
Abstract
Purpose:
Retropulsion of stone fragments during ureteroscopic laser lithotripsy (URSLL) remains a challenge for urologists and is associated with increased operative time and reduced stone-free rate (SFR). In this study, we compared the rate of retropulsion of ureteral stones during URSLL between the standard dorsal lithotomy (SDL) position and dorsal lithotomy position with reverse Trendelenburg (RT).
Materials and Methods:
Patients with ureteral stones requiring surgical intervention between May 2019 and January 2022 were randomized to undergo URSLL in either SDL or RT positions. The primary outcome of this study was stone retropulsion. Secondary outcomes included retropulsion to the kidney, SFR, operative time, 30-day emergency department visits and complications, and the need for conversion from semirigid to flexible ureteroscope. Differences between groups were evaluated using the chi-square test, Fisher exact test, Kruskal–Wallis test, or t-test.
Results:
A total of 114 patients were included in the study, with 57 patients in each group. There were no differences between groups in terms of baseline demographics or stone characteristics. Retropulsion was significantly less frequent in the RT group (68.4% vs 10.5%, p < 0.01). Similarly, the RT group was favored for lower risk of retropulsion into the kidney (40.4% vs 5.3%, p < 0.01), operative time (43.5 vs 33.0 minutes, p = 0.02), and need for ureteroscope conversion (16.7% vs 2.2%, p = 0.04). There was no difference in the SFR (100% vs 95%, p = 0.49).
Conclusions:
RT positioning during URSLL for ureteral stones significantly decreases the rate of stone retropulsion, operative time, and the need for conversion from semirigid to flexible ureteroscope.
Introduction
Since the 1980
Using an in vitro ureteral model, Patel et al. showed that retropulsion was inversely proportional to the incline angle, suggesting that placing patients in reverse Trendelenburg (RT) position during URSLL may be an effective strategy to decrease retropulsion. 11 To the best of our knowledge, no prospective in vivo study has evaluated the effect of the RT position on the rate of retropulsion during retrograde URSLL for ureteral stones.
The objective of this study was to determine whether RT position can be used to reduce stone retropulsion. It was hypothesized that the effect of gravity in the RT position would lead to significantly lower retropulsion rates compared with the standard dorsal lithotomy (SDL) position.
Materials and Methods
Patient recruitment and eligibility
This prospective randomized trial recruited patients with ureteral stones from two high-volume endourologists at a single academic institution. Institutional review board approval was obtained (IRB No. 19-00208), and patients were enrolled in the study from May 2019 to January 2022. All patients provided written informed consent with a guarantee of confidentiality.
Inclusion criteria consisted of age greater than or equal to 18 years and preoperative abdominal/pelvic CT imaging demonstrating the presence of at least one ureteral stone with total ureteral stone burden not exceeding 15 mm. The exclusion criteria were the presence of ureteral stones in two different anatomical ureteral segments, ureteral stricture, and anatomic urinary tract anomalies such as urinary diversion. Patients with pre-existing ureteral stents, concurrent ipsilateral renal stones, or those undergoing bilateral procedures were included in the study.
Study protocol
Before the initiation of the operation, patients were randomized in a 1:1 ratio using block randomization in alternating groups of three into one of two groups: a control group, in which patients were placed in the SDL position, and an intervention group, in which patients were placed in the SDL position and then moved to the RT position (20° of table incline), upon visualization of the stone. To facilitate surgical ergonomics and to maintain a comfortable standing position for the surgeon, the bed was raised to higher level while the patient was in the RT position (Fig. 1A, B). Patients were maintained in the assigned position until all stone fragments were removed. URSLL was performed using either a 120 W Ho:YAG laser with Moses™ technology (Lumenis Pulse™; Boston Scientific) or thulium laser (Soltive™; Olympus), based on the surgeon's preference.

