
Abstract
Objective:
The da Vinci single-port (SP) platform represents the latest innovation in minimally invasive urologic surgery, and the adoption of this technology by urologists is increasing. In this article, we briefly describe the evolution of minimally invasive and single-site surgery, and offer a comprehensive review of the current literature on the SP platform.
Materials and Methods:
For relevant articles, three electronic databases, including PubMed, Scopus, and Web of Science, were searched from their inception until August 15, 2022. The published literature to date within SP robotic surgery in urology will be discussed.
Evidence Synthesis:
There are relatively few high-quality studies on the SP system, but there are multiple case series describing unique indications and surgical approaches with the SP robot, demonstrating safety and feasibility in the hands of experienced robotic surgeons. There also are an increasing number of prospective, larger cohort studies comparing outcomes between SP and multiport (MP) approaches that show benefits of the SP system regarding improved cosmesis, postoperative pain control, and decreased length of stay.
Conclusions:
Multiple prospective studies have shown benefits regarding cost and pain control for SP platform procedures compared to the traditional MP robotic approach. While its high cost and learning curve represent barriers to adoption, the SP platform represents a critical development in minimally invasive surgery. As this technology is further implemented at more institutions, long-term, high-quality data should accrue that will demonstrate its true value.
Introduction
History
One of the distinguishing features of urology over the past 40 years has been a willingness of urologists to adopt new surgical techniques and technologies that improve patient care and establish strong foundations for further innovation. This spirit of innovation has perhaps been best demonstrated in the field of endourology, with its emphasis on developing minimally invasive surgical approaches to improve efficiency and patient outcomes. For example, ureteroscopy, percutaneous nephrolithotomy, and laparoscopic surgery—procedures initially with limited indications and reserved for the highest volume surgeons—have progressed to the point where these techniques are now standard in the treatment of a wide range of benign and malignant disease. 1 The advances in these minimally invasive approaches have largely been due to rapid improvements in the respective technologies; improvements in access and visualization and more versatile instrumentation have been essential for the widespread adoption of these techniques, with particular application to laparoscopy and its historically steep learning curve. 2
There is no better example of the realization of these advancements than the development and adoption over the past two decades of the da Vinci robotic surgical platform (Intuitive Surgical, Inc., Sunnyvale CA). Since its initial FDA approval in 2000, the da Vinci surgical system has revolutionized the treatment of numerous urologic conditions by enhancing the advantages—and minimizing the disadvantages—of traditional laparoscopic surgery for the surgeon by providing wristed articulating instrumentation, high-definition and three-dimensional visualization, and improved surgeon ergonomics.
In this article, we will provide a brief history of single-site surgery and its most recent iteration using the da Vinci single-port (SP) robotic system, review the literature with regard to the applications of the SP in urologic surgery, and investigate future directions and emerging technologies for the continued evolution of SP robotic surgery.
Laparoendoscopic single site surgery
As traditional laparoscopic surgery became standard for the treatment of many urologic pathologies, minimally invasive surgical techniques continued to be developed. The next step in the evolution of minimally invasive surgery involved attempts at utilizing a single working site in the abdomen, through which entire procedures would be performed. In 2009, Gill and colleagues drafted a consensus statement on the relatively nascent techniques of laparoendoscopic single site (LESS) surgery, stating that “technological advances in instrument design have fueled newer clinical applications, the success of which in turn has necessitated the development of yet newer technology. This self-perpetuating cycle now stands at the threshold of a quantum leap forward.” 3 Although that statement would prove to be prescient, early experiences with single site laparoscopic surgery and its subset, natural orifice transluminal endoscopic surgery (NOTES), showed that despite its technical feasibility, these approaches needed dramatic improvements in instrumentation for widespread adoption. 4
The da Vinci Si and Xi systems offered many of the technologic improvements necessary for LESS to become more practical and clinically useful. Improved ergonomics, 3D visualization, and instrument articulation with reduced clashing were major advantages that robotic LESS (R-LESS) offered compared to LESS. R-LESS was first described by Kaouk et al. in 2008 with a series of three patients using the da Vinci S system. 4 Subsequent larger series were reported for various urologic procedures, showing that although R-LESS proved more robust than LESS, it still had significant limitations because its design was not intended for single-site surgery. 5
Advantages and disadvantages of SP robotic surgery
Single-site surgery has distinct advantages over open and multiport (MP) surgery. While there are relatively few studies with small cohorts that evaluate outcomes in LESS, the few studies that have been done indicate that LESS is associated with improved cosmesis, reduced postoperative pain, and lower analgesic requirements. 2 However, while these same analyses show that there is no difference in complication rates, LESS is associated with longer operative times and higher rates of conversion to traditional laparoscopy and overall R-LESS has been shown to have similar outcomes when compared to the MP robotic approach. 6
Only a few studies have compared the SP and MP approach directly, mostly single institution with relatively small cohorts. Lenfant and colleagues recently published their data from the Cleveland Clinic comparing the SP and MP with regard to cost and perioperative outcomes. They found that for a prostatectomy, there was no significant overall cost difference between the two platforms. The SP group had higher operating room (OR) disposable costs but this was offset by the lower hospital costs due to significantly shorter lengths of stay. 7 In another study by the same group, using prospectively collected data comparing SP vs MP, they found that patients who underwent extraperitoneal radical prostatectomy with the SP robot had significantly shorter hospital stays, lower post-op opioid use, and similar perioperative outcomes compared to a transperitoneal MP approach. 8 Another single institution retrospective study published by Vigneswaran and colleagues in 2020 found similar results. 9
There are also unique challenges that accompany adoption of the SP system. Similar to LESS, the learning curve can be significant for various reasons. Because all four arms of the robot pass through a single 2.5 cm trocar, there is limited working space and decrease range of motion. The SP system attempts to improve this through the use of articulating “elbows” that spread out in the working space, but there can be significant instrument clashing that surgeons may experience especially early in the learning curve. 10 The elbow and camera articulation requires that instruments extend farther out the cannula, which means that there is often a greater working distance from the tissue compared to the MP system.
