
Abstract
Introduction:
Radical prostatectomy (RP) is one of the standard treatments for localized prostate cancer. However, in terms of functional outcomes, there are aspects that still need improvements. We designed this prospective phase I/II clinical trial to assess the safety, clinical feasibility, and functional outcomes of hypothermic robot-assisted RP (RARP).
Material and Methods:
Twenty patients with preoperative total 5-item International Index of Erectile Function scores ≥12 points, scheduled for RARP, were enrolled in the study. Pelvic hypothermia was induced using an endorectal cooling device (BelloCool System). The primary outcome was the completion rate of the planned hypothermic RARP. Secondary outcomes included the drop in neurovascular bundle (NVB) temperature, adverse (including device-related) events, continence, and potency recoveries, and postoperative quality of life. Contemporaneous patients (propensity score-matched for baseline characteristics) who satisfied the inclusion criteria were included in the control group.
Results:
The completion rate of the planned hypothermic surgery was 100%. The nadir NVB temperature was 24.9 [22.4, 28.2]°C, which was 10.2 [7.0, 13.1]°C lower than the nadir core body temperature. There was no device-related adverse event, and bowel function was well preserved for the whole follow-up period. At 12 months postoperatively, potency and continence recovery rates were higher in the hypothermic group than in the control group (40% vs 15%, p = 0.027 and 95% vs 80%, p = 0.167, respectively). The Kaplan–Meier curve showed faster recovery rate of potency in the hypothermic group (hazard ratios = 3.46, log-rank p < 0.01).
Conclusions:
Hypothermic RARP using the BelloCool™ endorectal cooling system is safe and feasible. A large-population-based randomized controlled trial is needed to confirm the potential for a benefit in continence and potency recovery.
Introduction
Prostate cancer (PCa) is the most common cancer in men, 1 localized disease is diagnosed in ∼75% of patients and are amenable to surgical treatment. 2,3 One of the important factors affecting decision-making regarding the treatment option for localized PCa is the deterioration of quality of life (QoL) after surgical treatment, especially regarding postoperative incontinence and erectile dysfunction (prevalence, 4%–31%). 4,5 Accordingly, the COMPARE study recently reported that patients with localized PCa were willing to trade cancer-specific survival for improved QoL (mainly determined by urinary and sexual functions). 6
Constant efforts have been made to improve functional outcomes after radical prostatectomy (RP). The Swedish Laparoscopic Prostatectomy Robot Open (LAPPRO) trial proceeded for 2 years, and its extended follow-up of 8 years demonstrated that robot-assisted RP (RARP) had better functional outcomes than open retropubic RP. 7,8 Clinicians have also been working to develop new surgical techniques such as meticulous bladder neck and apical dissections and artery- and nerve-sparing surgeries (with limited counteraction with the neurovascular bundle [NVB]). 9 An additional approach is to decrease acute inflammatory damage (caused by incision and thermal injuries) by inducing local hypothermia during surgery. 10
In this study, we performed a hypothermic surgery using a newly developed rectal cooling system, BelloCool (CEBIKA, Uiwang, South Korea). We earlier confirmed its safety and efficacy in a previous preclinical animal study. 11 This prospective phase I/II first in-human trial aimed to confirm its safety and feasibility, and functional outcomes in patients undergoing RARP.
Materials and Methods
Ethics statement
This study was approved by the Institutional Review Board of Seoul National University Hospital, Seoul, Republic of Korea (1906-162-1045). Written informed consent was obtained from all the patients.
Study design and patients
Male patients aged 19 to 80 years who (1) had pathologically proven PCa, (2) underwent RARP, (3) had a preoperative total 5-item International Index of Erectile Function (IIEF-5) score ≥12 points, (4) had an Eastern Cooperative Oncology Group performance status of 0 or 1, and (5) could read and agree with the contents of the informed consent form were included in the study. Patients who received prior treatment for PCa underwent radiation therapy/surgery in the pelvic cavity, or refused to participate in the study were excluded.
We prospectively enrolled 20 patients who consulted at Seoul National University Hospital, a tertiary referral hospital between October 2019 and April 2020. All the patients underwent conventional six-port transperitoneal RARP through the anterograde approach (with minor modifications). 12,13 Van Velthoven urethrovesical anastomosis and posterior and anterior reconstructions were performed. 12 Two surgeons who had already performed a total of 1842 and 120 RPs (of all types), and 991 and 83 RARPs, respectively, were involved in the study.
