
Abstract
The Endourological Society, the premier urologic society encompassing endourology, robotics, and focal surgery, is composed of a diverse group of >1300 urologists. However, limited information has been collected about society members. Recognizing this need, a survey was initiated to capture data regarding current member practices, as well as help the Society shape the future direction of the organization. Presented herein is the inaugural Endourological Society census report as the beginning of a continued effort for global improvement in the field of endourology. Using a REDCap® database, an email survey was circulated to the membership of the Endourological Society from May through June 2021. Twenty questions were posed, categorizing member data in terms of epidemiology/demographics, practice patterns, member opinions, and future educational preferences. Responses were received from 534 members, representing 40.3% of membership. Data demonstrated that the average age, gender, race, and ethnicity of the typical Society member respondent is a 48-year-old Caucasian male working in the United States, with a mean of 25 years in practice. Retrograde endoscopy and percutaneous nephrolithotomy were identified as the most common practice skills, and 50% of members are involved in robotics. Importantly, the census confirmed that the World Congress of Endourology and Technology remains popular with Society members as a means of educational advancement. To sustain and advance the Society, information is required to understand the career interests and future educational desires of its members. This inaugural census provides crucial data regarding its membership and how the Society can achieve continued success and adjust its focus. Future census efforts will expand on the initial findings and stratify the data to elucidate changes in the needs of the Society as a whole. Circulating an annual census will allow for continued improvements in the field of endourology and, ultimately, better care for urologic patients.
The Organization
The Endourological Society is a nonprofit organization founded in 1983 by a group of international urologists and incorporated in 1984. The Society strives to globally promote education and training in endourology by means of meetings, fellowship training sites, and the Journal of Endourology. The Society oversees international training sites where urologists can receive broad training in endourology with emphasis on laparoscopy, robotic surgery, image-guided therapy, percutaneous procedures, ureteroscopy, extracorporeal shockwave lithotripsy (SWL), and other new technologies. The Society is committed to being at the forefront of innovation and discovery of new technologies, techniques, and research. Our aim is to promote minimally invasive or noninvasive management of both benign and malignant urologic conditions.
The Mission
The mission of the Endourological Society is to improve the lives of patients with both benign and malignant urologic conditions by reducing the morbidity of invasive treatments through novel technology, innovative techniques, and noninvasive medical management relevant to our discipline. By virtue of its annual World Congress of Endourology and Uro-Technology, international fellowship programs, and the Journal of Endourology, the Society is committed to the global promotion of research, education, and evidence-based medical and surgical practice of endourology and minimally invasive urology.
The Vision
Our vision is to innovate, discover, and disseminate new minimally invasive procedures and noninterventional medical management to ultimately replace standard incisional surgery with less morbid equally effective alternatives, thereby improving patient health worldwide.
Introduction
As a prominent international urologic organization, the Endourological Society is committed to serving the global urologic community. The Society strives to promote the education and training in endourology through international meetings, fellowship training programs, and the Journal of Endourology. The Endourological Society Census is a broad inclusive survey of the demographics, practice patterns, and opinions of its members.
This inaugural report serves as a benchmark for which to gauge future innovation and growth in the field of endourology. The results of the census depict the current state of the endourology workforce and can elucidate the needs of the Society members. Future census reports will expand on the initial findings, allowing for global improvements in the field of endourology and, ultimately, providing better care to our urologic patients.
Methods
The census was created and distributed by the Endourological Society's Data Committee. Using a REDCap® database, a confidential email survey was circulated to a total of 1310 Society members. The survey remained open from May through June 2021 and Society members were sent email reminders twice during this timeframe. No individual patient or protected health information were used during this study, thus IRB approval was not necessary. Twenty questions were posed, categorizing member data in terms of epidemiology and member demographics, individual and group practice patterns, member opinions, and future education preferences.