One of the most notable differences of the SP system is the reduced grip strength of the instruments, which often requires changes in technique to appropriately retract and dissect tissue and may limit the use of robotic bulldog clamps. In addition, the SP system does not currently allow for the use of Firefly fluorescence imaging. While many of these challenges can be overcome by high-volume surgeons, future generations of the SP system will need to address these issues to allow for more widespread adoption. 11,12
SP Platform Specifications
The da Vinci SP
In 2018, the da Vinci SP system received FDA approval for widespread use in clinical practice. This device represents the fourth-generation robotic platform, behind the S, Si, and Xi robots. 13 Similar to previous generations, the surgeon has the ability control a camera and three instruments at any time. With the SP system, however, these instruments are contained within a single 2.5 cm diameter cannula, and are arranged at the 12, 3, 6, and 9 o'clock positions within the cannula. The instruments are 6 mm in size and the endoscope is 8 mm. Both the instruments and the endoscope articulate at an “elbow” and “endowrist,” allowing for increased working space within the body.
The surgeon is able to control each instrument separately as with previous generations, but now has the added ability of full camera angulation up to 30°, as well as the ability to move all instruments together at one time using added functionality of the foot pedal. Due to the narrower field of view and closer proximity of the instruments to one another, one of the unique challenges of the SP system is localization of the instruments relative to one another. To help the surgeon locate each instrument, there is a new navigator icon on the surgeon's screen that shows each instrument's location relative to the others and its maximal range of motion. 13
Upper Urinary Tract Surgery
In the last decade, LESS has been utilized for a variety of upper tract urologic procedures, including radical nephrectomy (RN), partial nephrectomy (PN), pyeloplasty, donor nephrectomy, and renal cyst decortication among others. 14 While the techniques used in LESS were similar to conventional laparoscopy, difficulties arose due to limited triangulation, a restricted working space and clashing of instruments which has limited the widespread adoption of these techniques. Multiple studies demonstrate that LESS compared to conventional laparoscopy have similar operative times, estimated blood loss (EBL), hospital stays, and complication rates, although with a slightly higher rate of conversion of 21% (15.8% reduced-port laparoscopy, 4% conventional laparoscopy/robotic surgery, and 1% to open surgery). 14,15 Therefore, the main benefits of LESS are reduced pain, decreased analgesic requirements, and more favorable cosmesis. 15
With the advent of robotic surgery and the many benefits associated with use of the robotic platform, there has been a renewed interest in SP R-LESS. Kaouk et al. performed the first series of SP robotic surgeries in 2008 using a custom designed R-Port through a 2 cm umbilical incision. 16 Since then, there have been further advances such as Intuitive Surgical Da-Vinci® Si, which enabled the use of curved instruments via the VeSPA system with 4 degrees of freedom (DOF), and the Da-Vinci Xi, which allowed the use of SP999 and SP1098-platform with 7-DOF-instruments. 17 The recent FDA-approved purpose-designed Da-Vinci SP Platform (Intuitive Surgical, Sunnyvale, CA) is a further refinement of SP technology and supports a single multichannel laparoscopic trocar that allows the use of snake like articulating arms with EndoWrist® technology and an articulating endoscopic camera (Fig. 1).
