
Abstract
Objectives:
To improve care in patients with large kidney stones using advanced intraoperative imaging techniques to reduce perioperative radiation exposure, improve stone-free rates (SFRs), and reduce the number of surgical interventions in a quality improvement project.
Patients and Methods:
Patients with kidney stones appropriate for percutaneous nephrolithotomy (PCNL) treatment were scheduled into a hybrid operating room for endoscopic surgery (PCNL and/or ureteroscopy) with intent to perform intraoperative CT (ICT). Imaging was performed using an Artis Zeego Care+Clear™ (Siemens) robotic-armed multiplanar fluoroscopy system with collimation to the level of the affected kidney(s). After the initial case, the proprietary CARE™ (combined applications to reduce exposure) protocol was used. When the hybrid room was unavailable, a mobile CT scanner (O-Arm; Medtronics) was used in the traditional room (n = 2).
Results:
Thirty-one ICTs were performed in 23 consecutive patients during endoscopic stone procedures with a median effective radiation dose of 1.39 mSv per scan, significantly less than the preoperative noncontrast CT (12.02 mSv) in the same patients (p < 0.001). Longitudinal radiation exposure associated with stone treatment significantly decreased by 83% (15.80 to 2.68 mSv, p < 0.001) compared with a similar historical PCNL cohort. Clinically significant residual stones (≥3 mm) were identified at initial ICT in eight patients (35%) and further treated in six patients. One patient had missed residual stone diagnosed 34 days after surgery, which was apparent on re-review of the ICT. Thus, final verified SFR was 87% for all stages. Mean number of procedures improved from 1.77 to 1.30 (p = 0.05) and rate of postoperative CT scans improved from 82% to 26% (p < 0.001).
Conclusion:
Ultralow-dose ICT was demonstrated to simultaneously improve SFR and number of staged treatments, and greatly reduce the perioperative radiation dose for our patients. The findings support the continued use of this modality to benefit all patients with large stones.
Introduction
After the field of endourology was born in the Veteran's Affairs system in 1978, 1 percutaneous nephrolithotomy (PCNL) became the standard treatment for large kidney stones. Since 2014, such stones have more typically been treated at our facility with retrograde ureteroscopy (URS) using high-power (100 W/120 W) holmium laser systems, and this approach has gained increasing acceptance internationally. 2 Stone-free rate (SFR) after stone surgery has been used as a marker of treatment quality. 3 However, patients with complex stones are at risk for residual fragments.
Stone patients also experience higher levels of radiation exposure than the general population, averaging 3.1 mSv per year, and 20% of patients at two large medical centers exceeded the 50 mSv occupational exposure limit recommended by the International Commission on Radiological Protection just related to follow-up imaging within a year of acute stone treatment. 4 Similarly, urologists and operating room staff treating these patients are at a risk of higher-than-average radiation exposure. 5 “As low as reasonably achievable” (ALARA) radiation principles mandate continuous efforts to reduce radiation exposures.
Urologic applications of advanced hybrid room imaging, including intraoperative CT (ICT), were initially described for percutaneous access and stone assessment using an “Artis Zee” (Siemens Medical Solutions, Melvern, PA) ceiling-mounted system (CMS) and the proprietary “UroDyna-CT” cross-sectional imaging protocol. 6 –8 The first case to assess residual stone burden and then confirm SFR during PCNL was reported in 2017, using an “Artis Zeego” floor-mounted robotic-armed multiplanar fluoroscopy system (RMPFS) to perform multiple ICTs. 9
In 2021, a series of 20 PCNLs used an RMPFS to perform a single ICT, with further treatment of missed stones in several cases. 10 A second series of 18 PCNL cases similarly performed one ICT using an “Artis Q” CMS. 11 These studies have demonstrated the utility of ICT in improving SFR. This report describes the incorporation of routine ICT to simultaneously improve large-stone treatment and reduce total radiation exposure in our patients.
Methods
A quality improvement (QI) project intended to improve the surgical care of nephrolithiasis patients using ICT and other advanced imaging techniques was authorized by our IRB in July 2021. For patients with large stone burdens, specific goals included improving SFR, the need for second-stage surgery, operative time, and radiation exposure. Ex vivo imaging evaluations were performed using a phantom model and artificial stones, similar to previously published methods. 6
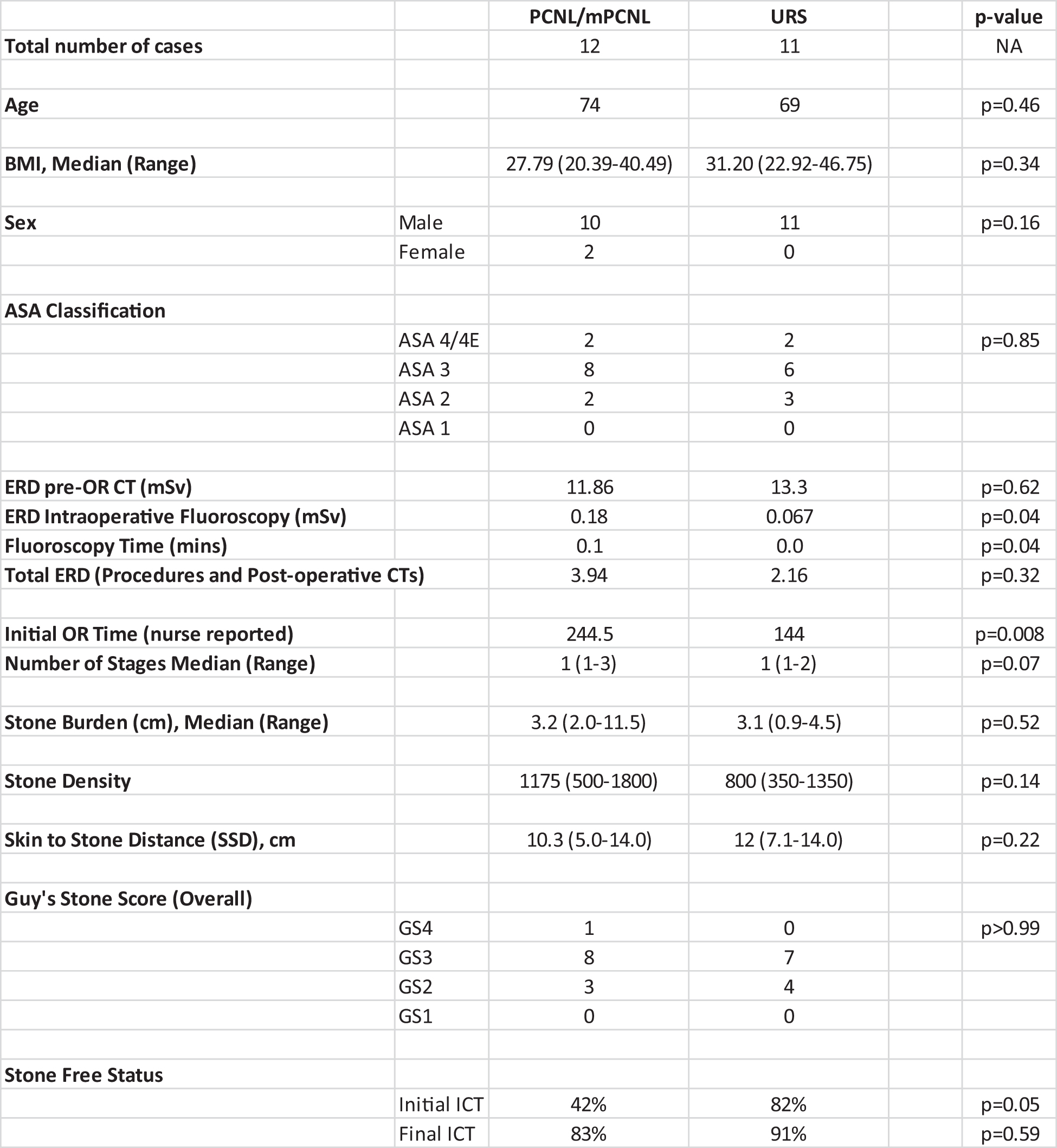
Artificial stones, as small as 2.7 mm, were confirmed to be easily observed using reduced-dose protocols with each system (Fig. 1). Patients with kidney stones that were appropriate for percutaneous treatment were treated with endoscopic surgery (PCNL and/or URS) in a hybrid operating room. RMPFS (Artis Zeego Care+Clear™) was used for fluoroscopy and coaxial imaging.