Pelvic hypothermia induction
Pelvic hypothermia was induced using the BelloCool system 11 (Fig. 1). The rectal balloon was optimally designed in two ways to induce effective cooling: (1) it was curved (to fit with the anatomical angle of the rectum) and (2) had an asymmetrical elliptical shape (to optimize the contact area with the prostate surgery cooling site). The lubricated rectal balloon was inserted inside the anus before robot docking and inflated with cold saline (4°C), which was automatically adjusted in real time according to intrarectal pressure measurement. After prostate was resected, it was removed before anastomosis.
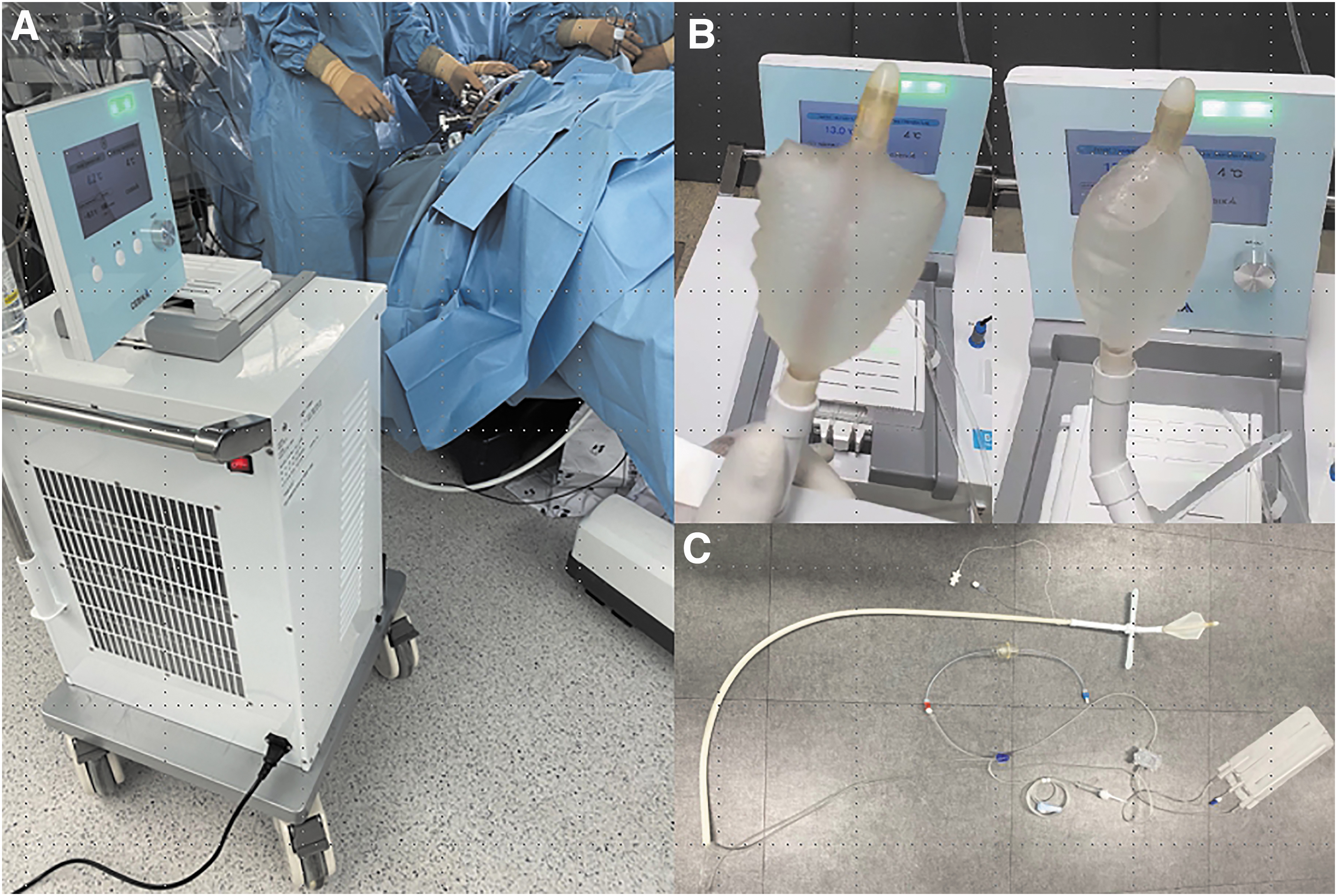
Bellocool endorectal cooling system.