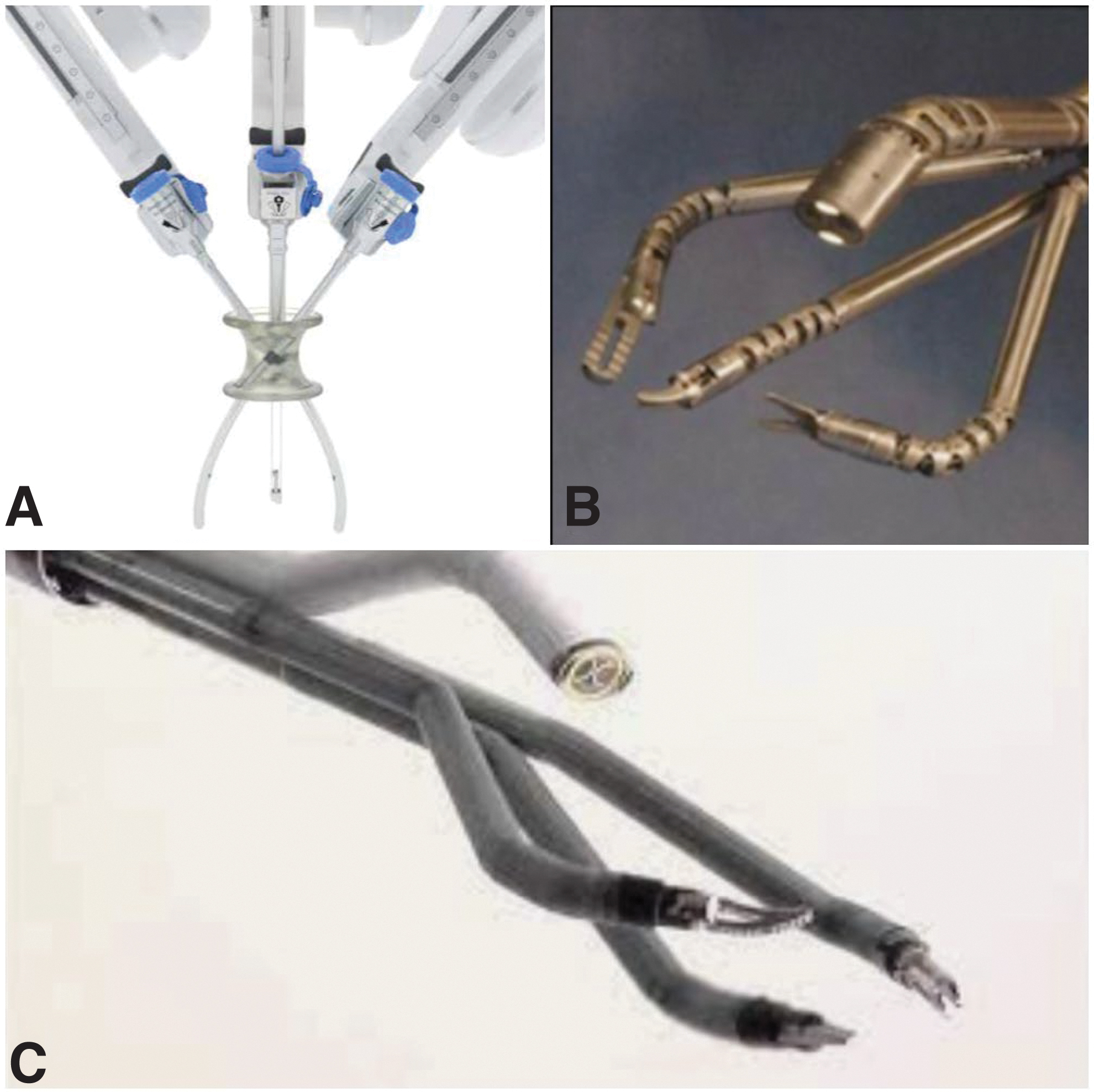
Various iterations of Da-Vinci® Single-Port Robotic Systems.
The main improvement in this system was the ability of the robot to pivot around a fixed-point allowing instruments to be deployed independently. Initial cadaver studies, with the third-generation system performing PN revealed satisfactory resection, operative times, and no complications (defined as injury to an organ or vessel). 18 The Da-Vinci SP platform is currently the most common SP system in use across the United States.
Radical nephrectomy
The first R-LESS RN was performed by Kaouk et al. in 2008. 16 Since then, there have been few studies directly comparing R-LESS RN to MP RN as most studies focused on PN being the more technically challenging procedure. Recently, the utility of even MP robotic surgery for RN compared to conventional laparoscopy has been called into question. 19 Early comparative studies evaluating R-LESS RN vs conventional laparoscopy were performed using the Da-Vinci Si system and a SILS port (Coviden, Mansfield, MA) or GelPort™ (Applied Medical, Rancho Santa Margarita, CA). 20 The authors noted no differences in operative time, EBL, or complication rate, however, patients in the R-LESS group had fewer narcotic requirements and shorter hospital stay (2.5 days vs 3 days) compared to the laparoscopy group.
A 2011 multi-institutional review of R-LESS-based urologic cases, including 210 RN revealed similar operative times, EBL, hospital stays, and complication rates; however, there was an increased conversion rate of 20.8%. The mean operative time for R-LESS RN was 158 minutes with a mean EBL of 168 mL. In another series of six RN performed with R-LESS, the authors noted no intraoperative or postoperative complications, a median operative time of 179 minutes and mean EBL of 100 mL. 21 Overall, SP robotic RN appears to be a safe and feasible option providing outcomes similar to conventional laparoscopy and MP robotic surgery.
Partial nephrectomy
A nephron sparing approach has become the preferred treatment option for most renal masses given the effective preservation of renal function and avoidance of the morbidity associated with chronic kidney disease such as increased cardiovascular risk and the need for dialysis. 22 Major developments in minimally invasive surgery have demonstrated equivalent oncologic outcomes and overall survival compared to conventional open surgery. 22 As such, there is increased interest in the use of laparoscopy and robotic surgery for PN. Concurrently, there has been an increased adoption of R-LESS for PN due to improved cosmetic outcomes, decreased analgesic requirements, and shorter hospital stays. 23 Several institutional and multi-institutional reviews have been published in the literature comparing R-LESS to MP robotic PN (Table 1).