Epidemiology/Demographics
Age, gender, race, and ethnicity
Contributing to the census were 534 respondents, representing 40.3% of the 1310 total Endourological Society members at the time of the survey. Of the practicing urologists surveyed, 8.1% are women, which is congruent with the data collected by the 2021 AUA Census that only 10.9% of practicing urologists are women. 1 Stratifying the data by gender does reveal that women offer woman-related urologic care more often than their male counterparts, but sample size limits the ability to determine statistical significance.
The average age, gender, race, and ethnicity of the typical Endourological Society member respondent is a 48-year-old Caucasian male working in the United States. Member age ranges from 28 to 84 years. Among respondents, 479 (90.7%) are men and 43 (8.1%) are women. Only 1.2% identified as nonbinary, preferred to self-describe, or did not disclose their gender. Most respondents identify as White (50.5%) with the second-highest category being Asian (22%) followed by Hispanic, LatinX, or Spanish (13.5%). Middle Eastern or North African (7%), Black, African American, or African (5.5%), American Indian (0.2%), and Native Hawaiian or Pacific Islander (0%) rounded out the least represented.
Practice location, duration, and type
Endourological Society members work in many locations (Fig. 1). Interestingly, although the Society is an organization with international representation, a large proportion of respondents are North American (45%). Respondents from a total of 56 countries are represented in this survey, with the largest proportion of respondents from the United States (38.6%), followed by Brazil (5.7%), Canada (5.2%), and Colombia (3.9%). A total of 13.7% of respondents practice in South America, 10.4% in Western Europe, 6.8% in the Middle East and North Africa, 6.8% in Southeast Asia and the Pacific, 5.2% in Eastern Europe, and <4% of respondents reported practicing in one of the following geographic locations: Central America and the Caribbean, Scandinavia, South Asia, Northern Asia, East Asia, and Sub-Saharan Africa.
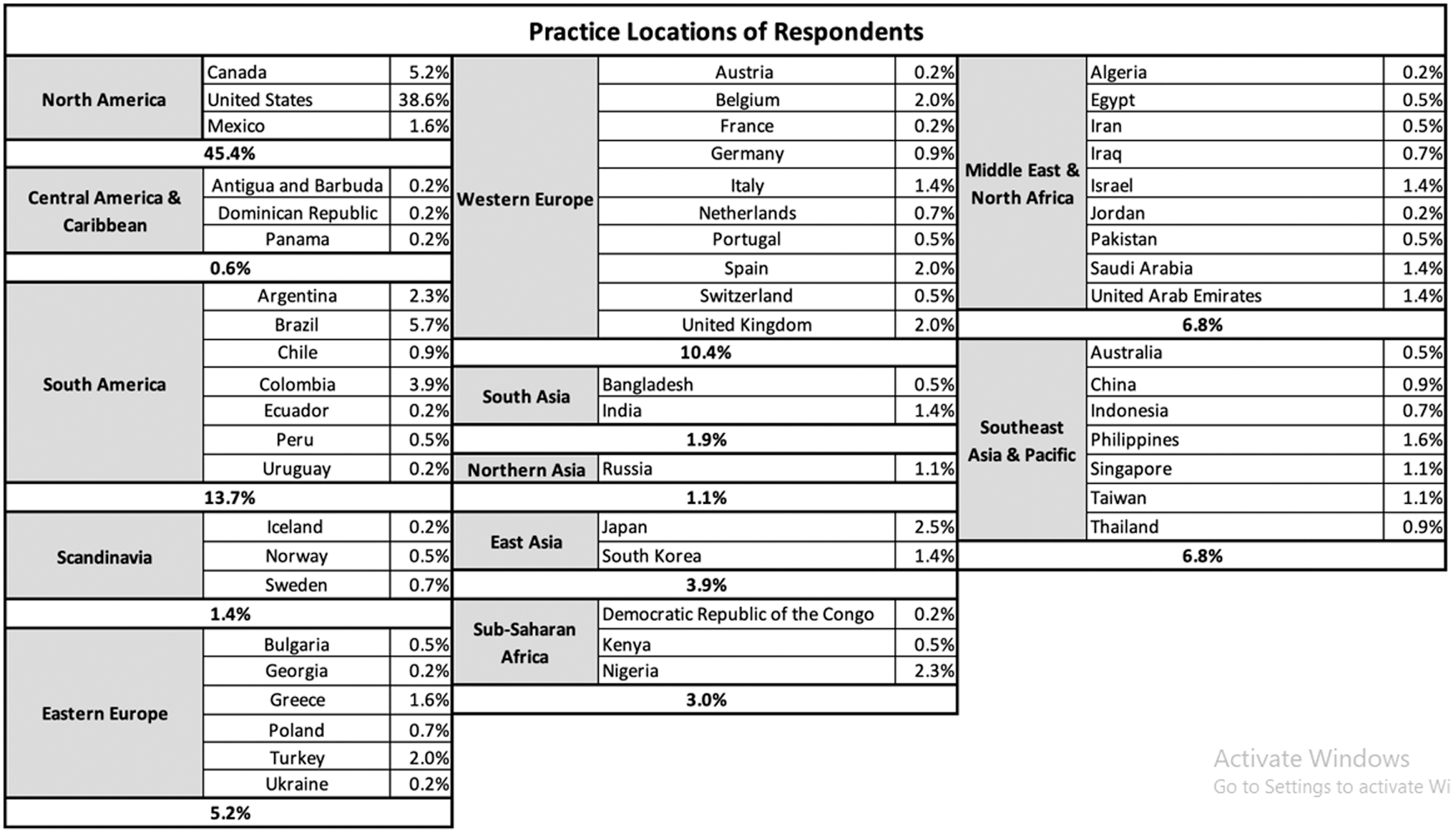
Practice locations of survey respondents.
Duration
Of the 431 respondents, 25.3% report working >25 years (Fig. 2). Respondents practicing between 1 and 25 years were relatively similar with the largest difference between those who have worked 6–10 years (12.8%) and 11–15 years (17.2%).
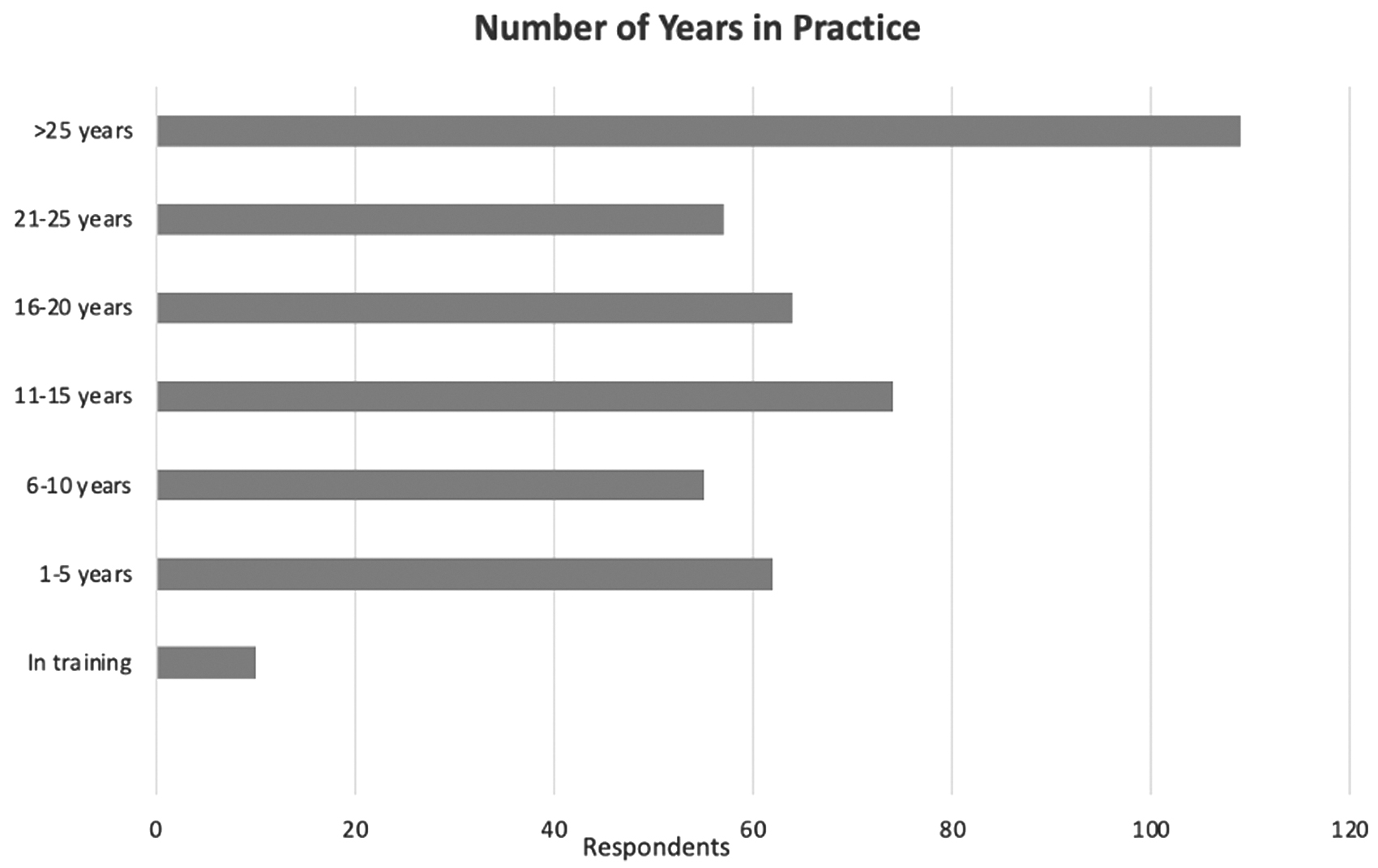
Demonstration of the total number of years in practice for all respondents (n = 431).
When isolated by gender, the data (Fig. 3) reveal that there are many more men compared with women in advanced practice over 25 years compared with junior urologists practicing 1 to 5 years. Of all the respondents, 62% of men and 67% of women completed a fellowship in endourology, laparoscopy, or robotics.

Comparison of the number of years in practice for men (n = 392) vs women (n = 36) respondents.
Types of active employment
A majority of respondents work full time (92.2%, Figs. 4 and 5). In the full-time cohort, 64.6% are employed in academic practice with the rest of respondents practicing in nonacademic settings (large or solo private practice, military, government, multidisciplinary, etc.) These trends are similar to the part-time cohort in which 50% of urologists were employed in an academic setting vs nonacademic.

Employment type of actively practicing respondents (n = 424).

Employment model stratified by full-time (n = 390) and part-time employment (n = 23).
Practice Focus
Skills and expertise of Endourological Society members
Figure 6 summarizes the findings of a total of 430 survey respondents. Overall, members of the Endourological Society are mostly involved in the field of endourology: complex retrograde endoscopy is performed by almost all the surveyed panel (87%), followed by percutaneous nephrolithotomy (PCNL) (80%). General management of urologic diseases is practiced by the majority, with 77.6% and 74.1% offering medical management of urolithiasis and general urologic practice, respectively. Advanced benign prostatic hypertrophy (BPH) surgical treatment is performed by 62% of respondents. In total, 60% of the respondents are engaged in the field of uro-oncology. A total of 61% and 50% offer laparoscopy and robotics in their current practice, respectively.

Skills and expertise currently offered in own practice (n = 430).