Intraoperative temperature measurements
For core body temperature measurements, an 18F esophageal probe (MediTop, Gyeonggi-do, Korea) was inserted into the esophagus. Core body temperature was defined as the lowest esophageal temperature measured during surgery. For intracorporeal NVB temperature measurements, a 9F esophageal probe (MediTop) was inserted through a 5-mm assistant port, and the temperature was measured directly along the anterior surface of the NVB. Proximal NVB temperature (right and left sides) measurements were performed immediately before the NVB dissection was initiated. Distal NVB temperature (right and left sides) measurements were performed after the NVB dissection was completed. The nadir NVB temperature was defined as the lowest NVB temperature among the four independent measurements (right proximal, right distal, left proximal, and left distal) for each patient. The maximum device-induced temperature drop was defined as the difference between the nadir core body and NVB temperatures.
Study outcomes
The primary outcome was the completion rate of the planned surgery. The secondary outcomes were (1) the drop in NVB temperature compared with the core temperature, reflecting the effectiveness of hypothermia; (2) all adverse events and device-related events, reflecting the safety of hypothermia; (3) postoperative continence and potency recoveries at up to 12 months; and (4) postoperative changes in QoL based on questionnaire score items.
Potency and continence were evaluated at baseline and at 1, 3, 6, and 12 months postoperatively. Potency recovery was defined as an erection sufficient for penetration, whereas continence recovery was defined as zero pad usage. Data from patient-reported questionnaires, which included the five-level version of EuroQol-5 dimensions (EQ-5D-5L), the Expanded Prostate Cancer Index Composite for Clinical Practice (EPIC-CP), and the IIEF-5, were collected at baseline and at 1, 3, 6, and 12 months postoperatively. The validated Korean versions of all the questionnaires were used. 14 –16
Selection of control patients
For comparison of treatment efficacy, control patients were selected. We primarily included patients registered in the SUPER-PC-RP (Seoul National University Enrolled Registry-Prostate Cancer-Radical Prostatectomy) prospective cohort, 17 who underwent RARP during the same period (October 2019 to April 2020). The patients in the cohort had all the clinical information analyzed in this study, thus making it possible to compare every parameter between the two groups. We applied the same inclusion and exclusion criteria applied in the treatment group (as a preferential method to match baseline characteristics), and thus recruited 168 patients.
Subsequently, to remove selection bias, we performed propensity-score matching. One-to-one matching without replacement was performed using the nearest-neighbor match on the logit of the propensity for seven variables: age, preoperative PSA level, prostate volume, clinical stage, International Society of Urological Pathologists (ISUP) grade group, and right and left nerve-sparing grades. Specifically, among the 168 candidate patients, the control patients were 3:1 matched (n = 60) with the treatment group, with adjustments for the aforementioned seven variables.
Statistical analysis
Functional outcomes, completion rate, and adverse events were evaluated in all patients. Statistical comparisons were performed using the chi-square test (for categorical variables) and the t-test (for continuous variables). Kaplan–Meier analysis was used to analyze the time to potency recovery. Health-related utility values were converted using a validated conversion formula derived for the Korean population. 15 Statistical significance was set at p-values <0.05.
Results
Safety and direct efficacy of the hypothermic surgery
A total of 20 patients with median age of 69 (interquartile range [IQR]: 63, 73) years were enrolled in this study. The completion rate of the planned hypothermic surgery was 100%. NVB temperature was measured as a direct indicator of hypothermic efficacy. The intrarectal balloon temperature was maintained at a median of 4.1 [IQR: 4.0, 4.3]°C. The nadir NVB temperature was 24.9 [22.4–28.2]°C, which was 10.2 [7.0, 13.1]°C lower than the nadir core body temperature (Table 1). No device-related adverse event was observed.
Intraoperative Temperature Measurements
Values are presented as median [IQR].
IQR = interquartile range; NVB = neurovascular bundle.
