superior iliac spine. Port A is made 2 to 3 cm inferior to the crossing point of line a and the costa margin. Port B is placed 5 cm cephalad to the anterior superior iliac spine on line b. Port C is 10 cm laterally to port A overlapping with line c. An isosceles triangle is formed at the position of the three ports. (See Supplementary Video and Supplementary Figs. S1 and S2.) Color images are available online.
Port A is made 2 to 3 cm inferior to the crossing point of line a and the costa margin. Port B is placed 5 cm cephalad to the anterior superior iliac spine on line b. Port C is 10 cm laterally to port A overlapping with line c. An isosceles triangle is formed at the position of the three ports. Port B is used as the camera port. Two monitors are placed at the cranial and caudal sides of the patient. The surgeon and the surgical assistant are standing on the abdominal side of the patient, as opposed to the traditional laparoscopy procedure where the surgeon is standing on the left side of the operating bed. When performing the distal ureterectomy and bladder cuff excision, the surgeon and assistant switch to face the caudal side of the patient.
Blunt dissection of the dorsolumbar fascia is made and an inflatable balloon is placed and expanded with air to allow further access to the retroperitoneal space. Once adequate space is established, the perirenal fat and Gerota's fascia covering the kidney are carefully dissected to fully expose the kidney. After fully exposing the kidney, it is then mobilized ventrally, to expose and separate the renal artery posterior to the kidney. The renal artery and the renal vein are clamped with three Hem-o-lok® clips at the proximal end and one Hem-o-lok clip at the distal end, after ensuring vascular control, the renal artery is ligated. Subsequently, the renal vein is ligated using a similar approach as the renal artery.
Upper segment of the ureter is dissected and clamped using Hem-o-lok clips. After fully dissecting the kidney, the ureter is stripped along the surface of the psoas major until reaching the edge of the pelvis and the iliac blood vessel, until reaching the vesicoureteral junction. Using the retroperitoneal approach, the iliac vessels can be easily identified.
At this point of the surgery, an adjustment of the position is needed, the surgeon switched to the foot side of the patient to perform the distal ureter and bladder cuff excision, while using the monitor placed on the foot side. While pulling the proximal ureter, dissection is made along the detrusor muscle while pulling the ureter to form a cone-shaped bladder cuff, the intramural ureter could be resected by retraction from the superior and lateral directions. Thenceforth, an endoscopic gastrointestinal automatic (Endo-GIA) staple is used due to its flexibility to excise the bladder cuff at the end of the cone-shaped structure.
As recommended by the guidelines, we routinely perform lymph node dissection for high-risk nonmetastatic UTUC in clinical practice, 7,8 but not for TaT1 UTUC because of the low risk of lymph node metastasis. 9 –11 Due to the limited space, lymphadenectomy may appear to be a challenge, however, the curative role and the extent of lymphadenectomy remains a matter of debate. In our study, lymphadenectomy is performed for patients with tumor staging above T3 in combination with neoadjuvant chemotherapy or switching to open approach. Due to anatomical differences in male and female patients, the uterine artery is severed to ensure the operation space.
The specimen is placed in an endoscopic specimen bag and removed from the enlarged incision of port A. The specimen must be carefully examined to ensure that the bladder cuff has been fully resected during intraoperative period (Fig. 2). Finally, a drainage tube is placed into port B.
