
Abstract
Introduction:
The volume of surgeries including ureteroscopy (URS) performed for urolithiasis is increasing. This includes for the elderly population. The aim of this study was to evaluate the outcomes of URS in extremely elderly patients and identify any lessons that could be learned for clinical practice and treatment planning.
Materials and Methods:
Retrospective analysis was performed of consecutive patients aged 85 years and older undergoing URS between 2010 and 2022 at our tertiary center. Uni- and multivariable logistic regression analyses were performed to identify possible risk factors for complications. Survival analysis, stratified by age-adjusted Charlson Comorbidity index (ACCI), was performed using the Kaplan–Meier method as well as the log-rank test.
Results:
Sixty-four URS procedures were performed on 51 patients (mean age 88 years, range 85–97). Mean ACCI score was 7 (range 4–13) and most patients were American Society Anesthesiologists 3 (78%). Mean operative time and hospital stay were 60 minutes (range 15–120) and 2 days (range 0–6), respectively. At 3-month follow-up imaging, 92% were stone free (zero fragments). Intraoperative complication rate was 14% and in three cases (5%), early termination of the procedure was necessary. Eight patients (13%) suffered a complication before discharge. Eighteen patients (28%) had documented late complications after their surgery. The complication rate when combining early and late adverse events was 41%. One year mortality rate was 23%. Multivariable regression analysis revealed that operation time and ACCI >7 were significant predictors of complications after surgery. Survival probability was significantly worse in those patients with ACCI >7 (p = 0.0083).
Conclusion:
The morbidity burden of URS in the extremely elderly is higher than for other population groups. Risk should be considered carefully and implementation of ACCI can aid this process. High scores should prompt strong consideration of a conservative approach. Operation time should be kept to a minimum wherever possible.
Introduction
The lifetime prevalence of urolithiasis is 14% and patients >65 years are estimated to represent up to 16% of all stone patients. 1,2 Findings from national databases reveal that the volume of ureteroscopy (URS) procedures performed for stone disease is increasing across all age groups including the elderly. 1,3,4 Currently, international guidelines do not make any specific recommendations for the surgical treatment of stone disease in the latter group, which also represents the fastest growing age demographic. 5 There is a lack of randomized studies in this age setting given the standard is to exclude patients >65 years for trials. 6 Overall, the evidence basis to guide endourologic practice in this particular patient population is largely limited to only a small number of studies. 2,7 –10
Furthermore, the literature is even more sparce regarding patients who are extremely elderly. However, the reality is that it is not an uncommon scenario for a clinician to be faced with challenging management decisions regarding stone disease in an extremely elderly patient who may also have multiple comorbidities. To this end, our aim was to evaluate the outcomes of URS in extremely elderly patients and identify any lessons that could be learned for clinical practice and treatment planning.
Materials and Methods
Retrospective analysis was performed on consecutive patients aged 85 years and older undergoing URS for stone disease between 2010 and 2022 at Haukeland University Hospital (HUH), a tertiary center in western Norway. There were no exclusion criteria. This age cutoff was selected based on the current life expectancy in Norway (female: 84.9 years, male: 81.5 years). 11 Ethical approval was cleared by the regional committee (REK 469396) and the study was registered as a clinical audit at HUH (e-Protocol 3300-3300).
Primary outcomes of interest were intraoperative, early (predischarge), and late (postdischarge within 90 days) postoperative complications as well as mortality (30 days and 1 year). The electronic records at other hospitals in western Norway were also checked to capture any potential hospital readmissions during the postoperative period. Secondary outcomes of interest included stone-free rate (SFR), operative time, and hospital stay. Additional information was also collected on American Society Anesthesiologists (ASA) grade, comorbidities, age-adjusted Charlson Comorbidity Index (ACCI), 12 anticoagulation status, and postendoscopic exit strategy among other parameters.
Patients underwent follow-up imaging in the form of noncontrast CT at 3 months postsurgery. This was used to determine SFR, which was classified into three grades: Grade A (0 fragment), Grade B (≤2 mm fragments), and Grade C (2.1–4 mm fragments). A standardized technique was employed for semirigid URS (8F/9.8F; Richard Wolf Medical Instruments, Vernon Hills, IL) and flexible URS (8.4F URF-V3 or 7.95F P7; Olympus, Tokyo, Japan). The energy sources used were Holmium: YAG laser (Medilas H Solvo 30 W; Dornier MedTech) and Thulium Fiber laser (Soltive Premium 60 W; Olympus). The latter was introduced at our centre in 2020.