Five patients experienced mild postoperative adverse events during the first 90 days, but there were no Grade III–V Clavien–Dindo complications 18 (Supplementary Table S1). There was one patient with mild hemoglobin drop (−2.4 g/dL) postoperatively among 20 patients (−1.2 [−1.5, −0.7]) (g/dL) (Table 3). During the surgical procedure, there was no observed damage in the rectal wall caused by the endorectal cooling device. And for the whole follow-up period, there was no significantly meaningful difference in patient-reported bowel function between the hypothermic group and the control group (Supplementary Table S2).
Comparison of patient characteristics
There were no differences in baseline characteristics between the two groups, indicating that the preoperative characteristics of the control group were well matched (Table 2). The nerve-saving grade, pathologic T stage, and positive surgical margin rate were comparable (Table 3). The operation time was significantly longer in the hypothermic group (mean difference ± standard error, 15.4 ± 7.5 minutes). This was surely because extra time was spent to install the BelloCool system and to perform the intraoperative temperature measurements.
Comparison of Baseline Characteristics Between the Hypothermic Surgery Group and the Matched Control Group
Values are presented as median [IQR].
BMI = body mass index; DM = diabetes mellitus; EPIC-CP = Expanded Prostate Cancer Index Composite for Clinical Practice; EQ-5D-5L = five-level version of EuroQol-5 dimensions; GG = grade group; HTN = hypertension; IIEF-5 = 5-item International Index of Erectile Function; ISUP = International Society of Urological Pathologists; PSA = prostate-specific antigen; VAS = visual analog scale.
Comparison of Perioperative Characteristics Between Hypothermic Surgery Group and Matched Control Group
Values are presented as median [IQR].
WBC = white blood cell.
Comparison of functional outcomes
At every postoperative time point (1, 3, 6, and 12 months), the hypothermic group showed a superior potency recovery rate (Table 4). At the end of the follow-up (12 months), potency was recovered in 40% of patients in the hypothermic group, against 15% in the control group (p = 0.027). The hypothermic surgery group tended to acquire a higher zero-pad continence rate at all time points, but the rate differences were not statistically significant. The Kaplan–Meier curve showed that potency recovery results were superior in the hypothermic group (log-rank p < 0.01) (Fig. 2). The superior result of potency recovery in the hypothermic group was also validated through IIEF-5 scoring system (Supplementary Table S3).

Kaplan–Meier analysis of interval to potency recovery. Color images are available online.
Comparison of Functional Outcome Between the Hypothermic Surgery Group and the Matched Control Group
Comparison of changes in patient-reported erectile dysfunction and QoL
Changes in the IIEF-5, EQ-5D-5L, and EPIC-CP scores for all patients are presented in Supplementary Table S4. None of these scores at 1, 3, 6, and 12 months postoperatively were significantly different between the two groups. We proceeded to perform a subgroup analysis in patients who showed potency recovery at 1 year postoperatively. The numbers of patients in the hypothermic and control groups were eight and nine, respectively (Supplementary Table S5). Although the IIEF-5 score did not differ between the groups, the EPIC-CP total and its sexual subscale scores tended to be significantly lower in the hypothermic group, indicating a better QoL.
Discussion
Although a minimally invasive approach with a magnified surgical field to perform nerve-sparing techniques more meticulously may improve the functional outcome, we have not yet found a fundamental solution to prevent postoperative functional deterioration. We devised a sophisticated and practical instrument, with proven safety and feasibility in an animal model. 11 Our device has several advantages over the UroCool device, previously invented by Finley et al. 19 First, the rectal balloon has a curved asymmetrical elliptical shape, unlike the straight-, cylindrical-, or oval-shaped UroCool device. This enabled the optimization of the contact with the prostate surgery cooling site.
Considering that thermal energy is sometimes not localized and could be transmitted to nearby tissues where it induces injury, 10 maximal contact may be an important factor contributing to the functional outcome. Second, 30 to 40 mL of coolant must be injected into the inner UroCool balloon and 60 to 100 mL into the outer balloon. The BelloCool has circumvented this inconvenience in that it is possible to automatically adjust the coolant flow rate and pressure intraoperatively. Third, the UroCool device uses a refrigerant, which is bulky and noisy, whereas our device uses the Peltier cooling technology, which hardly generates noise.
