
Abstract
Background:
Holmium laser enucleation of the prostate (HoLEP) has been used as an effective minimally invasive technique for management of enlarged prostates. We aimed to report the role of HoLEP in prostate cancer (PCa) patients either on active surveillance with bothersome lower urinary tract symptoms (LUTS) or for prostate debulking before radiation therapy and the impact on PCa management plans.
Methods:
Prospectively maintained database in two institutions was reviewed for patients with localized PCa managed by HoLEP with at least a follow-up of 1 year. We assessed prostate-specific antigen (PSA) trends, effect on international prostate symptom score (IPSS) and further management of PCa.
Results:
Out of >2000 HoLEP patients, 117 patients with a median follow-up of 30 months were included. Mean (standard deviation) age was 72.3 (±8.3) years with median (interquartile range, IQR) IPPS of 22 (16–28) and median (IQR) PSA at 7.6 (5.3–14.9) ng/mL. Gleason grade group was 1, 2, 3, and 4 in 47 (73.2%), 32 (27.35%), 7 (5.9%), and 4 (3.4%) patients, respectively. Median (IQR) PSA has significantly dropped to 1.3 (0.6–3.1), 1.4 (0.75–2.9), and 1.7 (0.86–2.75) ng/mL at 6-week, 3-month, and 1-year follow-up, respectively (p < 0.001). IPSS scores post-HoLEP obviously improved with mean (IQR) IPSS of 10 (5–13), 7 (3–12), and 3 (2–5) at 6-week, 3-month, and 1-year, respectively (p < 0.001). Eighty-eight (72%) patients stayed on active surveillance, whereas 27 (23%) patients had radiotherapy ± androgen deprivation therapy for persistently high or relapsing PSA. Within 36 intermediate-risk patients, 15 (41.6%) and patients had radiotherapy, whereas 21 (58.3%) patients continued active surveillance.
Conclusions:
HoLEP is beneficial in debulking large prostate in PCa patients with bothersome LUTS on active surveillance or before radiotherapy. HoLEP reduces the contribution of large adenoma to PSA level, thus reflecting PSA level better and helping reduce overtreatment.
Introduction
Holmium laser enucleation of the prostate (HoLEP) has been increasingly used as an effective minimally invasive surgical option for managing benign prostatic hyperplasia (BPH). HoLEP has the advantages of durable symptom relief, low overall complication rate, and very low reoperation rate compared with the traditional resection technique regardless of the prostate volume. 1 –4
Prostate cancer (PCa) is the second most common cancer and the fifth leading cause of cancer-related death among men worldwide. With the widespread screening and early detection for PCa, localized PCa was diagnosed in a significant percentage of patients with a growing role for active surveillance for very low and low-risk PCa. 5 –7
About 34% and 6% of patients on active surveillance for PCa can suffer moderate and severe lower urinary tract symptoms (LUTS), respectively, because of associated large benign prostate adenoma. 8 Even more, radiotherapy for localized PCa is usually associated with a surge in LUTS that persists for 3 to 6 months, especially in patients with pre-existing significant LUTS symptom scores before radiotherapy. 9,10
Few studies have evaluated the role of debulking the prostate volume in patients with PCa on active surveillance, specifically through transurethral resection of the prostate (TURP). 11 –13 In this study, we aimed to study the role of HoLEP in PCa patients either on active surveillance with bothersome LUTS or for prostate debulking before radiation therapy and the effect of prostate-specific antigen (PSA) drop post-HoLEP on further PCa management plans.
Materials and Methods
A prospectively maintained database of two separate institutions (Baylor Scott and White Health and Indiana University) was retrospectively reviewed for patients with localized PCa managed by HoLEP with at least a follow-up of 1-year post HoLEP.
Data regarding the baseline patients' demographics, PCa characteristics, the PSA trends before and within follow-up after HoLEP, effect on international prostate symptom score (IPSS) and quality of life (QOL), the impact of HoLEP on further management of PCa, and any associated complications were collected and analyzed.
Statistics
All statistical analysis was performed using the commercially available SAS (Statistical Analysis Software) version 9.4 (SAS Institute Inc., Cary, NC). For descriptive statistics, continuous variables were presented as mean (standard deviation) or median (interquartile range, IQR) according to normality, whereas categorical variables were given as absolute numbers and percentages. Wilcoxon Rank Sum tests were used for univariate analysis of quantitative variables that did not appear to attain normality. The significance level was set at a p-value <0.05.