Decision to insert ureteral stent at the end of the procedure was at the discretion of the surgeon using criteria outlined in European Association of Urology guidelines. 13 At least 6 months and imaging confirming stone-free status were required before a case could be categorized as a new stone episode. Uni- and multivariable stepwise (forward and backward) logistic regression analyses were performed to identify possible risk factors for complications (early and late combined).
Survival analysis, stratified by ACCI, was performed using the Kaplan–Meier method as well as the log-rank test to investigate significant differences in survival curves. Overall survival was compared against the expected survival for patients of matched age and gender in Norway at the time of surgery using the R Package “relsurv,”, 14 based on data made available from the Human Mortality Database. 15 All statistical analyses were performed using R version 4.1.1. 16 For all analyses, statistical significance was determined as p < 0.05.
Results
Over the study period, 64 URS procedures were performed on 51 patients (Table 1). The majority were performed in an elective setting (81%). Mean age at time of surgery was 88 years (range 85–97). The mean ACCI score was 7 (range 4–13) and most patients were ASA 3 (78%). Hypertension (63%) and ischemic heart disease (58%) were the most frequently recorded comorbidities. The mean size of the index ureteral and renal stones was 8 mm (range 3–27) and 13 mm (range 4–30), respectively.
Patient and Stone Characteristics
ACCI = age-adjusted Charlson Comorbidity Index; ASA = American society anesthesiologists; URS = ureteroscopy.
Preoperative hydronephrosis was present in 85% of patients. Seventeen percent had undergone previous extracorporeal shockwave lithotripsy (SWL) without treatment success. Forty-two percent had originally presented with sepsis and obstruction requiring emergency decompression. Other presenting complaints included persistent pain (53%) and hematuria (3%). Operative data are listed in Table 2.
Operative Data
Supervised by consultant urologist or endourologist
Ureteral stricture distal to the stone at the time of URS was encountered in 22% of cases. Overall, 3% underwent Double-J stenting and were relisted, whereas balloon dilatation was effectively performed in 16% of the total patient sample. A small number ultimately received permanent nephrostomy (3%), if Double-J stent insertion was not effective, or relisting for a new URS attempt was not deemed appropriate. The latter was based on a shared decision with the patient, which took into consideration their wishes, comorbidities, and functional status. Regarding exit strategy, 77% received postoperative drainage.
The mean operative time and hospital stay were 60 minutes (range 15–120) and 2 days (range 0–6), respectively. At 3-month follow-up imaging with noncontrast CT, SFR rates were 92% (Grade A), 96% (Grade B), and 100% (Grade C). Seven percent had a new ureteral stricture identified. None of the patients with a new ureteral stricture had undergone balloon dilatation. Intra- and postoperative complications are given in Table 3. Intraoperative complication rate was 14% and in three cases (5%), early termination of the procedure was necessary (bleeding n = 2, sepsis n = 1). Eight patients (13%) suffered a complication in the early postoperative period and before discharge.
Summary of Complications
CD = Clavien–Dindo
Hospital readmissions were recorded in 27% of patients. Eighteen patients (28%) had documented late complications after their surgery. The complication rate when combining early and late adverse events was 41%. Multivariable regression analysis revealed that operation time and ACCI >7 were significant predictors of complications after surgery (Table 4). Although the 30-day mortality was 0, four deaths were recorded within the first 90 days postoperatively. Each of these cases was determined to be related to exacerbations of underlying medical conditions. At 1 year follow-up, nearly a quarter of all patients (23%) had died.
Multivariate Regression Analysis of Potential Risk Factors for Complications (Early and Late)
Bold indicates statistically significant results.
CI = confidence interval; OR = odds ratio.
When the patient sample was divided according to ACCI, survival probability was significantly worse in those patients with a score >7 (p = 0.0083) (Fig. 1A). This difference was even more pronounced when ACCI score of 9 was employed as a cutoff (Fig. 1B). There was no significant difference in survival between patients undergoing emergency and elective surgery. When comparing overall survival with the expected survival at a population level, these matched closely (Fig. 2). This would suggest that in general, patients live as long as would otherwise be expected. However, in the select group of patients with high ACCI scores, deaths can occur earlier than expected.

Overall survival based on age-adjusted Charslon Comorbidity Index. Color images are available online.