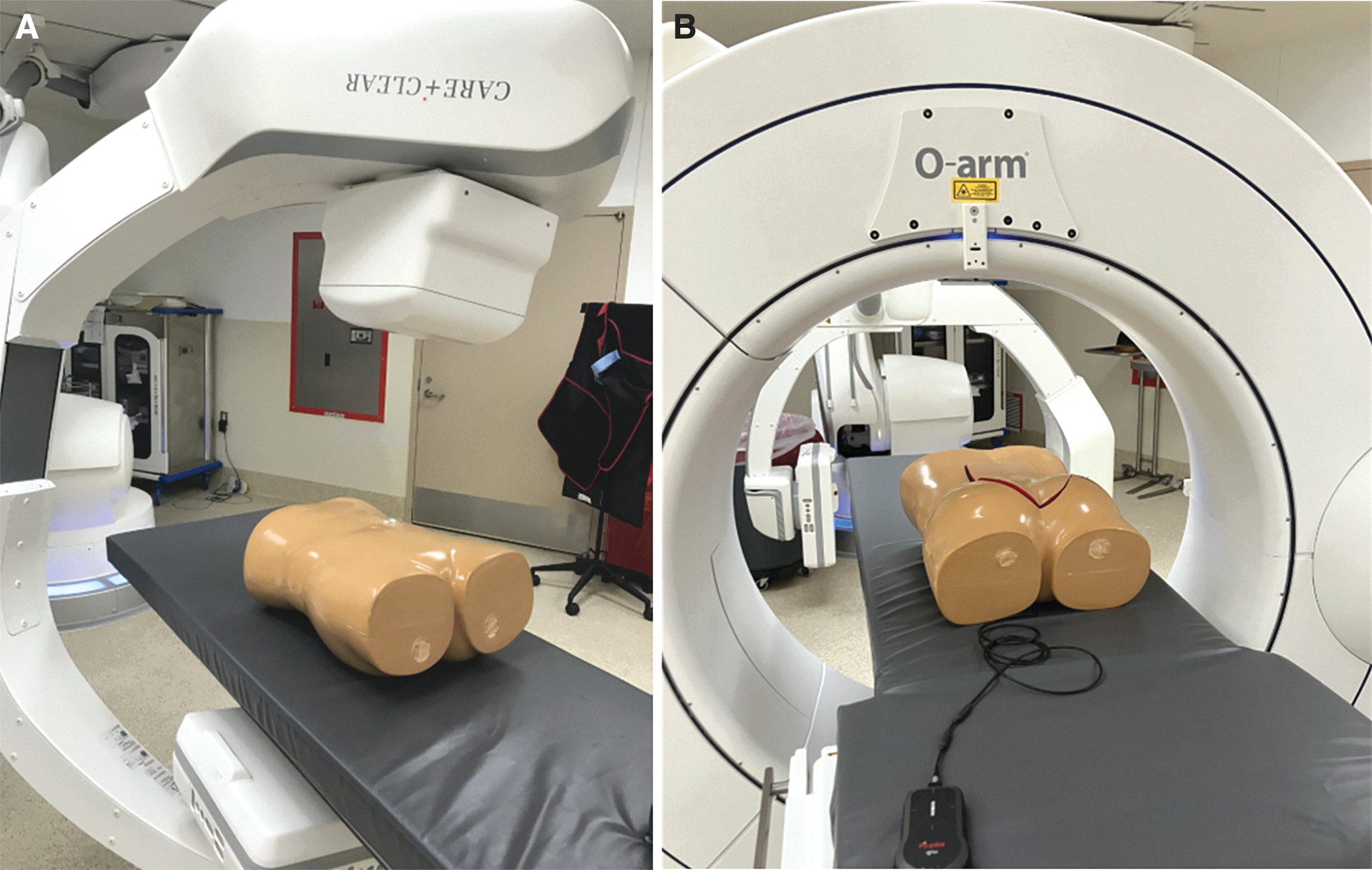
When the hybrid room was unavailable, ICT with a mobile system (O-Arm™; Medtronic, Minneapolis, MN) was offered, and fluoroscopy was then performed either with a traditional fluoroscopy system or with O-Arm. Both attending surgeons (M.D.S. and E.C.B.) trained at internationally recognized stone centers and were comfortable obtaining and teaching percutaneous access. The details of the surgical methods unrelated to CT imaging are provided (Appendix A1).
After endoscopic stone treatment was assessed to be complete or otherwise indicated, ICT was performed (Fig. 2). In PCNL cases, the surgical field was covered with drapes or the access site was closed while leaving a transurethral access sheath or wire in place. During the initial test phase, fluoroscopy confirmed kidney localization and craniocaudal collimation limits were set to the estimated boundaries of the kidney with a suitable margin for renal excursion. Apnea was induced immediately before ICT to avoid potential motion artifacts.

Ultralow dose (5sDR BODY CARE protocol) with phantom model and Plaster of Paris “stones.”