Results
Out of >2000 patients in the HoLEP database in both institutions, the study included 117 patients with pre-existing PCa who had HoLEP between September 2009 and August 2020. The patients' mean age was 72.3 (±8.3) years. Lower urinary symptoms score was severe in 73 (62%) patients with a median (IQR) IPPS score of 22 (16–28). One hundred six (90.5%) patients had pre-HoLEP either Gleason grade group 1 or 2. Table 1 shows patients' baseline data before HoLEP.
Baseline Patients' Characteristics
ASA = American Society of Anesthesiology; BMI = body mass index; CIC = clean intermittent catheterization; IPSS = international prostate symptom score; IQR = interquartile range; PSA = prostate-specific antigen; QOL = quality of life; SD = standard deviation
The median (IQR) operative time was 64 (42–82) minutes, whereas the weight of the resected adenoma was 67 (±41) gm. More than 90% of the patients had <24 hours hospital stay or same-day discharge. Blood transfusion and readmission were required in only 2 (1.7%) and 3 (2.5%) patients, respectively. Histopathology analysis of the HoLEP specimens showed PCa in 49 (41.9%) patients (Table 2). Median (IQR) serum PSA has significantly dropped from baseline 7.6 (5.3–14.9) before HoLEP to 1.3 (0.6–3.1), 1.4 (0.75–2.9), and 1.7 (0.86–2.75) at 6-week, 3-month, and 1-year follow-up encounters (p < 0.001) (Fig. 1). Follow-up data showed obvious improvement of IPSS scores and QOL post-HoLEP with mean (IQR) IPSS score of 10 (5–13), 7 (3–12), and 3 (2–5) at 6-week, 3-month, and 1-year follow-up, respectively (p < 0.001) (Table 3).
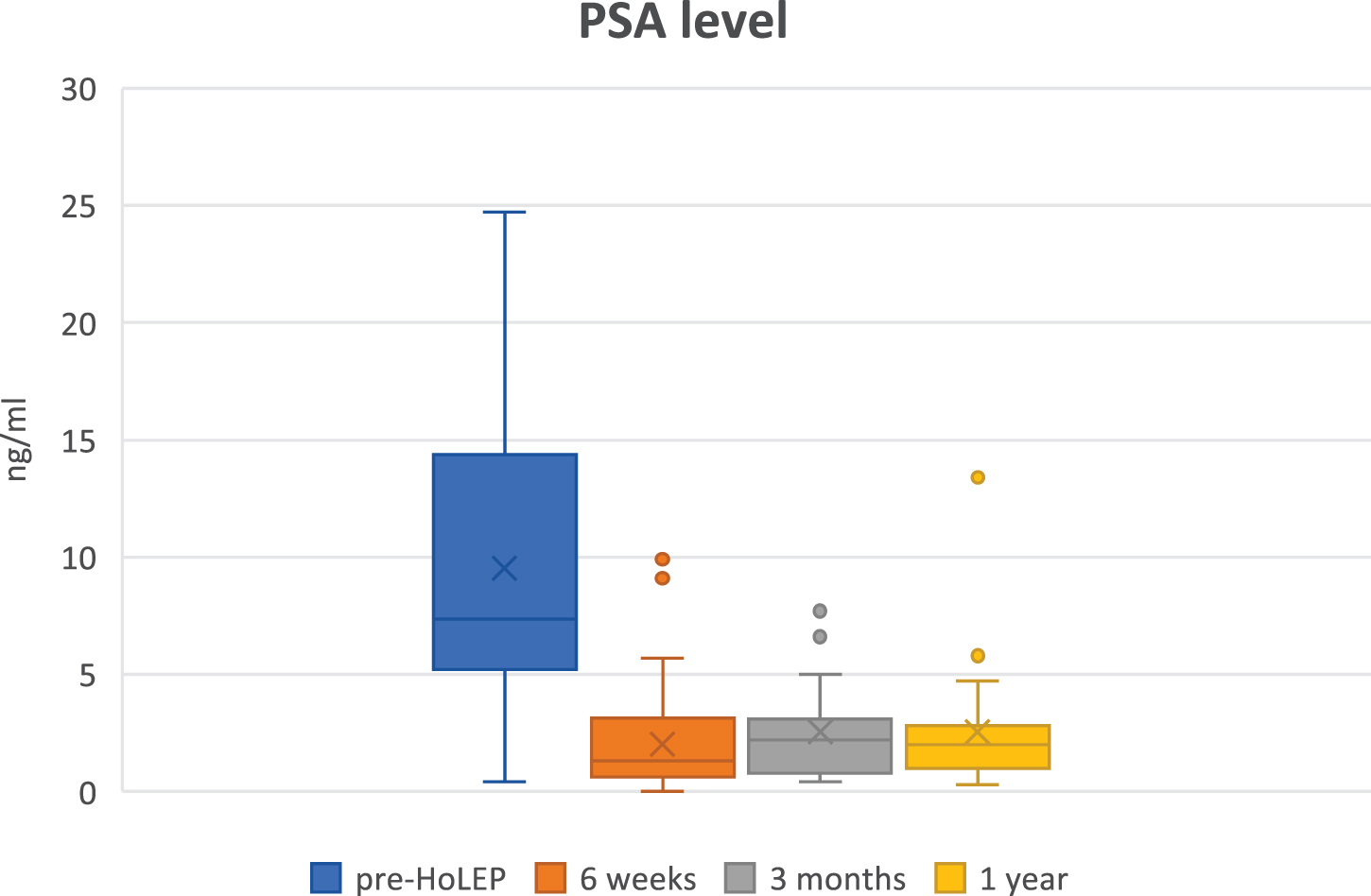
Comparison of PSA level at baseline and at 6-week, 3-month, and 1-year follow-up occasions. HoLEP = holmium laser enucleation of the prostate; PSA = prostate-specific antigen. Color images are available online.
Perioperative Outcome Data
BPH = benign prostatic hyperplasia; PCa = prostate cancer.
Postoperative Follow-Up Data
HoLEP = holmium laser enucleation of the prostate.