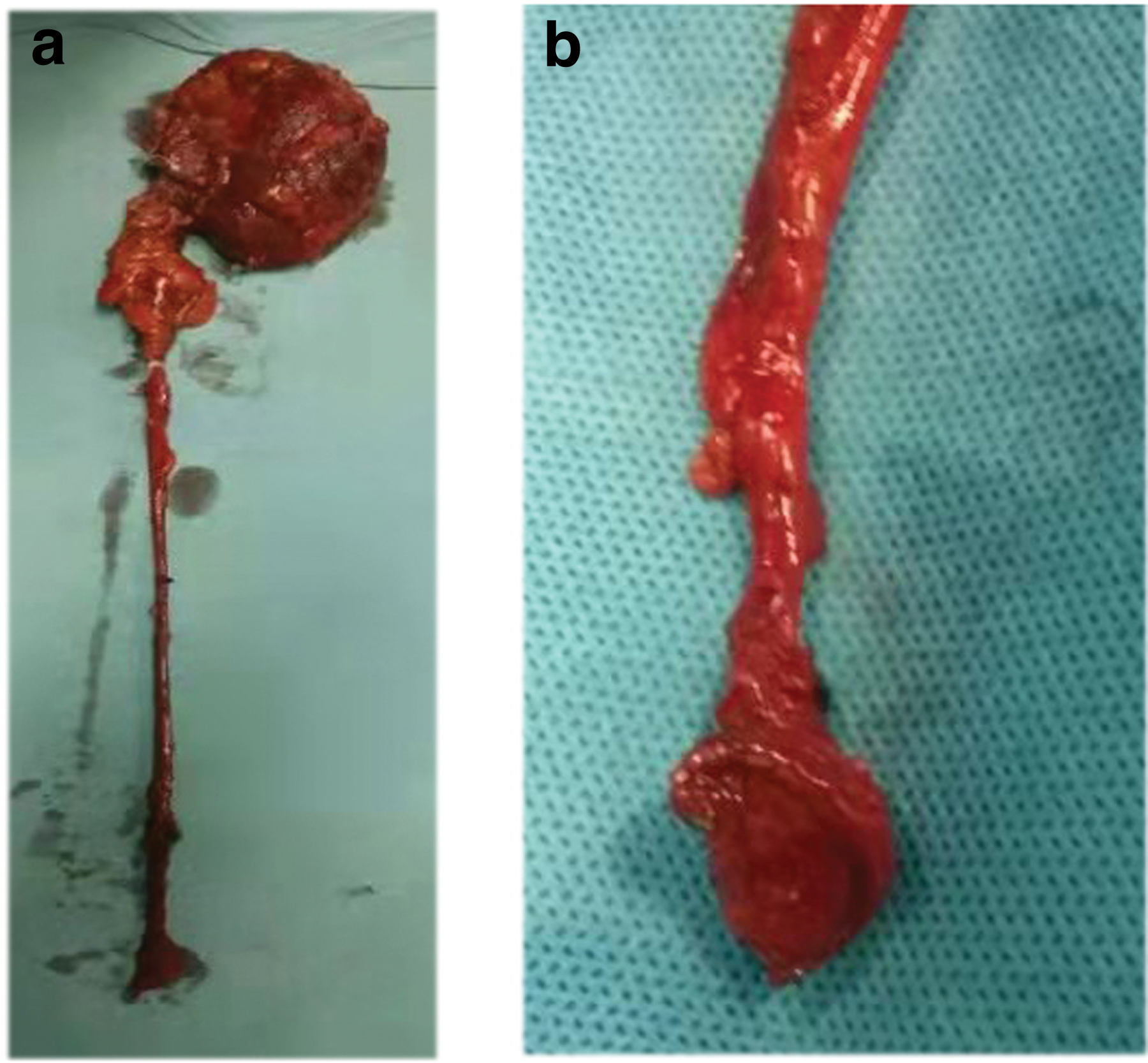
Complete bladder cuff excision.
Postoperative care and follow-up
Intravesical instillation of chemotherapeutic agent was performed within 24 hours postsurgery, epirubicin was the drug of choice in our practice. The surgical drain was left in place and could be removed 1-week postsurgery if there was sign of minimal drainage. We routinely performed cystoscopy 2 weeks after surgery in all patients to confirm whether the bladder cuff had been totally resected and to ensure no evidence of the formation of bladder fistula. All patients with a postoperative pathologic staging of pT3 were treated with gemcitabine and cisplatin regimen for four cycles.
Considering that UTUC has a high recurrence rate and progressiveness, postoperative surveillance was performed every 3 months during the first-year postsurgery, every 6 months during the second year, and annually for 5 years. Urologic ultrasonography, urinalysis, cytology, and cystoscopy were performed according to current guidelines. 8 CT urography, chest CT, and bone scan were performed for routine evaluation.