A smaller number (<25%) are engaged in infertility, women's health, and female pelvic medicine and reconstruction; pediatric urology is performed by 15.2% of respondents. Clinical research is carried out by 43.7%, consistent with the academic employment of 62% of respondents. Stratifying the data by gender reveals that 26.9% of men offer women's health and/or FPMRS services compared with 42.9% of women. This observation that female urologists offer woman-related urologic care more often than their male counterparts is interesting, but sample size limits the ability to determine statistical significance. In addition, a similar percentage of men and women respondents perform clinical research (43% vs 48.6%, respectively).
Minimally invasive surgery
Minimally invasive surgery (MIS) has gained worldwide acceptance; indications for robotic and laparoscopic surgeries have broadened. 2,3 Among the Endourological Society members who responded, 70% perform laparoscopy. However, for the vast majority of them (93%), laparoscopic surgery encompasses <50% of their clinical practice. As far as robotics is concerned, 49.4% of respondents perform robotic surgery, 28.6% do not have a robotic platform at their institution, and 22% do not perform robotic surgery despite access to a robot.
Of those respondents who engage in robotic surgery, 33% are highly engaged with robotics in their clinical practice, defined as >50% of their own practice. This differs from laparoscopic surgeons, with only 7% of them devoting more than half of their working time to laparoscopy. According to Tummers et al, laparoscopic spread has been accompanied by increasing hospital volumes, with a disproportionate rise in the number of surgeons performing laparoscopic procedures; therefore, surgeon individual volume has remained low and may have even decreased for some interventions. 4
As far as oncologic indications are concerned, MIS has been endorsed by international guidelines that state that all approaches—laparoscopic, robotic, and open—can be recommended for radical prostatectomy, partial nephrectomy, and radical cystectomy. 2,3 Among the Endourological Society members surveyed, a majority of laparoscopic and robotic users utilized MIS techniques for their oncology practice (Fig. 7A, B).
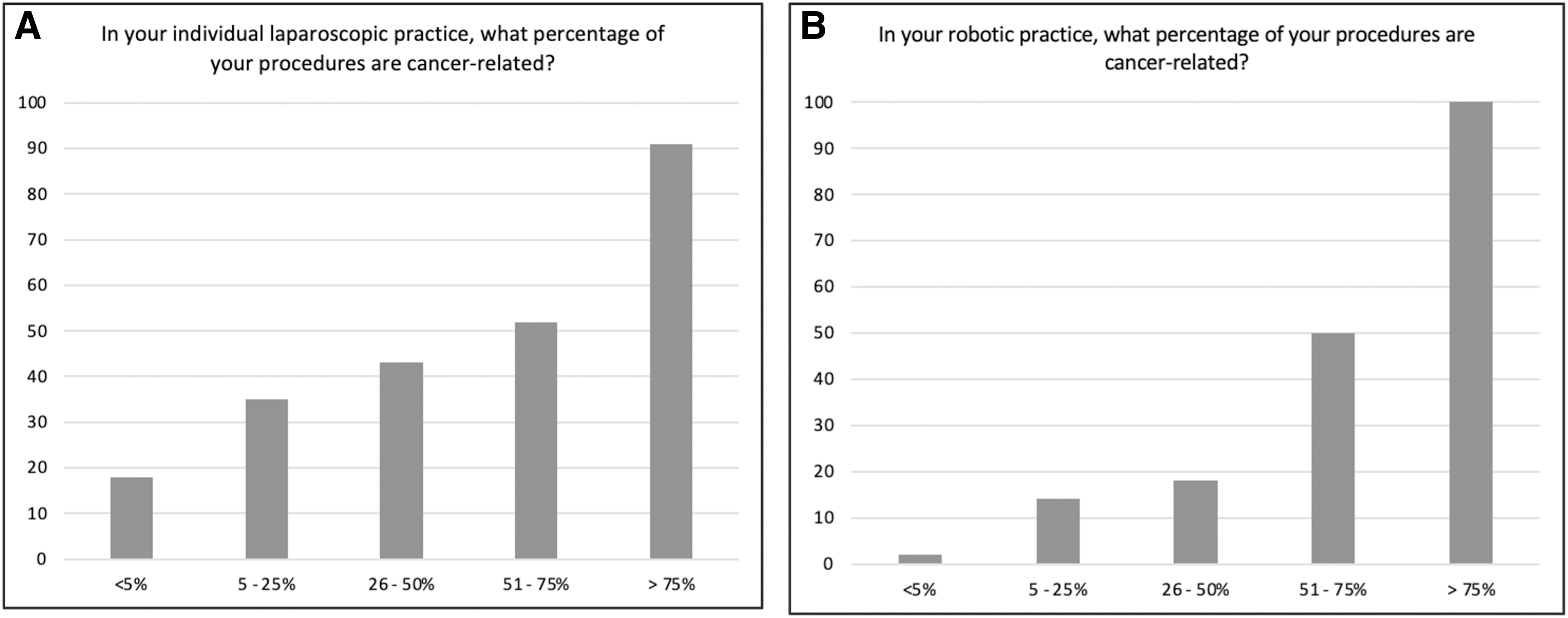
Demonstration of the percentage of a surgeon's laparoscopic
Reconstructive surgery, including urinary diversion and ureteral stricture management, is more often performed within the robotic setting (67.6% vs 27.5% for robotic and laparoscopic surgeons, respectively). Similarly, robotics is utilized more than laparoscopy for benign disease (58.5% vs 36.2%, respectively), including simple prostatectomy and diverticulectomy.