Stress incontinence was observed in 40 (34%), 12 (10%), and 1 (0.85%) patients, whereas urge incontinence was seen in 16 (13.6%), 4 (3.4%), and 3 (2.56%) patients at 6 weeks, 3 months, and 1-year post-HoLEP, respectively. One (0.85%) patient had a bulbar urethral stricture, whereas another patient (0.85%) was complicated by bladder neck contracture.
Median follow-up duration post-HoLEP was 30 months. Eighty-eight (72%) patients continued active surveillance, whereas 27 (23%) patients had radiotherapy ± androgen deprivation therapy (ADT) for PSA relapse or persistently high PSA after HoLEP. Only 2 (1.7%) patients had high-intensity focused ultrasound (HIFU). Three patients from the active surveillance group died from causes other than PCa.
Specific analysis of 36 (30.7%) patients with intermediate-risk PCa showed that their median (IQR) preoperative PSA was 9.05 (5.45–14) ng/mL, whereas 6 weeks, 3 months, and 1-year median (IQR) PSA were 1.5 (0.7–3.3), 1.5 (0.7–2.7), and 1.65 (0.9–2.45), respectively. With mean follow-up of 19 months post-HoLEP, 21 (58.3%) patients continued active surveillance, whereas 15 (41.6%) patients had radiotherapy ± ADT.
Discussion
With the wide spread of screening for PCa and early PCa diagnosed in large percentage of patients, there is always a concern with overtreatment. Both benign adenoma and PCa can share in high serum PSA levels. High PSA levels caused by associated BPH in PCa patients can change the patients' risk categorization and may lead to overtreatment with radical prostatectomy or radiotherapy instead of continuing active surveillance.
As shown in our results, HoLEP eliminates the contribution of large volume adenoma in PSA level and was associated with a significant drop of PSA post-HoLEP. Some of the intermediate-risk category patients with favorable pathology report (Gleason GG2) were planned to go for radiotherapy after HoLEP debulking; however, their PSA level markedly dropped post-HoLEP and were chosen to continue with active surveillance.