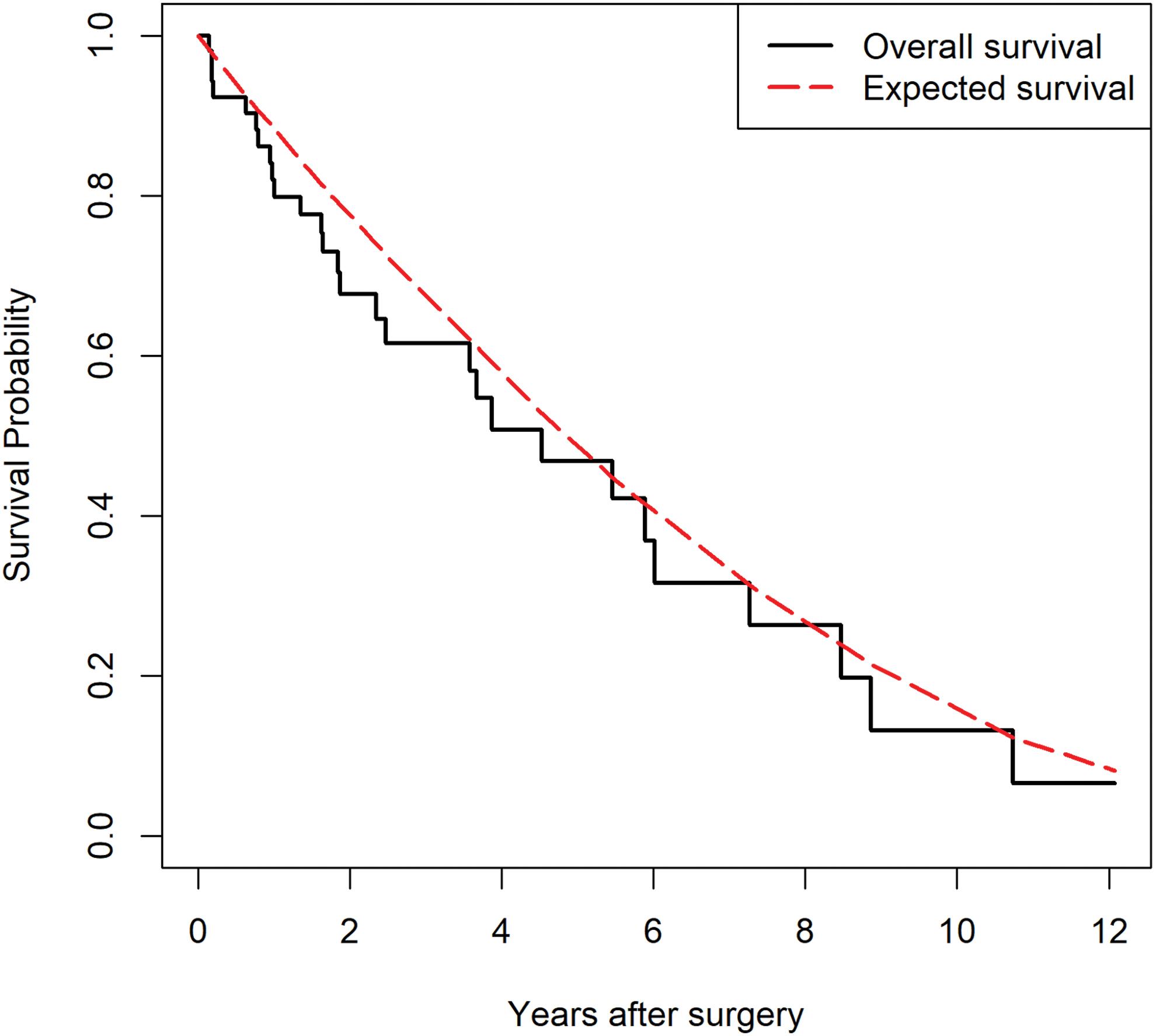
Overall survival of study group (black line) and corresponding expected survival (red line) of a matched cohort (by gender, age, and year of treatment) in Norway. Color images are available online.