All procedures were performed using a 200 μm laser fiber. During laser lithotripsy within the ureter, Ho:YAG settings were set to 0.5 J and 5 Hz (2.5 W), whereas the thulium laser settings were set to 1 J and 2 Hz (2 W). Τhe laser settings were adjusted according to the surgeon's discretion within the renal pelvis or calyces. The 7.5F Storz Flex X2 flexible ureteroscope and 6.5F Wolf dual channel semirigid ureteroscope were used, and the choice of whether to initiate the procedure with a semirigid or flexible ureteroscope was left to the surgeon's discretion.
Gravity irrigation with no additional pressure was used, and a saline bag was positioned 70 cm above the patient's abdomen. Lithotripsy was continued until all visible stone fragments could be safely removed and stone fragment extraction was performed using a stone retrieval basket. In the event of stone retropulsion to the renal pelvis, ureterorenoscopy was performed to basket or dust the migrated fragments. No ureteral access sheath was used, and the use of safety wires and stent placement were left to the surgeon's discretion.
Intraoperative parameters that were recorded included initial stone location, operative time, total laser energy used, number of ureteral segments of stone retropulsion, need for conversion from semirigid ureteroscope to flexible ureteroscope, and degree of impaction, as described in two previous studies by our group. 12,13
Primary outcome
The primary outcome was stone retropulsion during the surgery. For this study, the ureter was anatomically divided into three segments: proximal (ureteropelvic junction to iliac crest), middle (iliac crest to inferior border of the sacroiliac joint), and distal (inferior border of the sacroiliac joint to the ureterovesical junction). When a stone was noted to have migrated to a position proximal to its initial location, the ureteroscope was advanced to the new location of the stone and intraoperative fluoroscopy was used to determine whether a new ureteral segment had been entered. In this case, retropulsion was considered to have occurred. In the RT group, the C-arm was tilted 20° to maintain the fluoroscopic image perpendicular to the patient. If a stone moved proximally but remained within the same segment of the ureter, retropulsion was not considered to have occurred. The migration of stones from the ureter to the renal pelvis was readily evident on visual inspection. Stone retropulsion refers to retropulsion of the ureteral stone(s) of interest in patients who undergo treatment for concurrent ipsilateral renal stones or bilateral procedures.
Secondary outcomes
Secondary outcomes included retropulsion to the renal pelvis, operative time, SFR, postoperative emergency department (ED) visits, complications, and conversion from semirigid to flexible ureteroscope due to stone migration. Patients underwent follow-up imaging to assess residual stone burden with renal ultrasound and abdominal x-ray (kidney, ureter, and bladder radiograph [KUB]), and patients were considered stone free if there was no evidence of stone fragments on imaging. Conversion from a semirigid to flexible ureteroscope was considered to have occurred in procedures initiated with a semirigid ureteroscope, and transition to a flexible ureteroscope was necessary due to retropulsion of stone fragments that could not be reached with a semirigid scope. The SFR analysis included only patients who underwent imaging within 90 days of the procedure and those without concurrent renal stones/bilateral procedures. Similarly, the operative time analysis excluded patients who underwent concurrent renal stones/bilateral procedures.
Power analysis
A power analysis was performed for sample size estimation, based on the expected rate of retropulsion in a typical patient with a ureteral stone of 52%, based on published figures ranging from 28% to 60%. 4 An effect size of 50% was considered clinically meaningful. Setting α at 5%, the sample size required to achieve 80% power was calculated for 108 participants. Six additional participants were recruited to account for patient dropout, with a target of 114 participants.
Statistical analyses
Categorical data are presented as absolute numbers and relative frequencies. Nonnormally distributed data are summarized as median and interquartile range. Normally distributed variables are presented as mean ± standard deviation. Differences between groups were evaluated using the chi-squared test, Fisher exact test, Kruskal–Wallis test, or t-test, where appropriate. Multivariable logistic regression analysis was performed to account for the relevant patient and stone characteristics. Statistical analyses were performed using the R programming language and statistical environment (4.1.0). 14
Results
A total of 114 patients (57 in each group) were enrolled in the study, randomized, and included in the final analysis (Fig. 2; CONSORT diagram). Table 1 shows baseline patient demographics, stone characteristics, and intraoperative parameters. There were no differences between the two groups in terms of age, sex, American Society of Anesthesiology (ASA) score, body mass index, ureteral stone burden, stone composition, degree of stone impaction, presence of preoperative stent, laser fiber used, and initial stone location at the time of surgery. All stones underwent laser fragmentation before extraction.