Perioperative Outcomes of Robot-Assisted Partial Nephrectomy Performed Using the Single-Port vs Multiport Robotic System
BMI = body mass index; EBL = estimated blood loss; MP = multiport; NA = not available; PSM = positive surgical margin; SP = single-port.
In earlier years, conventional R-LESS had low adoption rates for PN due to the steep learning curve and technical limitations of the instruments such as reverse handedness, clashing of instruments and in-line optics which hampered triangulation. Second generation R-LESS technology overcame some of these limitations using articulating instruments, however, these too were hampered by the robotic instruments being fixed at the level of the fascia. Studies using earlier iterations of SP technology demonstrated that R-LESS for PN were similar in technique and outcomes compared to MP surgery. 24 In 2013, Komninos and colleagues published the largest contemporary series comparing R-LESS to conventional MP robotic PN. 25 The primary outcome, a trifecta of warm ischemia time ≤20 minutes, negative margins, and no surgical complications, was achieved in only 25.6% patients in the R-LESS group compared to 42.7% in the MP group.
Similarly, patients in the R-LESS group had a significantly longer mean operative time, warm ischemia time, and increased estimated glomerular filtration rate (eGFR) percentage change. No differences were noted with regard to hospital stay, EBL, postoperative eGFR, positive margins, and surgical complications. Similarly, another study in 2014 demonstrated comparable outcomes between both approaches with patients who underwent R-LESS having significantly lower postoperative pain. 6 More recent studies have shown further benefits of the SP Platform compared to MP surgery for PN. In 2022, Harrison et al. demonstrated in a propensity score-matched comparison decreased opioid use and decreased cumulative hospital stay in the SP group compared to a MP cohort. No differences were seen with regard to operative time, blood loss, ischemia time, or positive margins. 26
Similarly, in a study comparing perioperative outcomes in patients undergoing SP vs MP PN, Glaser and colleagues demonstrated similar operative times, conversion rates, hospital stay, and opioid requirements for both groups. Of note, the SP group were more likely to undergo a retroperitoneal approach as opposed to a transperitoneal approach (81% vs 19%, respectively). 27 Overall, SP continues to gain momentum as a viable option for PN especially within the confined space of the retroperitoneal approach and results in reduced pain and better cosmesis while overcoming the morbidity associated with MP surgery.
Pyeloplasty
Open pyeloplasty has long been considered the gold standard treatment for ureteropelvic junction obstruction with success rates approaching 90% to 100%. 28 However, due to the morbidity associated with open surgery, minimally invasive approaches were developed such as endoscopic balloon dilation and laser endopyelotomy. Unfortunately, these techniques have had poor long-term success rates of only ∼60% to 80%. 28 With increasing adoption of laparoscopy and robotic surgery most pyeloplasties are now performed in a minimally invasive manner. Since most pyeloplasties are performed in a pediatric population, newer technologies such as SP surgery are gaining traction to provide better cosmesis. 29
Current literature on SP robotic pyeloplasty remains scant with only a few case series and reports published to date. Lenfant et al. in 2020 published their first experience with 10 patients undergoing Da-Vinci SP robotic pyeloplasty. 29 All patients were placed in a modified flank position and a single 3 cm incision used for port entry. Incisions were initially umbilical but later converted to a mini-Pfannenstiel for improved cosmesis. The pyeloplasty was performed in a classic Anderson-Hynes dismembered manner for all cases. The authors reported no intraoperative complications, a mean operative time of 166 minutes, and median blood loss of 20 mL. Two patients with mini-Pfannenstiel incisions were discharged home the same day. Similarly, a case report in a pediatric patient demonstrated that SP robotic pyeloplasty is feasible and safe, noting that docking time was slightly longer than usual compared to MP surgery. 30
Parikh and colleagues in 2021 reported their experience with SP robotic pyeloplasty in a 10-year-old patient noting no difficulties or intraoperative complications. 31 They concluded that patient selection was paramount to success and suggested slightly older patients where the working distance of the articulating instruments can be kept at a minimum distance of 10 cm to optimize space and prevent clashing of instruments. In 2021, Harrison et al. reported the largest contemporary comparison of SP vs MP robotic pyeloplasty. 32 Twenty-one patients undergoing SP Platform pyeloplasty were propensity matched to 21 patients undergoing MP pyeloplasty. The SP group was associated with longer operative times (128 minutes vs 88 minutes) and a shorter follow-up time (9.3 months vs 18.7 months). There were no differences in perioperative or postoperative outcomes.
Another recent study demonstrated that patients undergoing SP robotic pyeloplasty had decreased length of hospital stay (11.4 hours vs 42.6 hours), lower opioid use and lower rate of opioid prescription on discharge. 33 Overall, SP robotic pyeloplasty is a feasible and safe procedure providing similar outcomes to MP surgery with improved cosmesis and decreased analgesic requirements.