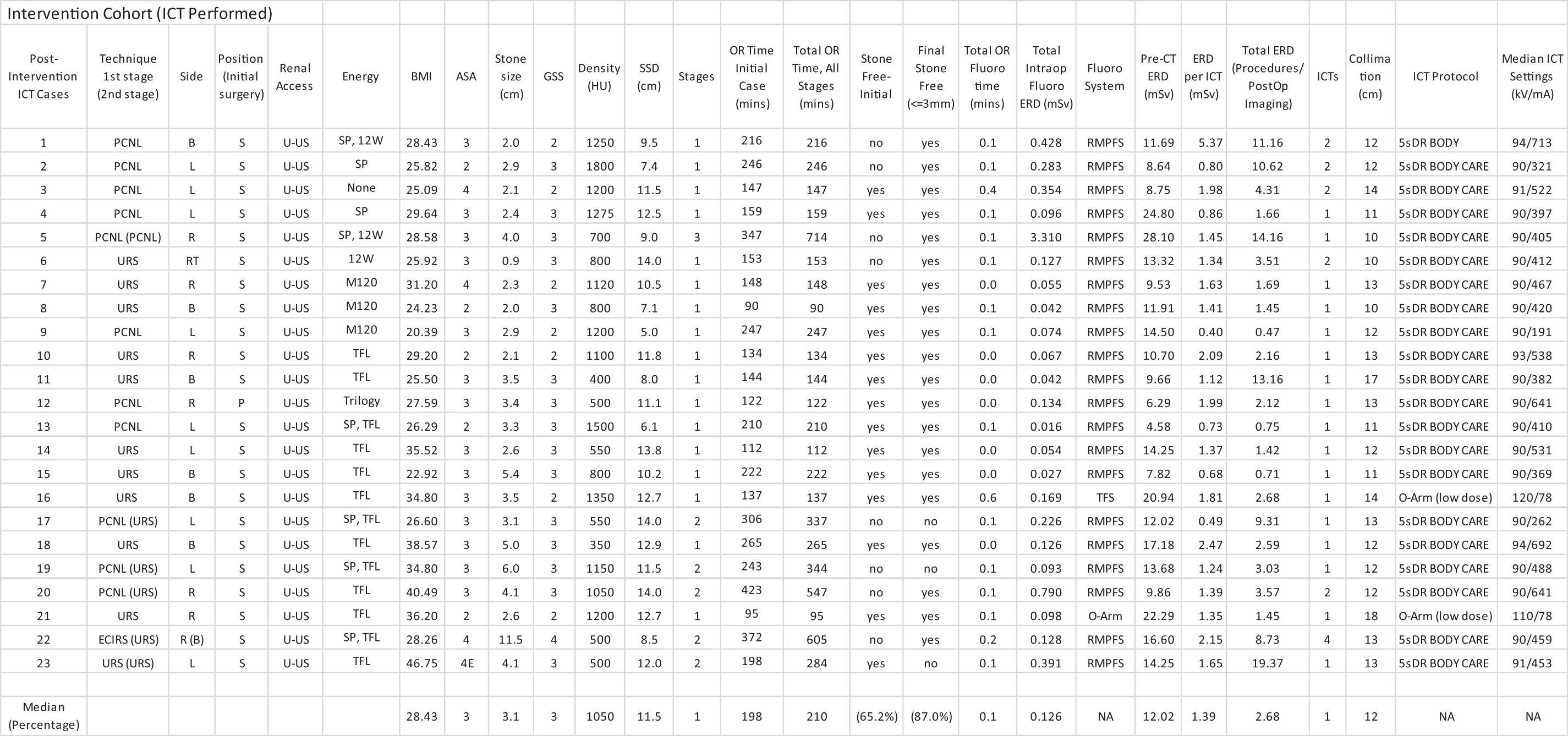
Cone beam 3D images were obtained during a 5-second 200° rotation of the C-arm. After the initial case, a further reduced-dose CARE™ (combined applications to reduce exposure) protocol (“5sDR BODY CARE”) was used. With the O-arm, a low-dose medium-sized patient abdominal protocol was utilized. ICT image settings are reported in Table 1. Coronal, axial, and sagittal image reconstructions were immediately reviewed by the surgeon. With concern for residual stones, further endoscopic evaluation was performed, followed by additional ICT when indicated after treatment.
Intervention and Retrospective Cohort Case Details
Effective radiation dose (ERD) was used to compare imaging modalities. Intraoperative radiation dosage was collected as dose area product (DAP) separately for routine fluoroscopy studies and ICT. DAP measurements for intraoperative imaging were converted to ERD using Monte Carlo simulations that considered both gender and variable directions of a radiation source, using NCIRF 1.0 software (National Cancer Institute) 12 (Appendix A2). Because of differences in ERD conversion methodology, comparisons with previously published ICT series were made using DAP values instead.
In addition, until 2019, interventional radiology reports at our facility included only the skin dose (mGy). A DAP conversion factor (0.25 Gy·cm2/mGy) was used for these procedures, since this was the consistent relationship observed using operative fluoroscopy in the same patients. The ERD for CT scans at our facility was automatically calculated from the dose length product (DLP) using NCIDOSE 2.0 software. When ERD was not provided in the radiology report, conversion was performed from DLP using an online resource, 13 which provided identical results.
Preoperative CT protocols requiring multiple scans were adjusted to report the equivalent ERD for a single scan but not for postoperative scans. Data on patient characteristics were prospectively collected. A retrospective chart review was performed on a historical cohort of patients who underwent PCNL without ICT. Radiation reports, including fluoroscopy time, DAP, and DLP, were attached to all imaging studies and reviewed in the picture archiving and communication system (PACS). Plain KUB doses were not typically included in the report or imaging, and a historically reported ERD of 0.7 mSv per KUB was assumed in the total radiation calculation. 14
“Operative times” were calculated retrospectively based on surgical nurse entry into the EMR, typically from the precystoscopy time-out until ready for extubation. Total operative time is the sum of case operative times performed in the operating room related to a given stone treatment, but also includes time of contralateral stone treatments performed contemporaneously. Operative time in the initial case is separately reported for clarity. Standard statistical methods were used in R/RStudio (4.0.3), 15,16 including Fisher's test for equality of proportions, the Kruskal–Wallis rank sum test for median values, and Welch's t-test for comparison of mean values.
Results
Twenty-four consecutive patients appropriate for PCNL from August 2021 to June 2022 were treated with RMPFS (n = 22) or O-Arm (n = 2). One patient with RMPFS was excluded preoperatively after Siemens technical support advised against attempting ICT because of extreme habitus (body mass index [BMI] = 69 kg/m2). Thus, 23 patients (30 renal units) were included based on intention to perform ICT. The stone burden was ≥20 mm in all cases, except in the transplant kidney.
Twelve patients were treated percutaneously and 11 patients (18 renal units) were treated exclusively retrograde. Thirty-one ICTs were performed, and 26% of patients had two or more ICTs. The ICT settings were 93.5 kV/713 mA for the initial BODY protocol case; 90 kV/437 (191–692) mA for the BODY CARE protocol cases using RMPFS, and 110 to 120 kV/78 mA using the O-Arm. (Table 1).