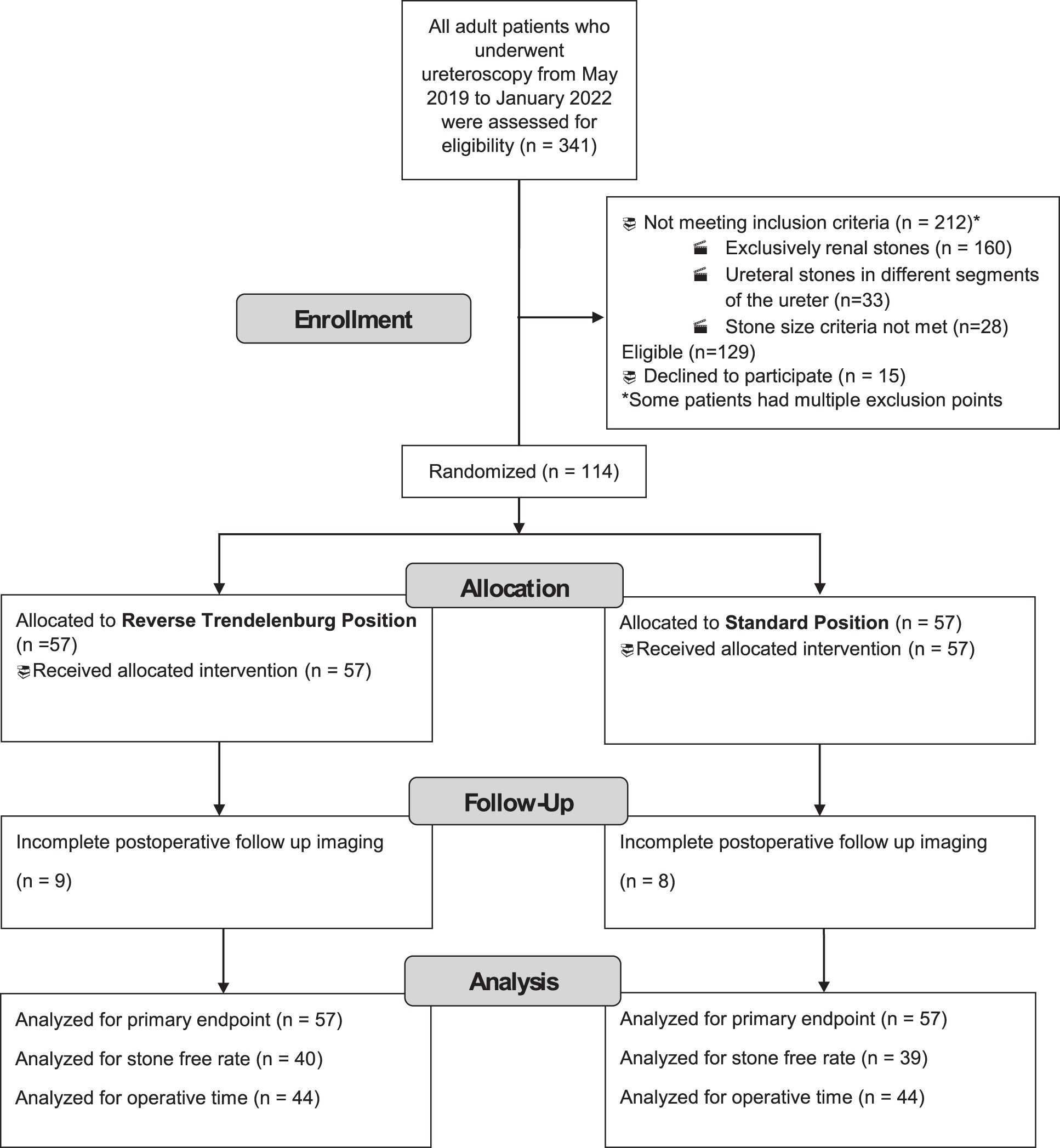
CONSORT diagram.
