
Abstract
Background:
En bloc resection of bladder tumors (ERBT) has been used as a treatment option to improve pathologic diagnostic accuracy in non-muscle invasive bladder cancer. We report on the feasibility of a novel ERBT technique using an electrosurgical snare with flexible cystoscope: flexible cystoscopic En bloc Snare Resection of Bladder Tumor (f-ESRBT).
Methods:
We used the electrosurgical snare to resect a superficial bladder tumor after injection of 50% glucose in the submucosa at the tumor base. We collected each resected tumor with a basket catheter and coagulated the resected area with a coagulation electrode. A flexible cystoscope was used for all procedures.
Results/Discussion:
We performed 10 operations. Mean tumor size was 10.2 ± 7.3 mm and mean surgery time was 13.8 ± 6.8 minutes. All procedures were performed without complications. Results showed f-ESRBT to be simple and minimally invasive and to enable accurate pathologic diagnoses.
Conclusion:
f-ESRBT is a feasible treatment option for small and non-muscle invasive bladder cancer.
Introduction
Transurethral resection of bladder tumor (TURBT) is still the standard treatment for bladder tumors, and its primary objective is to achieve an accurate diagnosis of the bladder tumors while completely removing the growth with local staging. Non-muscle invasive bladder cancer (NMIBC) comprises approximately 75% of newly diagnosed bladder cancer, 1 and despite adequate therapy, approximately 30% to 50% of NMIBC patients will experience intravesical recurrence. 2 This high recurrence rate means that patients with NMIBC need frequent endoscopic follow-up and often require TURBT.
En bloc resection of bladder tumor (ERBT) is a surgical technique that aims to resect a bladder tumor in one piece. This process permits more accurate staging of bladder cancer, including proper assessment of the resection margins, than can be obtained from conventional TURBT. 3,4 Several modalities, including needle and loop type electrodes and lasers, have been proposed for use in ERBT. However, these modalities are usually performed with a rigid cystoscope. 5
In contrast, endoscopic mucosal resection (EMR), which is a well-defined technique used for superficial tumors in gastroenterology, is performed with an electrosurgical snare and flexible endoscope. 6 We hypothesized that flexible cystoscopic En bloc Snare Resection of Bladder Tumor (f-ESRBT) may provide higher-quality resection than conventional TURBT and that the invasiveness of the procedure will be minimized by using the flexible cystoscope.
In this study, we discuss the feasibility of a novel technique, f-ESRBT applied to a total of 10 tumors in 9 patients. We believe this to be the first report of ERBT using an electrosurgical snare with flexible cystoscope.
Methods
Patients
From June to December 2021, nine patients with bladder tumors were performed f-ESRBT in the Jikei University Kashiwa Hospital. Inclusion criteria were three of fewer tumors and tumor diameter <30 mm. Perioperative and pathologic outcomes were evaluated.
We received approval for the protocol from the Ethics Committee of the Jikei University School of Medicine. Informed consent was obtained from patients included in the study.
Surgical technique
Patients are treated in an operating room under spinal anesthesia with 0.5% hyperbaric bupivacaine hydrochloride hydrate. A 27-gauge disposable injection needle (NM-221C-0427; Olympus, Tokyo, Japan) is inserted through a flexible cystoscope (CYF-VA2; Olympus), and 1 to 3 mL of 50% glucose is injected into the submucosa at the base of each tumor. We use 50% glucose because it tends to sustain mucosal swelling better than saline or 5% glucose. The 50% glucose is injected completely around the tumor pedicle to elevate the entire tumor.
The electrosurgical snare (SD-7C-1; Olympus) with a diameter of 23 mm is inserted while looking through the cystoscope until the tip of the snare comes into view. The snare is opened and lassoed around the tumor, and then tightened after ensuring that nonelevated bladder mucosa is excluded from the snare. Once snagged, the tumor stalk is amputated at its base by blend cutting (20–30 W). The tumor is collected using a basket catheter (FG-24SX-1; Olympus). Although there is generally little or no bleeding from the resection site, we coagulate the resected area with an electrosurgical coagulator (CD-6C-1; Olympus). All procedures were performed with flexible cystoscope (Fig. 1).