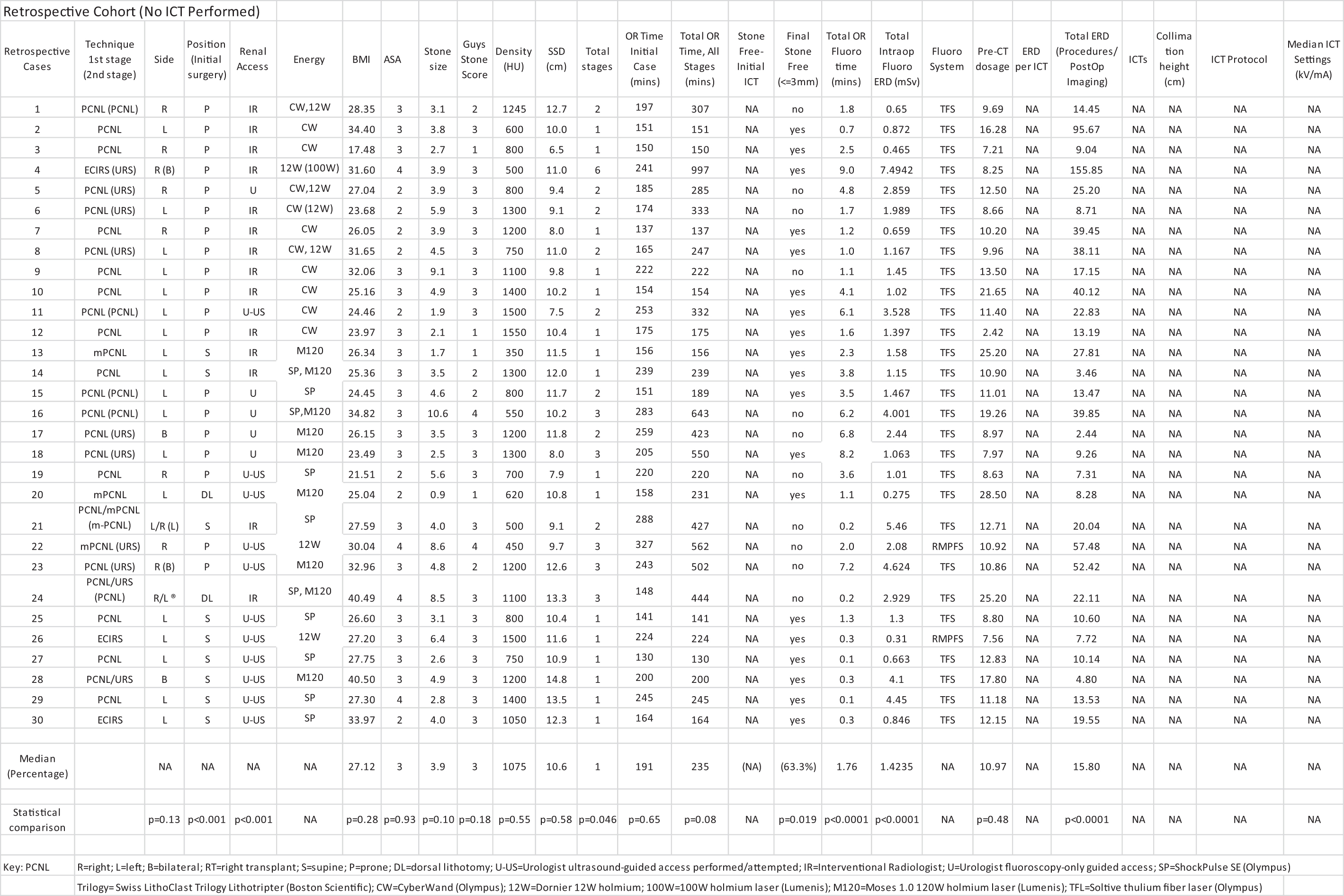
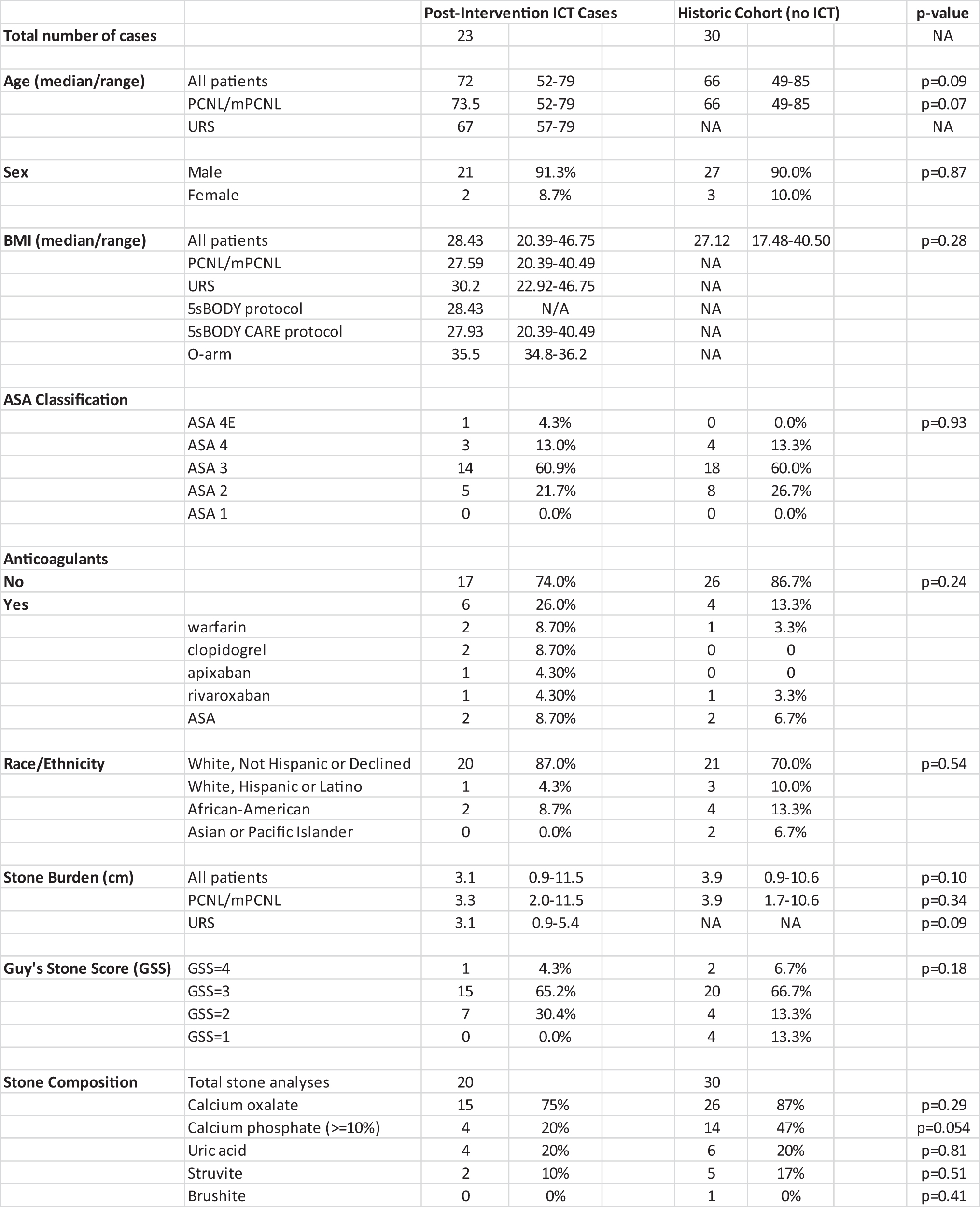
Comparisons were made to a retrospective cohort of 30 patients who underwent PCNL or attempted PCNL without ICT between July 2014 and July 2021 (Tables 1 –3). There were no statistically significant differences in age, gender, ethnicity, BMI, stone burden, stone density, skin-to-stone distance, Guy's Stone Score (GSS), stone composition (e.g., struvite), American Society of Anesthesia score (ASA), anticoagulants, or preoperative CT ERD between intervention and historical cohorts, nor in subset comparison of intervention PCNL and URS patients (Table 4). For intervention PCNL cases, significant differences were found in supine positioning (92% vs 30%, p < 0.001) and tubeless procedures (50% vs 7%, p = 0.001).