Baseline Patient Data, Stone Characteristics, and Intraoperative Variables
Position of ureteral stone as determined by a combination of visual inspection and fluoroscopy at the outset of the procedure.
Substances making up >50% of the entire stone composition; stone analysis by infrared spectroscopy.
Odds Ration cannot be calculated.
ASA = American Society of Anesthesiologists; BMI = body mass index; Ho:YAG = holmium:YAG; IQR = interquartile range; kJ = kilojoules; OR = odds ratio; RT = reverse Trendelenburg; TFL = thulium fiber laser.
Primary outcome
The overall rate of retropulsion in the RT group was significantly lower than that in the SDL group (6/57, 10.5% for RT vs 39/57, 68.5% for SDL; p < 0.01) (Table 2). When broken down by ureteral segment, there was a significantly higher rate of retropulsion in the SDL group for proximal (20/23, 86.9% for SDL vs 2/14, 14.3% for RT; p < 0.01) and distal ureteral stones (15/25, 60.0% for SDL vs 2/33, 6.06% for RT; p < 0.01). Retropulsion in the middle ureter occurred more frequently for patients in the SDL group (4/9, 44.4% for SDL vs 2/10, 20.0% for RT; p = 0.35) but did not reach statistical significance (Table 3).
Primary and Secondary Outcomes
Bold denotes statistical significance.
Determined using renal ultrasound and abdominal radiography (KUB).
Analysis excluded patients with concomitant ipsilateral nonobstructing renal stones.
Analysis included only patients for whom the procedure was initiated using a semirigid ureteroscope.
Analysis excluded patients who underwent bilateral procedures.
Odds Ration cannot be calculated.
ED = emergency department; KUB = kidney, ureter, and bladder radiograph; SFR = stone-free rates.
Rate of Any Retropulsion by Ureteral Segment in Each Cohort
Bold denotes statistical significance.
Position of ureteral stone as determined by a combination of visual inspection and fluoroscopy at the outset of the procedure.
Secondary outcomes
The rate of retropulsion into the kidney was higher in the SDL group than in the RT group (23/57, 40.4% for SDL vs 3/57, 5.3% for RT; p < 0.01). Similarly, operative time (43.5 minutes for SDL vs 33.0 minutes for RT, p = 0.02) and the rate of conversion from semirigid to flexible ureteroscope (6/36, 16.7% for SDL vs 1/46, 2.2% for RT, p = 0.04) favored the RT position. However, there were no significant differences in the SFR (39/39, 100% for SDL vs 38/40, 95% for RT, p = 0.49), 30-day ED visits (4/57, 7.02% for SDL vs 0/57, 0% for RT, p = 0.12), or overall complications (4/57, 7.02% for SDL vs 0/57, 0% for RT, p = 0.12) (Table 2).
Postoperative complications included four ED visits/Clavien complications in the SDL group and no ED visits/Clavien complications in the RT group. Of the four ED visits in the SDL group, two patients presented with urinary retention requiring Foley catheter placement (Clavien II) and two patients presented with flank pain. Of the patients with flank pain, one had a CT scan with no residual stone or hydronephrosis (Clavien II) and the other was found to have postoperative hydronephrosis secondary to ureteral stricture on postoperative day 25, requiring ureteroscopic laser incision with stent placement (Clavien IIIb).
A multivariate analysis was performed, including parameters with p-value <0.2 on the univariate. The multivariate analysis (Table 4) included the number of ureteral stones, initial stone location, operative time, use of flexible or semirigid ureteroscope at the beginning of the procedure, and study group. Patients in the SDL position were found to be 18.5 times more likely (p < 0.01) to have any retropulsion during the procedure, and none of the other parameters were found to independently affect the occurrence of retropulsion.