Single-port surgery is performed by a small number of surgeons (11%), with only 33% having an annual caseload of >20 procedures. As far as perspectives on new emerging robotic platforms are concerned, 79% expect a reduced cost for novel platforms, whereas 60% expect technologic advances; 33% expect easier adoption with a simpler learning curve and 8.4% hope that novel platforms perform closer resemblance to laparoscopic surgery.
Endourology/stone disease
More than a half of the respondents of the survey (53%) are highly involved in endourology for stone disease, accounting for >50% of their individual clinical practice. Ureteroscopy is the most performed procedure, with 87% of surgeons performing it frequently or very frequently. PCNL is frequently or very frequently performed by 55% of respondents, with 60% of surgeons having an annual caseload of >20 PCNL procedures. The majority of urologists (86%) obtain their own percutaneous access. Despite the introduction of the supine approach, 5 a high number still adopt an exclusive prone position (47.5%), whereas the supine alone is used by 16.3%. Overall, 36% of responding members use either prone or supine access for PCNL.
Almost all endourologists (91%) use either stone dusting and fragmentation with basket extraction; the time spent for dusting or fragmentation is equally distributed within stone removal practice. The practice of using only dusting or only fragmentation is used only by a small number of endourologists.
Overall, 68.1% of respondents adopt SWL for stone management. However, only 19% state to perform it as a frequent procedure and more than a half (56%) have an annual caseload of <20 shockwave treatments. Surprisingly, general/local anesthesia or sedation is still highly employed for SWL, whereas only 19% prefer not to use anesthesia at all or use nonsteroidal anti-inflammatory drugs administration. Nevertheless, SWL is still the most desired approach by the patients because of the lesser degree of perceived invasiveness, according to a recent survey by Walters et al. 6
Metabolic stone management is delivered by 83% of the respondents; however, only half declare a frequent engagement in outpatient medical practice with stone drug administration.
Endourology/BPH treatment
Endoscopic management for BPH is considered one of the most performed surgeries in urology. The introduction of new technologies such as laser energies and miniaturized instruments has allowed a reduction of the morbidity of such procedures, with indications to endoscopy extending also to larger prostates. 7
Within the Endourological Society, 84% of responding members perform endoscopy treatment of BPH. However, the time spent for the procedure is quite low for roughly half of the respondents; only 12% dedicate more than half their clinical practice to BPH surgery.