Summary of Patient Characteristics
Surgical Procedure Details

Comparison of Ureteroscopy and Percutaneous Nephrolithotomy Postintervention Cases
The final SFR after all stages improved from 63% to 87% after implementation of routine ICTs in our practice. Initial ICT demonstrated SFR of 66%; 83% in URS cases and 42% in PCNL cases, respectively. Further attempts to treat residual stones after ICT were made unless observation (e.g., clots) and/or amount of residual stone burden either made this futile or would have prolonged operative time beyond our comfort level (Fig. 3). In one case, residual calcifications were interpreted as “dust” on ICT. However, after diagnosis of 6 and 4 mm obstructing ureteral stones on CT scan 34 days postoperatively, a distinct corresponding calcification within the dust was able to be identified on retrospective review and the SFR and ERD were adjusted accordingly (Fig. 4).
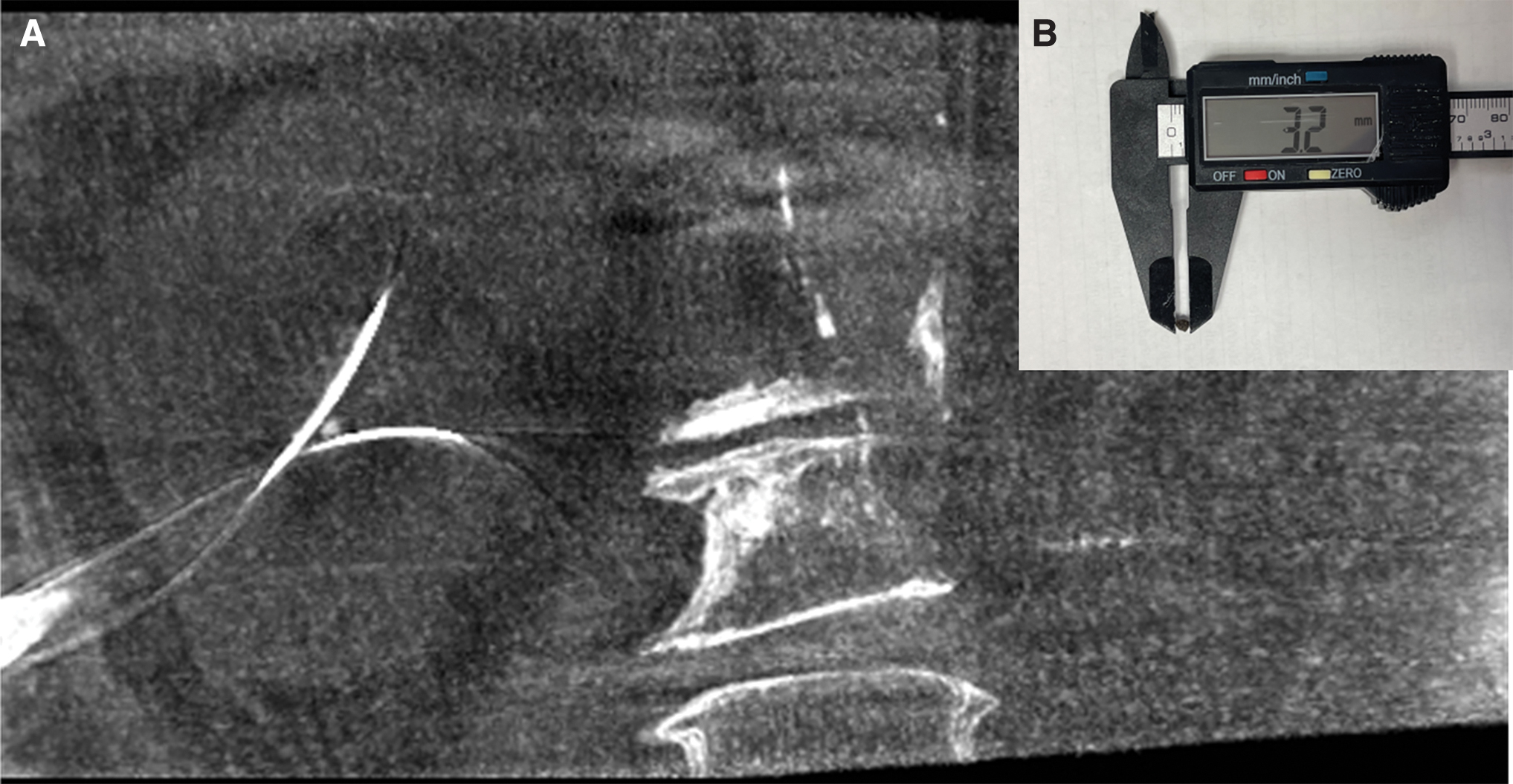
Initial patient with residual stone removed after ICT.