Statistical analysis
Statistical differences in both groups were measured and performed using nonparametric test of the null hypothesis, in particular, Student's t-test and Mann–Whitney U test. All data were analyzed using SPSS 16.0. The difference between both groups was considered statistically significant if the p-value was <0.05.
Results
A total of 86 patients were enrolled in this study: 58 in the SCRNU group and 28 in the TRNU group. The clinical characteristics of included patients were shown in Table 1. No significant differences were detected between the two groups in terms of baseline characteristics (all p > 0.05, Table 1).
Clinical Characteristics of 56 Patients with Upper Urinary Tract Urothelial Carcinoma
SCRNU = single-position complete retroperitoneoscopic radical nephroureterectomy with bladder cuff excision; TRNU = traditional retroperitoneoscopic nephroureterectomy with open bladder cuff excision.
None of the patients required conversion to open surgery and the resected specimen showed no positive surgical margin. The bladder cuff of all the patients had been confirmed to be removed completely (Fig. 2). The surgical outcomes of SCRNU group and TRNU group are shown in Table 2. Compared to TRNU group, patients in SCRNU group had shorter operative time (p < 0.001), less estimated blood loss (p = 0.002), shorter drainage indwelling time (p = 0.003), faster restoration of bowel function (p = 0.003), lower pain scores evaluated at 1, 12, and 24 hours after surgery (p = 0.009, p = 0.012, and p = 0.023, respectively), shorter length of hospital stay (p = 0.003), and less medical expenditure (p = 0.003).
Surgical and Follow-Up Outcomes Between the Two Cohorts
Twenty patients (34.5%) in SCRNU group and 12 patients (42.9%) in TRNU group reported postoperative complications of fever, infection, bleeding, and lower limb deep vein thrombosis in Grade I/II (Clavien classification). All of the postoperative complications and symptoms were treated and resolved after treatment. None of the included patients experienced major complications.
Findings from direct observation under cystoscopy revealed that the bladder incision healed nicely in all study participants, and the ureteral orifice was not observable on the affected side. The staples can be seen located within the bladder mucosa (Fig. 3). Using this surgical method, we do not observe formation of calculi or bladder fistula in all study participants.

The healed bladder incision healed well after bladder cuff resection.
Seven study participants were lost to follow-up. The mean follow-up time was 45.4 months for SCRNU group, compared with 39 months for TRNU group (Table 2). By the end of follow-up, all of the included participants survived. The bladder tumor recurrence rate was similar in the SCRNU group compared with the TRNU group (14/58 vs 8/28, p = 0.66).
Discussion
In the traditional surgical management for UTUC, the patient needs to be repositioned and resterilized which complicates the procedure. To address this issue, we have developed a new surgical approach, SCRNU, and proposed new surgical technique to manage the distal ureter and excising the bladder cuff since 2013.
Generally, there are two types of approaches for laparoscopic nephroureterectomy, both of which can be performed effectively and efficiently through the transperitoneal approach and the retroperitoneal approach. 5 One of the key advantages of transperitoneal approach is that it can provide a relatively larger space for operation. However, compared to retroperitoneal approach, transperitoneal surgery may have a greater risk of intra-abdominal organ injury. 12,13 There is also concerns about a higher risk of intraperitoneal implantation of tumor cells by transperitoneal approach, resulting in worse disease progression. 14 In addition, when dealing with the lower ureter, the limited dissection space in the lower abdominal and the pelvic area increased the complexities and can be more challenging for the operator. In light of these considerations, we adopted the retroperitoneal approach.