Donor nephrectomy and renal transplant
MP robot-assisted kidney transplantation (RAKT) has emerged as a viable and potentially less morbid approach compared to open surgery. 34 The interest in a minimally invasive approach to renal transplantation was due to the desire to decrease the risk of wound-related complications, such as dehiscence, infection, and hernia, that are associated with open kidney transplantation. 35,36 A recent systematic review comparing open vs minimally invasive kidney transplant, including robotic approaches, has demonstrated lower surgical site infections (0%–8%) and less wound complications such as incisional hernias (0%–6%) with quicker postoperative recovery and improved cosmesis with the minimally invasive approach. 37 With the advent of SP robotic systems, there has been renewed interest in RAKT. In 2021, Kaouk et al. described their initial experience with SP robot-assisted kidney transplant and autotransplantation. 38 Six deceased donor transplants and three autotransplants were performed using the SP robotic system with either a transperitoneal or extraperitoneal approach.
All procedures were performed in a supine position with the bed tilted 30 laterally and using a midline periumbilical incision with Gelpoint™ system. The Gelpoint was used to introduce the allograft. Total operative and vascular anastomosis times for SP RAKT ranged from 300 to 400 and 52 to 92 minutes, respectively. For autotransplantation, total operative and vascular anastomosis times ranged from 510 to 600 and 65 to 83 minutes, respectively. None of the cases required conversion to open and all patients did well postoperatively with good allograft function after 1 year of follow-up. Similarly, Kaviani et al. described their experience with extraperitoneal SP RAKT in 12 patients with end-stage renal disease. 39 They showed excellent outcomes, including good graft function with mean follow-up of 6.3 months, no complications and median renal vein/artery anastomosis times of 26 and 37 minutes, respectively.
In addition to renal transplantation, SP robotic surgery has also been effectively used for donor nephrectomy. Garden et al. in 2021, described their first experience with seven robot-assisted donor nephrectomies (RADN) using the Da-Vinci SP system with mean operative time of 218 minutes, warm ischemia time of 5 minutes, and extraction time of ∼3 minutes 37 seconds. All patients did well postoperatively with no major complications. 40 Overall, SP RAKT and RADN appear to be safe and effective procedures, with the potential to reduce overall morbidity and enhance recovery.
Lower Urinary Tract Surgery
Radical prostatectomy
Several centers have reported their experience with SP robot-assisted radical prostatectomy using the SP platform (SP-RARP). 8,9,41 –43 Published studies have demonstrated that the SP robotic technique represents a safe and feasible approach to perform radical prostatectomy. 17,44 –46 Compared to the widely accepted MP robot-assisted radical prostatectomy (MP-RARP), these studies demonstrated that the SP approach has comparable perioperative outcomes, including operation time, EBL, and postoperative complications. 17,44 –46 Regarding postoperative outcomes, SP-RARP was associated with a significant reduction in postoperative pain, postoperative morphine usage, length of hospital stay, and indwelling urinary catheter duration. 17,44 –46 Studies comparing perioperative outcomes between SP-RARP and MP-RARP are shown in Table 2. 8,9,42,45 –48
Perioperative Outcomes of Robot-Assisted Laparoscopic Radical Prostatectomies Performed Using the Single-Port vs Multiport Robotic System
LOS = length of stay.
These relative improvements in surgical outcomes appear to be responsible for the greater likelihood of SP-RARP being performed as an outpatient procedure than MP platform. 8,9 This higher rate of outpatient surgery in the SP-RARP group could have caused by reducing opioid requirements following a reduction in postoperative pain in this patient group. 8,49 Therefore, the patients can be discharged earlier with a potential reduction in the side effects of opioids, such as nausea and vomiting, hypotension, constipation, and opioid dependence. 49 Shorter length of hospitalization has also been associated with other benefits such as decreased nosocomial infection rates and reduced hospitalization cost. 7
SP-RARP has been reported to have better surgical scar cosmesis, and therefore, a lesser perceived psychosocial impact on patients. 42 This is important as it may affect the patient's decision for proceeding with surgery. 42 However, most studies that demonstrated a preference for single-site robotic surgery predominantly studied in younger patients undergoing reconstructive surgery for benign diseases. 23,44 The impact of cosmetic advantages on older oncologic patient population is not clear but may not be negligible. 23
The SP-RARP technique is currently not as widely utilized as MP-RARP due to concerns regarding the learning curve, technical difficulties, and cost-effectiveness of acquiring an additional robotic platform. 44 Presently, most of the available evidence base for SP RARP has been reported by high volume centers and by experienced MP RARP surgeons. Hence, the results from these studies may not be able to be extrapolated to novice SP-RARP surgeons. Furthermore, the limitation of current published studies was the short-term follow-up period; thus, these studies have not yet reported long-term oncologic and functional outcomes such as biochemical recurrence, urinary continence, and sexual function recovery. Therefore, further well-designed studies and clinical trials are needed to determine the role of SP-RARP regarding long-term oncologic and functional outcomes. 8,9,41 –43,50
SP robotic radical prostatectomy technique
The da Vinci SP system has expanded the options for RARP, with transperitoneal and extraperitoneal approaches being the most commonly used. The transperitoneal approach is currently the preferred method for multiarm robot-assisted radical prostatectomy and was the first to be performed using the SP platform. In 2019, Kaouk et al. reported promising results and potential benefits of the extraperitoneal SP RARP, which included a small single incision, no additional ports, no Trendelenburg positioning, minimal postoperative pain, decreased use of opioids, and same-day discharge. 51 In 2021, Kaouk et al. demonstrated the feasibility of SP robotic transvesical radical prostatectomy using a dedicated SP robotic platform in 20 cases. 52
At our center, we have adapted our technique for performing transperitoneal MP-RARP with a nerve-sparing approach to the SP platform as follows. The patient is in steep Trendelenburg position. Restraint straps are used to prevent patient sliding. A Veress needle is used to insufflate the abdomen. A 12 mm port was placed just above the umbilicus in the midline, initially with a dilating laparoscopic port, which is then exchanged to a 25 mm SP port via the GelPOINT access platform (Applied Medical). Laterally, a 12 mm AirSeal (SurgiQuest, Inc., Milfort, CT) port is placed 10 cm away from the SP port on the left side as a +1 for the assistant. The robot is docked as shown in Figure 2.