Wu and colleagues in their large TURP series in patients with prediagnosed PCa have reported that greater PSA reduction (>68%) after TURP, post-TURP PSA <4 ng/mL, low Gleason score at diagnosis, and <5% tumor involvement in TURP specimens were associated with better progression-free survival (PFS). Moreover, they have shown that prostate-directed local therapy significantly improved PFS in intermediate- and high-risk groups but not in the low-risk group. In the intermediate-risk group, local therapy improved PFS only for patients with post-TURP PSA >4 ng/mL or <68% PSA reduction after TURP. 12
Hagmann and colleagues have reported their long-term follow-up of patients managed by TURP with active surveillance for PCa. They reported that half of active surveillance patients will encounter disease progression and eventually require definitive management; however, half of the patients benefit from delaying active treatment and are spared the adverse side effects. 13
HoLEP was reported to be associated with lower nadir postoperative PSA level in patients with BPH compared with most series of TURP and simple prostatectomy. Mean serum PSA at 3 months post-HoLEP is reported at 0.6 ± 0.6 ng/mL. 14 Elmansy and colleagues have studied the PSA velocity within 2 years of follow-up after HoLEP in >300 patients with BPH. They showed that PSA dropped post-HoLEP to the mean of 0.91 ng/mL. Also, they have reported that higher baseline PSA, lower PSA reduction, and higher PSA velocity after HoLEP were linked to a higher risk of PCa diagnosed later on during follow-up. 15 Similar data were recently reported by Lambert et al. They reported that the first postoperative PSA was an independent predictor of PCa diagnosis after HoLEP with an optimal cutoff value of 1.73 ng/mL. 16
HoLEP has been repeatedly reported to be associated with higher rate of incidental PCa detection in patients having surgery for BPH compared with TURP. It is reported that 5.6% to 23.3% of patients with HoLEP are diagnosed with incidental PCa. Data report favorable functional and oncologic outcomes of incidental PCa post-HoLEP with wide range of oncologic treatment. 17 –19
There is little literature on the use of HoLEP in patients with previously diagnosed PCa. Rivera and colleagues first reported the use of HoLEP in 11 patients with localized PCa with a Gleason score range of 6 to 9. They concluded the safety of HoLEP in the treatment of LUTS in selectively chosen patients. 20 Recently, Schober and colleagues have reported HoLEP use for management of refractory LUTS in a small cohort of 20 patients on active surveillance for PCa. Their results showed drop of median PSA from 8.5 ng/mL before HoLEP to 1.4 ng/mL at median follow-up of 18.5 months. 21
In contrast, patients managed by radiotherapy for localized PCa with large volume prostate usually suffer from significant LUTS and possible urine retention especially with pre-existing high symptoms scores. 9,10 Horiuchi and colleagues have reported using HoLEP for debulking huge prostate adenoma before HIFU in 10 patients with localized PCa. In their study, HoLEP before HIFU was found to be associated with a lower symptom score and lower catheterization rate compared with treatment with HIFU alone. 22
Technically, The HoLEP surgical technique and follow-up were similar to the usual conducted in patients with BPH. The authors did not face different technical challenges or difficulties with HoLEP in the patients with PCa.
This study shows that HoLEP is safe and effective in debulking prostate for improving the LUTS symptom score in PCa patients either to continue active surveillance or before local treatment with radiotherapy or HIFU to avoid severe exacerbation of LUTS.
The limitation of this study is its retrospective nature. Prospective randomized studies to validate the beneficial effect of HoLEP debulking before radiotherapy in the setting of large prostate size are further required.
Conclusions
HoLEP is beneficial in debulking large prostate in PCa patients with bothersome LUTS on active surveillance or before radiotherapy. Moreover, HoLEP reduces the contribution of large volume adenoma to PSA level in PCa patients, thus reflecting PSA level better and reducing overtreatment, especially in intermediate-risk category patients.
Footnotes
Authors' Contributions
Conceptualization by K.W. and M.M.E. Design, methodology, and analysis/interpretation by M.E. and A.S. Data collection and processing by M.E., A.S., A.P., and S.J. Literature review and writing by M.E. Supervision by J.L., K.W., S.J., and M.M.E. Critical review and editing by J.L., S.J., and M.M.E.
Informed Consent
Informed consent was waived by the Institutional Review Board (No. 019-195).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The author, Mohamed Elsaqa, is funded by a scholarship grant from the Ministry of Higher Education of the Arab Republic of Egypt.