Finally, the temperature of the pelvic region was maintained <30°C with the UroCool device, whereas with our device, the pelvic temperature was constantly maintained at ∼26°C. Since it is <28°C, neuroprotection effect may be fully optimized according to Kawamura et al. 20 Given that variation of the NVB temperature between individuals is smaller than the previous reports, 19 we could conclude that low NVB temperature is effectively achieved and stably maintained. The safety of this device was assessed by orthogonal approaches. There was no device failure, and the operation was completed without any problems. Adverse events within 90 days of surgery were reviewed. A minor complication occurred in 5 of 20 patients (25%) (Supplementary Table S1), which was comparable with that of the matched control group [n = 12/60 (20%)]. Furthermore, constantly maintained endorectal cooling did not grossly induce any bowel injury and it was also judged by a patient-reported questionnaire (Supplementary Table S2).
Compared with previous studies performed using the UroCool device, our study showed potential for more promising results. Several studies demonstrated that age and preoperative potency may be risk factors hindering good functional recovery. 19,21 The mean ages of patients were 67.8 ± 5.9, 59.9 ± 6.9, and 62.5 years in this study, the UroCool feasibility trial study, and the UroCool multicenter randomized controlled trial (RCT) study, respectively. The mean preoperative IIEF-5 score were 18.1 ± 3.8 (present study) vs 22.7 ± 2.9 (UroCool feasibility trial study) vs 19.4 (UroCool multicenter RCT study). Furthermore, considering that Asians have a tendency to show slower and lower rates of potency recovery after RARP, 22 we may expect more promising functional outcomes in future multicenter RCT.
Interestingly, although the number of patients who regained potency was similar in both studies, the EPIC-CP total and sexual subscale scores tended to be better in the hypothermic group, indicating that patients in the hypothermic group who recovered potency had significantly better QoL than control patients who had also regained potency. Furthermore, among these patients, 37.5% of hypothermic group did not need medication for intercourse, whereas 22.2% of control group did not need medication. This may also indicate that what matters is not only the preservation of the NVB, but also the quality of the preserved NVB, which may be affected by the local inflammatory response.
Since this trial with small number of patients primarily attempted to assess the safety and efficacy of BelloCool device, the functional outcomes of this study should not be interpreted as robust evidence. But rather they should be considered as a potential possibility for clinical benefit. Large-population-based RCT should be followed to confirm the improvement of functional outcome and QoL in the hypothermic group.
This study has some limitations. Because of time constraints, we could not obtain real-time temperature measurements of the surgical site during the entire surgery. Second, since one of the two surgeons had not been exposed to this medical device before this trial, his learning curve could not be considered. Third, because it is not double-blinded trial, surgeons may have had inherent bias toward more meticulous nerve sparing in the hypothermic group. And fourth, there was inter-surgeon functional outcome variability, raising the need for multicenter RCT with a greater number of surgeons to more accurately assess the clinical benefit of this device.
However, this study has several strengths. We confirmed the possibility that continence and potency recoveries might be better in the hypothermic group using BelloCool device. With the vast amount of questionnaire data, we could analyze each patient's QoL trends. Furthermore, with a rigorously matched control group obtained from a prospective cohort, we compared the clinical efficacy of hypothermic RARP using real-world data. If hypothermic RARP is combined with novel techniques such as thermal magnetic resonance virtual imaging 23,24 or intraoperative nerve monitoring and mapping, 25 we believe that we could ultimately overcome the challenge of functional outcome deterioration after surgery and widen our scope to various pelvic surgeries, such as robot-assisted simple prostatectomy. 26
Conclusion
Hypothermic RARP using an endorectal cooling balloon device (BelloCool™) is safe and feasible. NVB temperature was effectively lowered with little inter-patient variation. Functional outcomes showed the potential for clinical benefits of hypothermia compared with the matched-control group. Well-designed RCT is warranted to confirm the efficacy of this device in terms of improving post-RP urinary and sexual function.
Footnotes
Authors' Contributions
C.W.J. had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept, design, and funding obtained by C.W.J. Initial drafting of the article by J.H.H. and D.H.P. Statistical analysis by J.H.H, D.H.P., and C.W.J. Supervision by H.K., Y.J., C.K., and C.W.J. Administrative, technical, and material support, acquisition of data, analysis, and interpretation of data, and critical revision of the article for important intellectual content by all authors.
Author Disclosure Statement
This system was invented by Chang Wook Jeong, Jung Chan Lee, and Hee Chan Kim.
Funding Information
This study was supported by a sponsored contract with CEBIKA, Inc. Grant number: 0620193230.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.