SP robotic system docked aside with the patient in Trendelenburg and the assistant in the left side. SP = single-port. Color image is available online.
We place our camera at the 12 o'clock position, the cautery scissors at 9, the bipolar at 3, and the cadiere at 6. As our approach is transperitoneal, the bladder is dropped to develop the space of Retzius. The superficial dorsal venous complex is divided with bipolar cautery. We leave the endopelvic fascia intact and delay placing a dorsal venous complex (DVC) stitch for prostates smaller than 60 cc. Our preference for the bladder neck dissection is to approach from lateral to medial to drop the bladder away from the prostate. After division of the bladder neck, seminal vesicles and vas deferens are individually dissected (Fig. 3).

Seminal vesicles and vas deferens are individually dissected. Color images are found online.
The vasa are elevated with the Cadiere forceps to lift the prostate outward from the pelvis. The Denonvilliers' fascia is opened sharply, and the perirectal fat is visualized before finding a plane onto the posterior surface of the prostate. The prostatic pedicles in prostate may be divided with clips or spot cautery. A combination of sweeping and spot cautery helps to dissect the neurovascular bundle away from the prostate and to maintain the thicker anterolateral layer of tissue that supports the prostate and urethra on both sides. Once the anterior planes approach the apex, they are joined at a level proximal to the urethra. The preserved structure around the prostate apex has the appearance of a “hood,” including the detrusor apron, arcus tendineus, puboprostatic ligament, and some fibers of the detrusor muscle (Fig. 4).
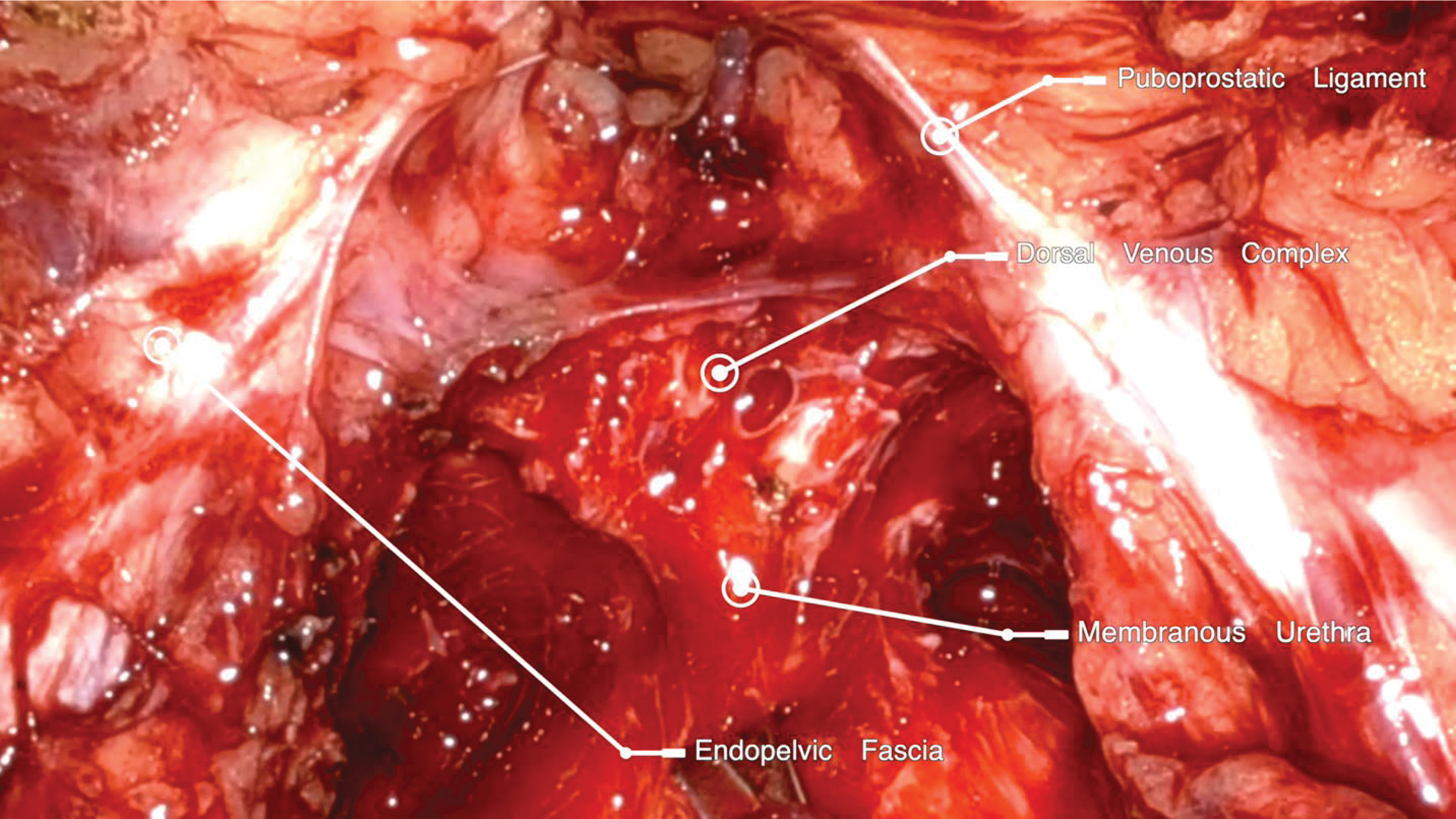
Preserved structure around prostate apex has the appearance of a “hood,” including the detrusor apron, arcus tendineus, puboprostatic ligament, and some fibers of the detrusor muscle. Color image can be found online.
Urethral length is maximized by rotating the prostate from side to side before final division. We then reapproximate the posterior Denonvilliers' fascia and the retrotrigonal fibromuscular tissue to the posterior rhabdosphincter with a running stitch of 3-0 V-loc. The dorsal venous complex is oversewn using a 3-0 V-loc suture in continuous manner. The anastomosis is then completed using a running stitch of a double-arm 3-0 barbed suture (Quill®). A Lahey stitch is performed to prevent lymphocele formation. Laparoscopically, a butterfly needle is used to perform a transversus abdominis plane block on either side. The specimen is then extracted through the midline port.