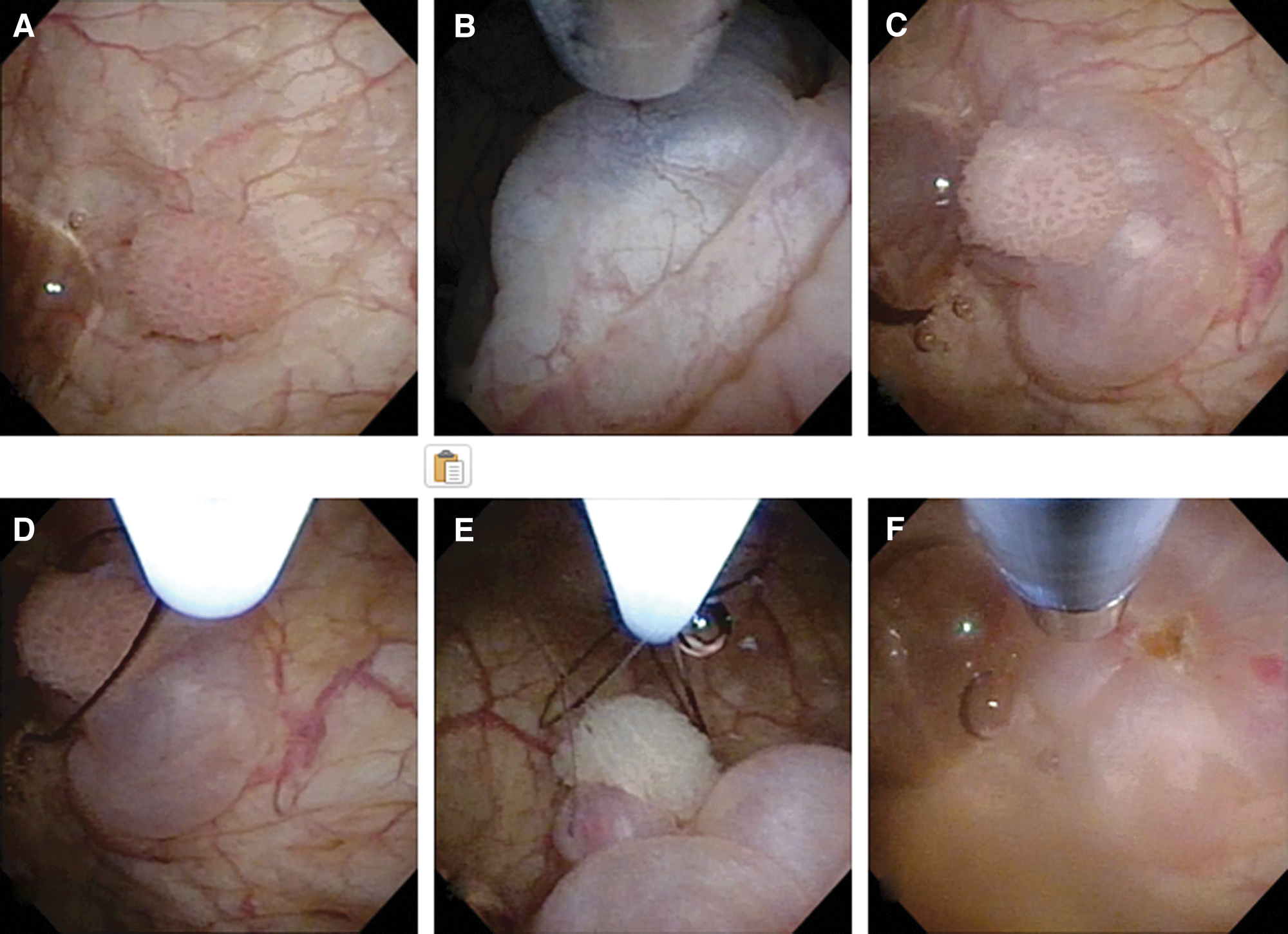
Description of the f-ESRBT surgical technique:
Results
A total of 10 tumors from 9 patients were treated by f-ESRBT. Patient and tumor characteristics are shown in Table 1. The mean tumor size was 10.2 ± 7.3 mm. Four tumors were located on the lateral wall, two on the posterior wall, and one each on the anterior wall, dome, trigone, and neck.
Characteristics
SD = standard deviation.
The mean surgery time for a single tumor was 13.8 ± 6.8 minutes. All procedures were performed without complications. All tumors were resected in one piece, and no residual tumor was noted macroscopically. The mean duration of catheterization after f-ESRBT was 2.7 ± 0.6 days. The results of operations are summarized in Table 2.
Intraoperative and Postoperative Data
Pathologic results showed eight specimens with urothelial carcinoma, of which seven were pTa and one was pT1. The other two specimens were benign: one instance of inverted papilloma and the other of cystitis. One patient had a pT1 urothelial carcinoma (UC), with no detrusor muscle tissue present in the specimen. We performed a repeat trans urethral resection (TUR) in that patient and found no residual tumor. The detrusor muscle sampling rate was 30% (Table 3).
Pathologic Data
Follow-up period was 12.75 ± 1.92 months. Two of seven patients with urothelial carcinoma experienced recurrence. Both patients received TURBT again and their results of pathology analysis was pTa.
Discussion of the Technology
TURBT is the standard treatment for NMIBC. But conventional TURBT causes tissue fragmentation and is thus not ideal for obtaining tumor samples for pathologic testing. ERBT has been gaining acceptance as there is increasing evidence that it improves the safety and quality if resected specimens of bladder tumors were used. However, it has not been widely adopted because of the complexity of the ERBT technique and the lack of robust evidence on oncologic outcomes.