Discussion
In this series of 51 patients of extreme age undergoing URS for stone disease, our results reveal that although it is feasible to perform this endourologic intervention in this special patient group, the overall postoperative complication rate (41%) is higher compared with results previously reported for the general adult population at our center (12%). 17 For the latter group, the operative time at our facility was also shorter (49 minutes) and 92% were discharged the same day. 17
In Norway, it is projected that one in six of the population will be >75 years by 2050. 18 The findings of this study are, therefore, of increasing relevance to daily clinical practice. Operation time and ACCI >7 were a significant predictor of surgical complications. Our findings highlight the role ACCI could play in assessing risk at the planning stage. Based on our findings, we recommend that when faced with an elderly patient with stone disease who is a possible candidate for URS, a careful and multidisciplinary approach should be taken.
The higher the ACCI score, the more strongly a conservative approach with permanent nephrostomy should perhaps be considered. The relatively high rate of new stricture formation (7%), which seems to be twice as high as what we have previously reported from our center in the general adult setting, also supports considering a more conservative approach. 19
Emiliani et al. recorded a postoperative complication rate of 9.5% in a similar study of patients aged 80 years and over. However, that study recorded hospital readmissions only within the first 30 days of surgery. Our rates may be higher as we included those occurring up to 3 months postsurgery. 7 Taguchi et al. reported a series of 27 patients with the same age cutoff as our study and their overall complication rate was much lower, at 3.7%. 20 However, in their study design, the authors assigned only five adverse events as fulfilling their study criteria for what could be deemed a postoperative complication. In that particular study, 30 days was also the follow-up period.
In a study by Berardinelli et al., again the postoperative complication rate was lower but their selection criteria excluded certain groups such as those with preoperative infection and neurologic disorders among others. 8 In our study, all causes of deaths were exacerbations of underlying medical conditions. Although the causes were not directly surgical related, it is possible that the patients' overall condition may have been worsened by the physiologic stress of their surgery in recent months and so these deaths have all been included as complications accordingly. Together with the longer follow-up period, this approach may serve to capture the true burden of undergoing URS in this age group and, therefore, be more representative.
Alternatives to URS for stone disease include SWL. Outcomes associated with the former are generally poorer than for the general adult population and several studies have identified lower age to be associated with more effective SWL treatment. 21 –23 The complication profile associated with SWL in the elderly has also been reported to be higher. 24 In addition, common comorbidities such as coagulopathy and dementia often preclude SWL as a treatment option.
The surgical indications reported for patients undergoing URS in our study reveal that it was nearly always to treat an obstructive and symptomatic stone burden. This is also reflected in the high rate of preoperative hydronephrosis (85%) on imaging recorded in this study compared with other patient groups previously recorded from our center. 19,25 In this regard, the clinician is largely focused on treating the culprit stone when the patient is elderly rather than clear the whole stone burden as may be the case in younger patients. 26
Limitations
This study is limited by its retrospective and single-center status. However, it does represent one of the largest reported series in extremely elderly patients. Our electronic health system also allows for complications admitted to other hospitals in western Norway to be accounted for. The complication period was set at 3 months rather than 30 days. As such, this study may have served to capture a more accurate morbidity and mortality burden after URS in this special patient group. The results can, therefore, represent a valuable contribution to an under-reported topic, yet one, which is of increasing relevance given the aging population.
Conclusion
Although it is feasible to perform URS in extremely elderly patients, the morbidity and mortality profiles are worse compared with younger groups. Clinicians should evaluate the individual risk profile carefully at the time of case selection and implementing routine use of ACCI could serve to aid this evaluation process. Higher ACCI scores should prompt the clinician to strongly consider a conservative approach.
Footnotes
Authors' Contributions
P.J.-J. contributed to conception (equal), methodology (equal), data collection (lead), formal analysis (equal), original draft (lead), review, and editing (lead). C.A.M. was involved in formal analysis (lead), methodology (supporting), original draft (supporting), writing—review and editing (supporting), and software (lead). J.N.H. carried out data collection (supporting), methodology (supporting), and writing—review and editing (supporting). P.G. was involved in data collection (supporting), methodology (supporting), and writing—review and editing (supporting). M.S.Æ. oversaw data collection (supporting), methodology (supporting), and writing—review and editing (supporting). C.B. took charge of conceptualization (supporting), supervision (supporting), methodology (supporting), original draft (supporting), review, and editing (supporting). Ø.U. carried out conceptualization (equal), supervision (lead), methodology (equal), formal analysis (supporting), original draft (supporting), review, and editing (supporting).
Author Disclosure Statement
Ø.U. has acted as a consultant for Olympus. The other authors have nothing to declare.
Funding Information
No funding was received for this article.