Simple prostatectomy
Previous studies demonstrated that the robotic technique is a safe and feasible approach for performing robot-assisted simple prostatectomy (RASP) for large-volume benign prostatic hyperplasia (>80 mL). 53 Furthermore, the robotic approach offers the advantage of reduced hospitalization stay and reduced blood loss. 53 However, the published literature on SP robotic simple prostatectomy is scarce, composed of a number of small case series.
In 2019, Steinberg et al. were the first to publish their experience with 10 patients who underwent extraperitoneal robot-assisted simple prostatectomy using the SP robotic system. 54 All patients effectively underwent the procedure without open conversion. Mean operative time and EBL were 172 minutes and 141 mL, respectively. Mean volume of adenoma resected was 65 g. Mean length of hospital stay was 1.1 days. Mean catheter time was 1.9 days.
In 2020, Kaouk et al. demonstrated their technique of SP percutaneous transvesical simple prostatectomy using the SP robotic system. 55 In the study, no cases required conversion to a MP robotic platform or open approach, nor required the placement of additional assistant ports. No intraoperative or postoperative complications were noted. Median operative time and EBL were 190 minutes and 100 mL, respectively. Mean volume of adenoma resected was 84.3 g. Median length of hospital stay was 19 hours. Postoperative catheterization time ranged between 7 and 12 days. Then, in a follow-up study published in 2022, these authors updated their results with 42 cases. 56
All procedures were effectively performed with no conversion, additional port placement, or intraoperative complication. Median length of hospital stay decreased to 4.6 hours after surgery. The median urinary catheter time for all cohort was 7 days and reduced to 3 days after technique adjustment for the last 19 consecutive patients. All patients had a significant postoperative improvement in maximum flow rate compared to baseline (19.0 mL/s vs 6.5 mL/s). 56
Most recently, Khalil et al. presented their study findings to compare intraoperative and short-term postoperative outcomes between the da Vinci MP and SP robots for patients undergoing RASP. 57 A minor increase in complication rate was recorded in the SP group; however, this did not reach statistical significance. SP-RASP is safe and shows equivalent perioperative outcomes when compared with the MP robotic system with the caveats that the present literature is composed of small case series performed by experienced robotic surgeons.