In gastroenterology, EMR and endoscopic submucosal dissection (ESD) have become the standard procedures for superficial tumors. 7 EMR is a simpler technique than ESD and is indicated for tumors <2 cm because those tumors can be resected with a negative margin and have a low risk of submucosal invasion. ESD, which is performed for larger tumors and involves a variety of endoscopic tools, is technically more difficult and results in higher rates of perforation than EMR. However, for tumors >2 cm, ESD can be an effective and curative procedure. 6
Several variations of ERBT have been reported, including needle and loop electrodes, modified loop electrodes such as knife or J-shaped units, and laser energy devices, 8,9 all of which are similar in concept to ESD. A few instances have been reported of bladder tumor resection using electrosurgical snares and a rigid cystoscope, but none of the reported techniques has been widely accepted or adopted. 3 –5,10 –14
We developed the f-ESRBT technique for small bladder tumors based on the EMR concept rather than ERBT. In general, sampling the detrusor muscle is essential for diagnosing T1 and T2 bladder cancer and also for improving oncologic outcomes. 15 In contrast, there is no theoretical need to sample the detrusor muscle for the diagnosis of pTa bladder cancer, and no evidence on whether the presence of detrusor muscle in samples has any effect on oncologic outcomes in low-grade pTa bladder cancer. 16 ERBT allows us to evaluate the surgical margins, which is of considerable clinical importance as we have discussed previously. 3
In gastrointestinal pathologic diagnosis of EMR or ESD, the horizontal and vertical margins of a specimen are important indicators of thorough resection, and the presence of muscle in the samples is not considered particularly useful. In fact, the f-ESRBT specimens contain little detrusor muscle because the f-ESRBT procedure starts with submucosal injection of 50% glucose to lift the mucosal space from the underlying muscle, similar to the standard EMR technique.
We consider tumors of <1 cm to be appropriate candidates for f-ESRBT resection with a snare and collection of resected specimens with a basket catheter. The prognosis is good for low-risk bladder tumors, especially those <10 mm, 17 and we believe that detrusor muscle sampling is unnecessary for accurate diagnosis and good prognosis. When the vertical or horizontal margins of specimens are positive, or the specimens are pT1, we routinely schedule a repeat TUR. Further studies will be necessary to determine oncologic outcomes for f-ESRBT.
To our knowledge, this is the first report of this type of bladder tumor extraction using a flexible cystoscope. There are two merits of using the electrosurgical snare and flexible cystoscope. First, the electrosurgical snare procedure is as technically simple and safe as EMR. In this study, mean operation time was shorter than that reported for conventional TURBT or ERBT. 18 The risk of perforation is also low, similar to that seen with EMR, because the tumor is resected after injecting 50% glucose into the submucosa. Second, the flexible cystoscope is easier to operate and to observe through than a rigid cystoscope, and the flexible cystoscope is also less invasive to the urethra.
We use a 16.2F flexible cystoscope, much thinner than the 24F sheath of a rigid cystoscope, which reduces the risk of postoperative urethral stricture. 19 Most conventional TURBT and ERBT are performed under general or spinal anesthesia in the operating room. In this pilot study, f-ESRBT was performed under spinal anesthesia, but the less invasive nature of the flexible cystoscope may allow us to perform this procedure under local or intravenous anesthesia in clinics in the future.
Limitation
In our study of seven patients with pTa bladder cancer, five were high grade, and five of the specimens did not contain detrusor muscle. According to the current guidelines, repeat TURBT is recommended for patients with high-grade pTa bladder cancer if the tumors are large or if there is no muscle in specimen, but we did not perform repeat TURBT for these patients. The evidence in guidelines is based on the studies that bladder cancer was treated by conventional TURBT, not ERBT. In our previous study, we showed the possibility that repeat TUR can be omitted after ERBT in patients with pT1 bladder cancer and negative margins. 20 Based on our study, we hypothesize that repeat TURBT may be unnecessary after f-ESRBT in patients with pTa high-grade bladder cancer and negative margins. We would like to further increase the number of cases and verify the matter whether we can omit repeat TURBT for patients with pTa high-grade bladder cancer or not.
Conclusion
We performed a novel technique, f-ESRBT, for the purpose of minimizing the invasiveness and simplifying the procedure. This is the first report using electrosurgical snare and flexible cystoscope. Our findings indicate the feasibility of f-ESRBT in 10 bladder tumors. However, the limited number of cases means that further study is needed to validate the clinical utility of this procedure.
Footnotes
Authors' Contributions
A.M. contributed to the protocol and project development, data collection and management, data analysis, and article writing and editing. S.A. and Y.K. contributed to data collection. T.K., S.K., T.Y., K.O., and K.A. contributed to article editing. J.M. contributed to the protocol and project development and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.