For our SCRNU technique, the three trocar ports were positioned ventrally to increase more space for excising the lower ureter and the bladder cuff. No additional trocar port or incision in the lower abdomen was required. More importantly, intraoperative repositioning of the patient is not needed, making this procedure preferable for both the patient and the operator. Other published studies reported the surgical technique and option for retroperitoneal resection of the bladder cuff by increasing the number of trocar ports. 15,16 By simplifying the conventional TRNU approach, the surgery can be performed more straightforwardly, only requiring switching the position of the surgeon and the camera placement port during the operation. With the current trend where minimally invasive surgery has become the norm and the increasing prevalence of robot-assisted laparoscopic surgery, 17,18 our laparoscopy technique can also be adapted and modified to be performed using robot arms.
Both the TRNU and SCRNU use the retroperitoneal approach. However, compared with the traditional method, our proposed surgical technique had shorter operative time, less blood loss, shorter duration of drainage indwelling time, and shorter length of hospital stay. This could be attributed to not requiring the patient to be repositioned for the ureterectomy and bladder cuff excision, without having the need for repeated surgical position adjustment, resterilization, and open incision, we manage to shorten the surgical time, resulting in less blood loss and less manipulation of the abdominal viscera. In addition, postoperative pain and the mean hospital stay decreased in the SCRNU group patients were less than the TRNU group. The follow-up results showed that bladder incision tumor has not occurred and the recurrence rate of bladder tumors was no significant difference between the two groups.
To avoid leakage of urine containing tumor cells and disseminating in the body, an Endo-GIA™ stapler was used to remove the bladder cuff and seal the stump simultaneously. However, with this technique, residual urothelium between the staples of Endo-GIA stapler might result in an incomplete excision of bladder cuff. 19 To address this issue, the specimen should be examined to confirm that the bladder cuff has been removed completely. McDougall and colleagues followed 25 patients with bladder cuffs excision using Endo-GIA stapler for 2 years and reported no metastases. 20
Based on our own experience and the retrospective data that we collected, we did not observe metastasis on the bladder excision site. Bladder stone formation is another concern due to the exposed staples at the anastomotic site. To deal with this issue, we routinely performed cystoscopy procedures to screen for metastasis and bladder stone formation. As shown in Figure 3, the staples can be seen within the bladder mucosa, and no stone formation was found.
Despite of the anatomical differences in male and female patients, we did not observe any significant difference in terms of the operative time. For female patients, the broad uterine ligament can be pushed medially along with the peritoneum in the new SCRNU approach, and it is made possible to avoid these tissues as opposed to the TRNU technique. This would protect the overall integrity of the pelvic floor of female patients.
The limitations of our study are the relatively small sample size, the relatively short follow-up time, and data collected retrospectively in a single center. We tried to minimize selection bias by including all study participants; however, since the study is conducted in a single center, selection bias might still be a concern. In addition to the tumor site and clinical stage, the pathologic characteristics of the tumor and other factors might be confounding factors that can potentially influence the surgical outcome. Regardless of the limitations, our study proposed an innovative way to manage UTUC safely and effectively. Future studies with randomized controlled trial design with multicenter collaborations and longer follow-up time are needed to further establish the safety and effectiveness of the new SCRNU technique.
Conclusions
In this study, we report a modified single-position, completely retroperitoneoscopic nephroureterectomy technique that is feasible, safe, and minimally invasive approach to managing the distal ureter and bladder cuff. It is more superior in terms of postoperative outcomes, with shorter operative time, less blood loss, and more aesthetically pleasing. Moreover, patient repositioning is not needed during the surgery.
Footnotes
Acknowledgments
We thank the patients for consenting to participate in this study.
Authors' Contributions
Y.S. and S.W. are the first authors, who collected surgical data, processed the data, and wrote the article. Z.L. and L.Y. helped with data collection and assembly. Q.G., Z.L., and Z.X. performed data analysis and interpretation. W.L. and S.S. revised and edited the article . H.W. and B.Z. helped with the final correction. All authors read and approved the final version of the article.
Consent for Publication
Written informed consent was obtained from patients for the publication of this report and any accompanying images. All authors agreed to publish this work.
Ethics Approval and Consent to Participate
Informed consents were obtained from all patients before surgery and the study was approved by the Institutional Ethics Committee of Aerospace Center Hospital.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video
Supplementary Figure S1
Supplementary Figure S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.