Despite the introduction of minimally invasive alternatives, transurethral resection of the prostate still remains the most performed approach for 74% of respondents, whereas enucleation is offered by 45% of them. The diffusion of novel technologies is still moderate and variable: photoselective vaporization (PVP) followed by holmium laser enucleation of the prostate (HoLEP) are the most available ones (50% and 42%, respectively). When available, 45% and 26% of surgeons offer PVP and HoLEP to the majority of their patients undergoing BPH treatment, respectively. Thulium enucleation for BPH is offered half the time or more often for only 5.6% of urologists. Similarly, UroLift® and Rezūm™ have never been used by 76% and 79% of the respondents, respectively.
Education
The first annual census confirmed that the World Congress of Endourology and Technology (WCET) remains popular with our membership. Nearly 46% of those members who responded to the survey reported attending the meeting in 2019. The most frequent reasons for attendance were to acquire updates to management strategies (59%), acquire technical updates to procedures (56%), and recognize new or emerging technology (55%).
Interestingly, educational courses were not a high priority for WCET meeting attendees, with only approximately one-third of meeting attendees (35%) having attended the offered educational (didactic or hands-on) courses. Of those who did attend the offered educational courses, they attended an average of 3.6 courses. Regardless of their attendance of educational courses, respondents would be most interested in future educational courses focusing on surgical techniques for nephrolithiasis (78%) and BPH (58%), and the medical management of nephrolithiasis (61%). Other sessions such as the plenary with debates, discussion of new technology, guideline updates, evidence-based practice reviews, and nightmares were all universally viewed as either essential or very important (all >80%).
The most popular plenary topics were New Technology in Endourology (93%), Debates (88%), and Where is the Evidence (82%) with the least popular being Challenge the Expert (68%) and Society Sponsored (36%). Semi-live surgery remains popular with two-thirds of respondents confirming that this session is either essential or very important (64%). Although only 35% of WCET attendees participated in an educational course, didactic instructional courses were rated as favorably as hands-on courses, with 75% and 70% viewing them, respectively, as either essential or very important.
There was significant interest in future WCET being available as a virtual or live-streamed event (89%). However, the overwhelming majority of respondents felt that the virtual educational (88%) and social or networking (95%) experience was either equivalent or worse than an in-person version (Fig. 8A, B).
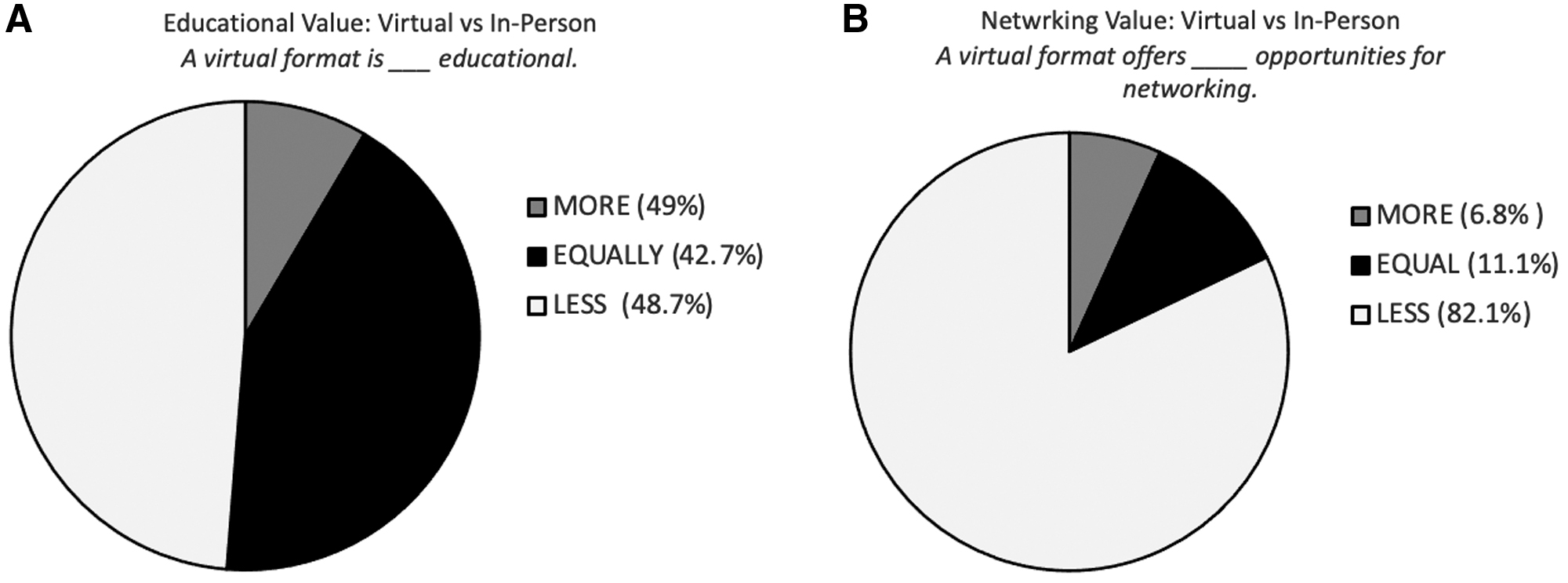
Opinion of the educational