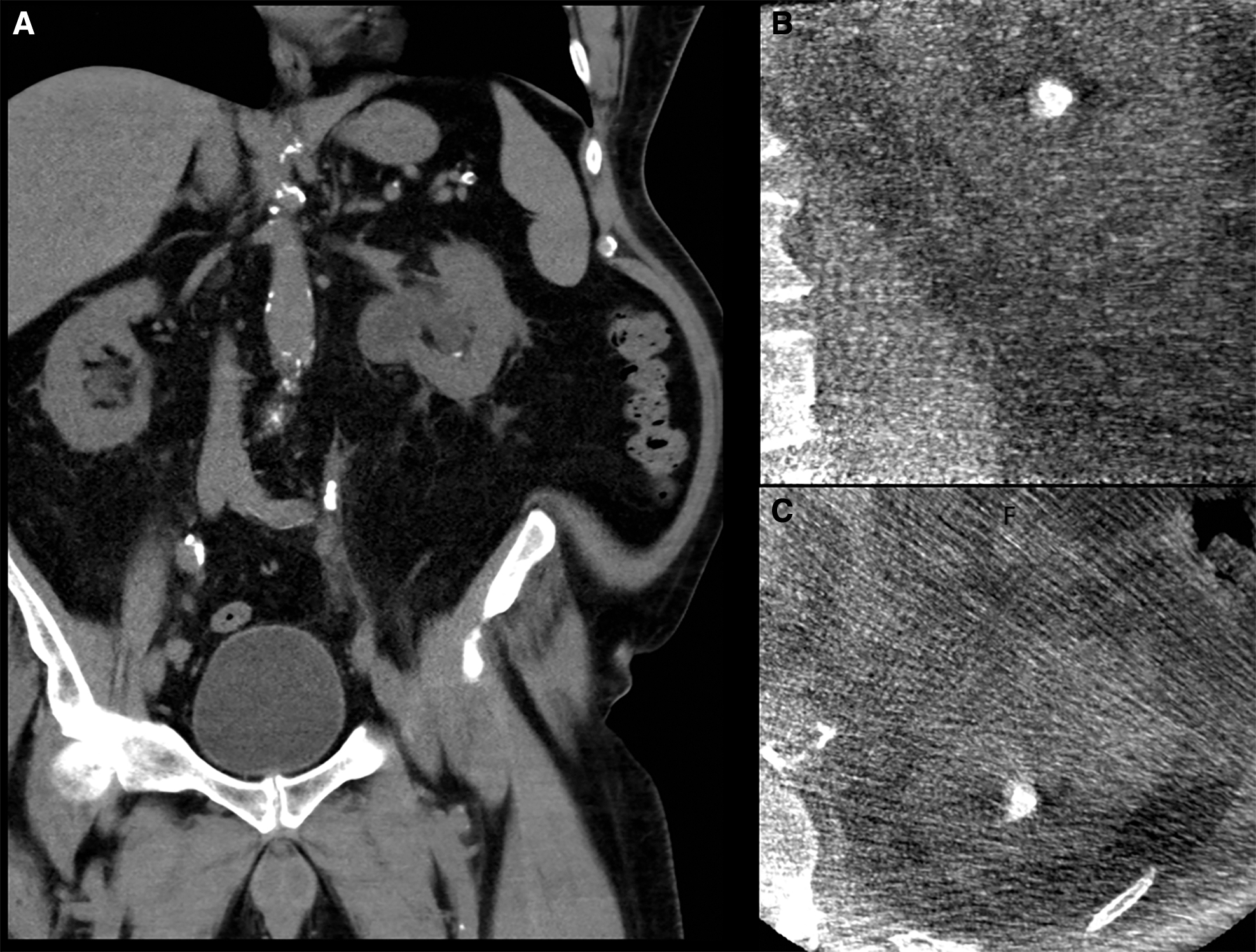
Missed residual stone originally interpreted as “dust”.
Thus, the final ICT SFR increased to 91% in the URS group and 83% in the PCNL group. Of the eight patients with residual stones on initial ICT, three were effectively treated immediately, and three patients were rendered stone free with subsequent surgery. Two patients still had residual stones even after staged surgery performed later using a retrograde approach because of intraparenchymal calcifications or unusually challenging anatomy (Fig. 5). In addition, mean number of procedural stages (i.e., total number of anesthesia events) was significantly lower in the intervention cohort (1.30 vs 1.77, p = 0.05).
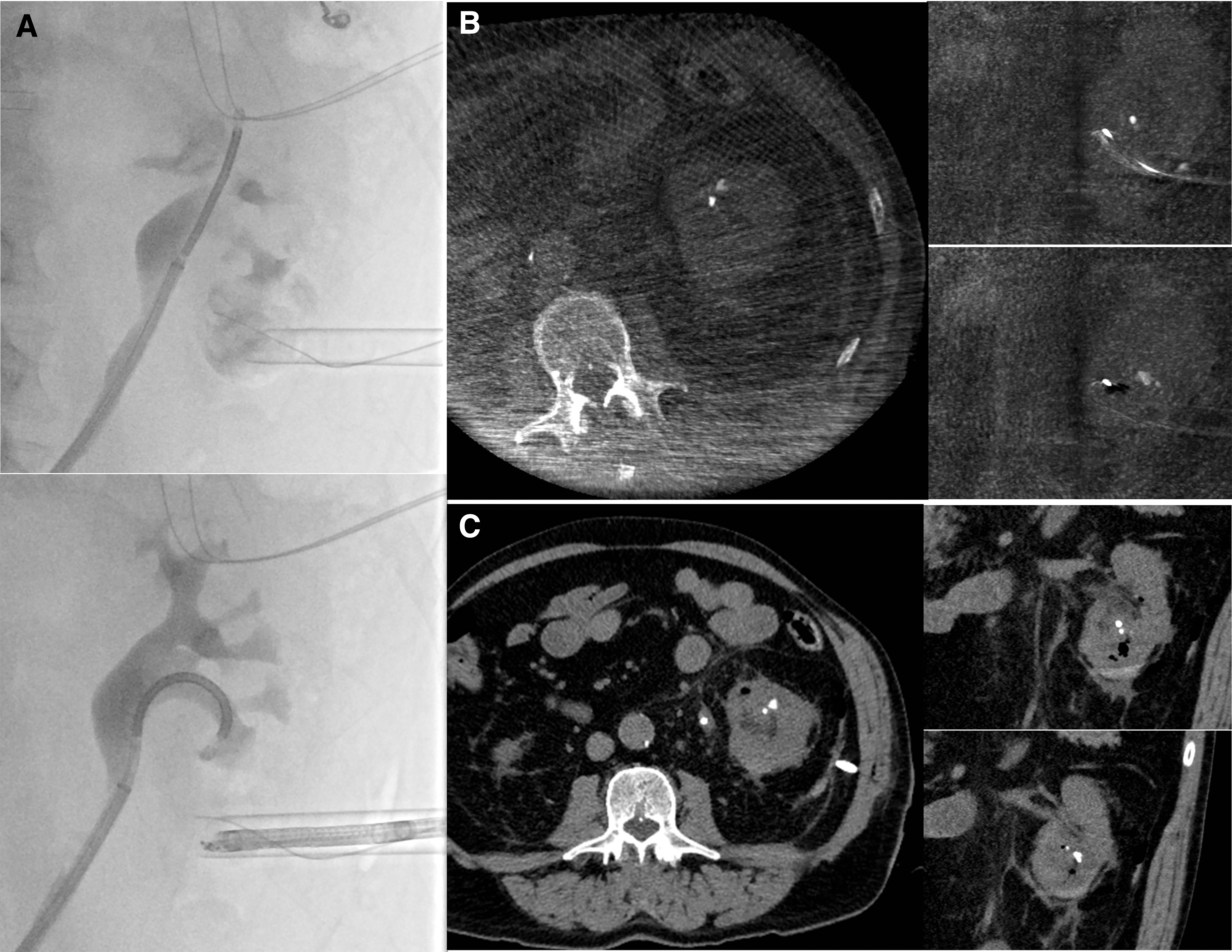
Intraoperative fluoroscopy with comparison of intraoperative and postoperative imaging in a patient with prior radical cystectomy and ileal conduit.
