
Abstract

W
A 7-year-old female child with cloacal exstrophy underwent neonatal closure of exstrophy and correction of exomphalos with osteotomy and colostomy. Subsequently the bladder was reconstructed at ∼5 years of age with 35 cm of ileum and a 2.5 cm Monti continent valve conduit in the right lumbar region. Both the ureters were reimplanted in the ileum and the bladder neck was closed (Fig. 1). The left ureteral reimplant was not draining adequately and became symptomatic. A left percutaneous nephrostomy was done, and a guidewire was passed into the neobladder, over which a 5F Cook multilength ureteral Double-J stent was passed. The nephrostomy was subsequently removed, and a routine stent change was done through the Monti orifice.
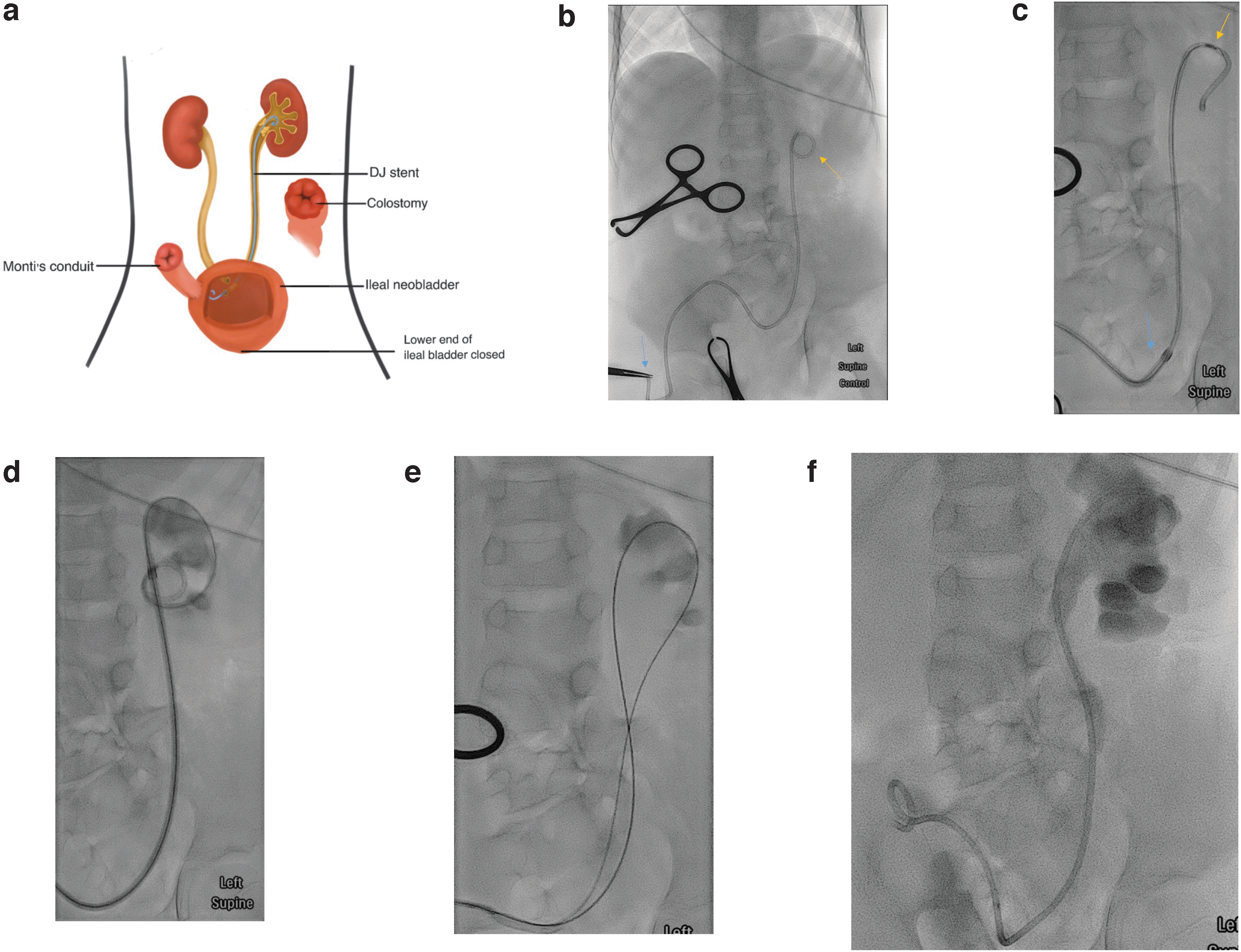
a) Diagram of operative bladder reconstruction
The latest stent change was attempted at 8 months gap because of a delay resulting from other major orthopedic reconstructions that resulted in encrustations in the stent and needed the use of a novel approach to change the stent, as described in this report. Cystoscopy was performed under general anesthesia using a 9.5 scope in the supine position through the Monti stoma. The lower end of the Double-J stent was retrieved and the lower end of the stent was passed over to the interventional radiologist.
Attempts to advance a standard 0.889 mm hydrophilic guidewire (Terumo, Japan) through the Double-J stent failed because of severe encrustation of the upper end. A thinner 0.457 mm “V-18” (Boston Scientific, Natlick, MA) was also ineffective in crossing the central lumen of the stent. A long (8F × 35 cm) sheath (Brite Tip; Cordis, USA) was then advanced over the Double-J stent into the left pelvis. The stent was then retrieved intact and confirmed to be severely encrusted.
Over a stiff Amplatz wire, dilatation of the vesicoureteral junction was subsequently done with 4 mm and 6 mm balloons. A new 7F × 26 cm Boston Scientific Percuflex stent was inserted. Postoperatively, the patient was admitted overnight for observation and discharged the next day with subsequent follow-ups with interventional radiology in 3 months.
We feel that this case demonstrates the effectiveness of the technique even in a pediatric patient with smaller anatomy. The sheath size used should be adapted to the Double-J stent in situ and the size of the patient. In addition, these kids have undergone several operations and reoperations are difficult, thus, access is limited to the artificially created Monti stoma. Hence this approach to changing stents is novel and valuable. As this was the first time this technique was documented to be done through a Monti's stoma, attached hereunder are references on the effects of a ureteral stent change in a Monti stoma and their relevant complications. 2,3
Footnotes
Acknowledgment
The authors acknowledge the contribution of Nah Jie Hui for her creation of the illustration for this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.