In terms of payment options for future educational courses, there was an equal distribution of interest between add-on pay-per-course (39%), add-on all-inclusive course pass (25%), and inclusion of all courses in the general meeting fee (36%).
Additional educational offerings that can be sponsored by the Endourological Society were also queried. In-person synchronous formats were still highly requested. An accredited clinical observership, short-term fellowships of 1 to 3 months, short-term international exchanges of 1 to 2 weeks, and master classes of surgical techniques of 1 day were regarded as either essential or very important for respondents (all >50%). Similarly, virtual or asynchronous formats were also of value. For example, an on-demand video library of surgical technique video modules was either essential or important for three-quarters of respondents (75%). A nearly identical number of respondents agreed that an endourology “update series” was either essential or important (76%).
Respondents were given the opportunity to provide additional educational topics of interest that were not included in the survey. In total, 41 respondents (10%) were interested in other topics not listed explicitly in the survey. Four persons demonstrated a strong desire for the continuance of the “Masterclass in Endourology & Robotics” webinar series. One person recommended the creation of online videos or podcasts with content experts in the field to discuss major themes of endourology. Another member would be highly interested in prerecorded videos of endoscopic procedures (e.g., HoLEP) with a voice-over narration from the performing urologist with discussion of the procedure as it occurs in real time. Other commonly mentioned topics of interest include brachytherapy, adrenalectomy, office-based ultrasound for the diagnosis, treatment, and surveillance of prostate cancers, pediatric stone management, and focal therapy for prostate cancer.
Conclusion
The census will be conducted annually and reports will be made available online at
Footnotes
Authors' Contributions
Writing—original draft (lead), writing—review and editing (equal), methodology, and data curation by H.M. Writing—original draft (supporting), writing—review and editing (equal), methodology, and data curation by L.S. Writing—review with some editing and visualization by V.S. Conceptualization (supporting) and writing—review and editing (equal) by A.G. Conceptualization (supporting) and writing—original draft (supporting) by M.S., M.B., A.E.K., and B.R. Conceptualization (supporting), writing—original draft (supporting), and writing—review and editing (equal) by J.B.Z. Conceptualization (lead) and project administration by T.D.A.
Author Disclosure Statement
All authors have nothing to disclose, including, but not limited to, competing interests, personal financial interests, or employment-based interests that may inappropriately influence or affect the integrity of the submission.
Funding Information
No funding was received for this article.