The total cumulative radiation dose related to treatment and postoperative imaging for large kidney stones was significantly lower after the intervention at 2.68 mSv, compared with 15.80 mSv (p < 0.001). Even after excluding initial diagnostic imaging, 13% of historic patients exceeded 50 mSv during and after treatment, whereas the highest total ERD after intervention was 19.35 mSv. ERD per ICT was 1.39 mSv, an 88% dose reduction from preoperative scans (12.02 mSv).
One complex paraplegic patient with struvite-containing stones (case 22) had four ICTs performed before being rendered stone free; however, the combined ERD of 8.60 mSv was 48% lower than that of the preoperative CT (16.6 mSv). In addition, the proportion of patients with at least one standard CT after initial surgery was significantly lower (26% vs 82%, p < 0.001).
The CT rate after final treatment (within 3 months) in the historic cohort was 43%. In addition, contributing to the overall dose reduction was a combination of increased adoption of ultrasound-guided access by surgeons and fluoroscopy dose reduction technologies of the RMPFS. This decreased operative fluoroscopy time from 1.8 to 0.1 minutes and fluoroscopy-related ERD from 1.42 to 0.126 mSv (p < 0.001). The total ERD was higher in the postintervention PCNL than in URS patients (3.94 vs 2.16 mSv), but the difference was not significant (p = 0.32).
In ICT cases, initial cases were 198 minutes and total case times (all related surgeries) were 210 minutes. This was slightly higher than initial case time (191 minutes), but lower than total combined case times (235 minutes) in the retrospective cohort, but only approached significance (p = 0.08) for all combined case times. Initial case operative time was 53.5 minutes higher for the PCNL cases with ICT than preintervention (244.5 minutes), but this was not significant (p = 0.09). The gap narrowed to only 11.5 minutes when comparing total operative time for all stages (246.5 minutes vs 235 minutes, p = 0.71). Initial case operative times in the URS patients (144 minutes) were 100.5 minutes lower than those in the postintervention PCNL cases (p = 0.008).
Thirty-day complications were equivalent between the postintervention and preintervention groups with no deaths (p > 0.99). After the QI intervention, there was one Grade IV and two Grade II complications. This included an ICU admission for fluid overload attributed to perioperative fluid management, a patient with preoperatively treated candiduria having a brief episode of fever and hypotension responsive to antibiotics and fluids without ICU care required (Candida identified on blood cultures), and a patient admitted postoperatively for constipation and stent pain. In the preintervention cohort, there was one Grade IIIa and one Grade II complication. These included a patient with pneumothorax requiring a chest tube after dilation of a tract over a previously placed nephrostomy tube; and an admission for pain, acute kidney injury, and perinephric hematoma. All patients recovered well and were discharged uneventfully.
Discussion
This QI initiative simultaneously addressed two important clinical problems in current stone practice to improve patient care: intraoperative identification of incomplete stone treatment and reduction of overall radiation exposure by obviating the need for follow-up cross-sectional imaging in most cases. Two recent series demonstrated the utility of ICT during PCNL to identify incomplete stone treatment and to improve SFR using RMPFS or CMS, and our findings were similar.
Both studies were limited to a single ICT, with subsequent CT performed during the follow-up period. One important difference from these prior series is that ICT was repeated after further treatment, which increased our verified final intraoperative SFR from 61% to 78% during the initial ICT case and to 87% for all stages, with a modest radiation dose.
Ultimately, we were unsuccessful in the treatment of residual identified stones (>3 mm) in 25% of these cases, even after subsequent staged treatments. This is similar to the 30% and 43% rates reported in the respective studies. Consistent findings of untreatable residual calculi in some patients are critical to informing realistic expectations overall with treatment. In addition, it may be advisable to establish a time limit after identifying residual stones to avoid unnecessarily prolonged surgery.
Combining reduced-dose protocols and collimation techniques makes it possible to obtain ICT with exceptionally low radiation exposure, using either an RMPFS or a mobile CT scanner. Despite dose reduction, discrete calcifications <1 mm could still be clearly observed. In particular, after laser stone dusting, these were often too small to be effectively measured. Our CARE protocol patients had 94% lower dose than that reported by van den Broeck et al (personal communication), 10,17 89% lower than Kingma et al, 11 and 78% lower than our first patient, who had standard protocol imaging, but the same degree of collimation (12 cm).
Similarly, the two O-Arm ICTs had a 93% reduction in dose relative to preoperative CTs. One study found that mean ERD of KUB in contemporary practice was 2.15 mSv, much higher than the 0.7 to 0.8 mSv commonly reported, 18 and also higher than most of our ICTs. ERD <2 mSv was achieved in 90% of CARE protocol studies (including a patient with BMI = 46.75 kg/m2) and in both O-Arm cases (BMI = 35.5 kg/m2), meeting a previously proposed definition for ultralow-dose (ULD) CT. 19
ICT during retrograde URS has not been reported previously. All URS patients were confirmed to be clinically stone free, although one patient required further treatment after the initial ICT. Intriguingly, this patient had the smallest stone (9 mm) in the transplanted kidney. In addition, ICT during one second-stage URS case after initial endoscopic combined intrarenal surgery (ECIRS) proved critical to locating residual stones.
A specific advantage of ICT after stone dusting is that tiny fragments can be directly dispersed with directed flushing immediately before imaging, which can be useful for documenting complete treatment. Fragments that are too small to effectively basket can subsequently accumulate in the calix. Such collections can be incorrectly interpreted as a larger residual stone and, if not recognized, could prompt inappropriate secondary interventions.
However, appearance of “dust” can increase challenges in interpretation, as demonstrated in one case of a patient who subsequently became obstructed with a 6 mm stone. However, retrospective review did then identify the stone on the initial ICT. Paradoxically, this supports that properly interpreted ICT has potential to improve URS outcomes as well. Given the extremely low doses and demonstrated benefits, we intend to expand the use of ICT to smaller stones treated ureteroscopically, at least in select cases.