Radical cystectomy
Limited literature is available on surgical outcomes of radical cystectomies on the SP surgical platform. Overall, the existing case series support feasibility and safety in the short-term perioperative period of SP robotic radical cystectomy. 58 –60
In 2019, Kaouk et al. were the first to demonstrate their technique for robotic intracorporeal ileal conduit urinary diversion (ICUD) following radical cystectomy performed by using the da Vinci SP surgical system. 60 They performed four cases by replicating the steps of their institutional approach for intracorporeal ICUD performed with the MP robotic platform. In this study, they reported that mean robotic operative time for ICUD was 75 minutes. There was no conversion to standard MP robotic approach. One patient was converted to extracorporeal urinary diversion because of extensive adhesions of small bowels. No intraoperative complication was noted. All patients were discharged on postoperative day 5. One patient reported self-limited nausea and vomiting after discharge (Clavien grade I). 60
In 2020, Zhang et al. reported four cases using da Vinci SP system for ICUD following radical cystectomy. 59 All patients effectively underwent the procedure without intraoperative complications. The mean operative time was 270 minutes. The mean length of stay was 5.5 days. There was only one 30-day complication (Clavien grade II) and no additional 90-day complications. 59 In 2021, Gross et al. were the first group that compared intraoperative and short-term postoperative outcomes between the da Vinci MP and SP robots for patients undergoing radical cystectomy. 58 This retrospective study used propensity score analysis, including 12 SP cases and 24 MP cases.
On average, patients with an SP radical cystectomy had a lower lymph node yield than those with an MP radical cystectomy (11.9 vs 17.1, p = 0.034). All other perioperative outcomes, including operative time, blood loss, 90-day complication rates, 90-day readmission rates, and positive surgical margin rates, were not significantly different between the two groups. 58
Lower ureteral reconstruction
Similar to radical cystectomy, the published literature on SP robotic lower ureteral reconstruction is scarce, composed of case reports and small case series. In 2018, Kaouk et al. described their technique for robot-assisted ureteric reimplantation performed using the SP surgical platform. 61 The study included three patients diagnosed with distal benign ureteric strictures. An extra port for the bedside assistant was used for the first two procedures. All the cases were effectively completed without complications. 61 In 2019, Dobbs and colleagues demonstrated their techniques for SP cases, which the majority performed were SP prostatectomies for prostate cancer and nephrectomy (n = 32); however, four lower urinary reconstruction cases were performed, including vesicovaginal fistula repair (n = 2), and ureteral reimplantation (n = 2) with no conversions required to an open approach. 13 Based on these initial experiences, SP robot-assisted reconstructive urology surgery could be feasible and safe using the da Vinci SP surgical system. 13,61
Future of SP Robotic Surgery
Over the past decade, there have been significant advancements in the evolution of SP robotic surgery. From humble beginning with the Da-Vinci Si-based VeSPA systems to the second generation SP999 system and now with the most recent Da-Vinci SP platform, there have been significant improvements in the imaging and technical capabilities of these systems. The Da-Vinci SP platform provides versatility with an independent instrument clutch and pivot controls that allow positioning of instruments around the robot's remote center to help overcome some of the limitations of previous models.
As technology advances, the benefits of SP robotic surgery continue to manifest in a similar manner to the supplantation of conventional laparoscopy by MP robotic surgery. Furthermore, with the expiration of Da-Vinci patents for EndoWrist and other technologies in 2019, new manufacturers have emerged on the market, effectively ending the monopoly of Intuitive Surgical in this space. 62 The recently unveiled Enos robotic single-access surgical system (Titan Medical, Inc., Ontario, Canada) provides insight into next-generation SP robotic surgery. 62 The platform consists of a surgeon workstation with a 3D high-definition display and natural handle interface. The patient cart houses a 25 mm insertion tube through which two articulating arms and two (2D and 3D) lighted camera systems are placed. The arms are multiarticulated to bring flexibility and strength while grasping, suturing, and cutting tissues.
Ten tip types are under development for final release. MIRA®, the Miniaturized In Vivo Robotic Assistant (Virtual Incision, University of Nebraska, Lincoln, NE), is the world first miniaturized robotic platform weighing only 2 pounds. The platform includes a surgeon console and companion cart. MIRA does not require docking and can be inserted through a SP held in place with an adjustable stand. It consists of an endoscopic camera and two articulating arms that provide multiquadrant access. A complete suite of single use disposable instruments are available with the platform. Several other robotic platforms are currently under development in countries, including South Korea, Japan, and Germany. 62 These novel technologies are poised to continue to advance the role of SP robotics in the future.
Conclusions
In conclusion, SP robotic surgery continues to be a safe and viable option for a wide variety of urologic procedures, including radical and PN, pyeloplasty, radical and simple prostatectomy and radical cystectomy. The limited benefits over conventional MP robotic surgery, including decreased pain, decreased analgesic requirements, and shorter time in hospital, will continue to expand as the technology matures. As robotic technology advances, especially with the emergence of new manufacturers on the market, SP robotic surgery may well represent the future of surgery and will allow surgeons to perform complex procedures that were previously unimaginable.
Footnotes
Authors' Contributions
T.T.N.: Writing—original draft (equal); formal analysis (lead); and writing—review and editing (equal).
J.B.: Writing—original draft (equal) and writing—review and editing (equal).
A.S.N.: Writing—original draft (equal) and writing—review and editing (equal).
R.W.D.: Writing—review and editing (equal).
D.I.L.: Conceptualization (lead); Supervision; and writing review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.