We estimate that the performance of ICT added ∼30 minutes, on average, to the surgical time. This largely reflects the steep learning curve of the procedure and additional endoscopic evaluation and/or treatment in several cases. Notably, both residual iodinated contrast artifact and vascular calcification can be mistaken for stones, which prompted additional assessment after ICT and added at least 15 minutes to the operative time in two cases (Fig. 6).

Iodinated contrast artifact seen during bilateral ureteroscopic treatment with dilute (50:50) iodinated contrast used during the left stone treatment before treating the right side (no contrast used).
One strategy to avoid contrast artifact on ICT when contrast is needed is to use CO2-digital subtraction pyelography technique. 20 In the most recent cases, only ∼10 additional minutes was required to perform and interpret the study. One frequent challenge with RMPFS is impending collisions of the system's flat plates (which need to be clear throughout a 200° rotation) with the patient or table during the practice spin. Although the system anticipates such collisions as an integrated safety feature, adjustment of the table and/or patient position is necessary.
As this was a reportable QI project involving a change in routine practice for all patients, there are inherent limitations compared with a research study. First, a prospective randomized control group for comparison was not permissible, although comparison with a historical cohort was allowed. Nevertheless, patients were their own controls for imaging-related radiation comparisons. Second, our practice has been to only selectively obtain CT scans after PCNL because our radiology department does not currently offer low-dose or ULD stone protocol CTs.
Instead, we have favored a combined ultrasound and KUB approach for imaging follow-up to limit radiation exposure. This makes a direct comparison with historical patients difficult regarding SFR. Because our prior practice did not involve routine postoperative CT and we were satisfied with the quality of ICTs, routine performance of studies involving ionizing radiation solely to validate imaging studies would have been unethical.
Apart from the additional times directly related to ICT already described, operative times in this report are longer than typically expected for several reasons. First, by facility convention, nurse-reported times begin with initial cystoscopy and include time of repositioning and redraping before making initial incision, and then extend beyond the time of closure or scope removal to include drape removal, patient cleaning, and repositioning to supine when initially in prone or lithotomy position. These factors overstate operative times as usually reported, especially for PCNL cases.
“Total operative time” is the sum of all cases performed under anesthesia, including contralateral treatment not originally intended during a total episode of care. To illustrate, one case reported as 997 minutes “total operative time” involved large bilateral stones (3.9 and 2.5 cm, respectively). Despite intention for percutaneous treatment, these stones were treated exclusively retrograde using holmium laser (12 W/100 W). This was because of severe stone impaction that precluded appropriate access by either the interventional radiologist or the urologist (28 and 9 minutes of fluoroscopy time, respectively). A contralateral obstructing stone event then prompted bilateral URS from the third case onward, because the patient declined contralateral percutaneous treatment. Complete treatment of both sides involved six separate surgical procedures over a 7-month period.
Additional factors impacting operative times include that our facility provides the initial experience with endoscopy for first and second year trainees, who most typically participate in these cases; inconsistent operating room nurse support especially during the COVID-19 pandemic; a transition from prone PCNL with fluoroscopic access to supine PCNL with primary ultrasound-guided access in the year before initiating the project for the corresponding author; a learning curve for using the hybrid room in postintervention cases; and early limitations in power supplies for our 120 W holmium laser system.
One reasonable criticism of our analysis is that our postintervention cohort included both primary PCNL and URS cases, whereas the historical cohort included only initial PCNL cases. Unfortunately, many PCNL-eligible stones at our facility were preferentially treated retrograde with high-power holmium laser systems before implementing the ICT intervention, but these patients could not be easily identified retrospectively. This likely explains the larger overall stone size before intervention (3.9 cm vs 3.1 cm); although this difference was not significant (p = 0.10), the analysis may have been underpowered.
Although the ICT intervention PCNL and URS subgroups were objectively similar by stone size and GSS (Table 4), and the intervention cohort to the retrospective group overall (Table 1), these measures may not adequately account for patient outliers, surgeon selection biases, or differences in technologies used. Thus, it may not be entirely fair to compare SFR of the intervention group (or either subgroup) with the retrospective PCNL cohort. Nevertheless, this does not diminish from the overall benefit of reduced radiation exposures with ULD ICT.
Another potential critique is that ICT using RMPFS and a portable scanner were both included in this analysis. Although these are different systems, the coaxial imaging principles are fundamentally the same. Unlike a formal research protocol, the description of two systems represents a real-world experience consistent with the goals of the project, which was to optimize care for all patients. Despite having ready access to a hybrid room, the authors have encountered unavoidable conflicts such as emergency vascular cases. In the authors' opinion, inclusion of an O-Arm backup imaging system, and our finding that ULD ICT can be achieved with it as well, is ultimately a strength of this report.
Finally, a tremendous opportunity for reducing total radiation exposure for patients revealed in this project is radiation from preoperative CT imaging. Most preoperative CT scans were ordered by nonurologists (emergency room, primary care, endocrine, or inpatient medicine) or were performed at outside facilities, before urology referral. Unfortunately, our facility does not currently offer low-dose or ULD stone protocol CTs. However, our radiology colleagues have expressed willingness to consider implementing such protocols in the future.
Conclusions
ULD ICT during endoscopic stone procedures was performed using either the RMPFS in a hybrid room or a portable imaging system in a traditional operating room. Extremely low-dose protocols allow multiple ICTs to be performed, when indicated, to achieve a stone-free status, while allaying some of the growing concerns about cumulative radiation exposure for both patients and clinicians. Improvements in SFR, staged procedure rates, and overall radiation doses support the continued routine use of ICT in our practice.
Footnotes
Acknowledgment
M.D.S. thanks Dr. Duke Herrell for providing training in hybrid room PCNL in 2011–12, which helped make this project possible.
Authors' Contributions
X.G.G. was involved in investigation and writing—original draft (equal) and review of revision. E.C.B. was involved in conceptualization, methodology, investigation, formal analysis, writing—review and editing of original draft, and revision. M.D.S. was involved in conceptualization, methodology, investigation, software, formal analysis, writing—original draft (equal) and revision (lead), observation, project administration, and supervision.
Ethical Approval
IRB Protocol: COMIRB 21-3896. The Colorado Multi-Institutional IRB (COMIRB) reviewed our protocol and determined that this project qualifies as a QI rather than human research. Therefore, additional patient consent is not required. Publications related to this project were authorized by the IRB. The findings of the QI project may not be generalizable to other patients and facilities.
Data Access Statement
All relevant data are within the article and accompanying tables.
Author Disclosure Statement
None relevant to the project or article. M.D.S. is a consultant for Laborie/PrimeSight. Siemens has provided technical training and support related to the RMPFS, including customized lower radiation settings for fluoroscopy (not coaxial imaging). They did not attempt to influence the manuscript and did not review the manuscript before submission or revision.
Funding Information
No external funding was received.