Multivariate Analysis to Determine Factors Predictive of Any Retropulsion
Bold denotes statistical significance.
Position of ureteral stone as determined by a combination of visual inspection and fluoroscopy at the outset of the procedure.
CI = confidence interval.
Discussion
Minimizing stone retropulsion remains a significant technical challenge during URSLL and has been associated with decreased SFR, increased operative time, and the need for repeat procedures. 3,15,16 This study indicates that RT positioning is an effective strategy for reducing ureteral stone retropulsion, which can also result in a subsequent reduction in operative time and the need to convert from a semirigid to flexible ureteroscope. The reduction in operative time likely resulted from the lack of need to “chase” stone fragments proximally up the ureter, as well as the reduction in the need to convert to a flexible ureteroscope. Furthermore, small stone fragments were more readily washed out of the ureter in the RT position, likely reducing basketing time. In addition to reducing operative time and presumably procedural costs, reducing the need for converting from semirigid to flexible ureteroscope can have profound impacts on practices in areas of the world where flexible fiberoptic ureteroscopes are not readily available.
There is no standard definition for retropulsion of ureteral stones in the literature. We found that the most common definition considers retropulsion to be the migration of stones from the ureter to the renal pelvis, likely because most studies assessing retropulsion include only proximal ureteral stones. The specific definition of retropulsion used in this study was chosen as the primary outcome because this event is rare for distal and middle ureteral stones. This definition of retropulsion improves granularity while maintaining adequate objectivity and clinical relevance for stones along the entire length of the ureter.
Previous studies have examined modifications in patient positioning to enhance the surgical outcomes during URSLL for ureteral or kidney stones. In two randomized studies by Zhou et al. 17 and Pan et al., 18 the Trendelenburg position (head down 30°) was used in patients with proximal ureteral stones. In both the studies, the rate of retropulsion was higher in the Trendelenburg position, but the SFR was also higher because retropulsed stones preferentially migrated to the upper pole calices, where treatment is easier compared with the interpolar and lower pole calices. When performing URSLL for renal stones, our group showed that the T-tilt position (15° Trendelenburg and 15° airplane away from the affected side) can increase the SFR from 76.7% to 92.1%. 19 In this study, a 20° table incline was used because it provides an optimal balance between antiretropulsion and surgical ergonomics. The current study adds to the literature as it is the first to investigate the utility of the RT position as a strategy to prevent retropulsion in vivo.
The major limitation of our study is that it was performed at a single academic center using gravity irrigation, pulse-modulated lasers, and specific laser settings, which potentially limits the generalizability of the results. Additionally, the SFR was assessed using renal ultrasound and KUB, which are less sensitive than CT scans. This was decided because post-URSLL CT is not routine in our practice to avoid additional radiation and costs to the patients. Besides, both groups were evaluated using the same modalities making the comparison of the SFR possible. Finally, the rate of proximal ureteral stone was higher in the SDL group, besides randomization, which may have skewed the results. Multivariate analysis was performed to mitigate this possibility, showing that stone location at the beginning of the procedure was not associated with the occurrence of retropulsion. The RT position during URSLL was found to be the only parameter that was independently correlated with decreased retropulsion and could be used to decrease stone retropulsion and improve URSLL efficiency.
Urologists have utilized various strategies to reduce retropulsion, such as antiretropulsive devices, antiretropulsive laser modalities, and even antegrade irrigation via pre-existing nephrostomy tubes. 3,4,10,15 Despite their proven benefits to patient outcomes and overall reduction in per-procedure costs, 16 according to a multicenter study by Saussine et al., antiretropulsion devices are only used in 14.5% of URSLL cases worldwide. 3 We posit that this underutilization is due to a combination of upfront costs, the need for additional training, and surgeon inertia. Additionally, such devices must be placed alongside the ureteroscope, which can be difficult in patients with a small ureteral caliber and may limit maneuverability. 20 Compared with other antiretropulsion technologies, intraoperative RT positioning is cost-free, requires no additional operative time or training, poses virtually no risk to the patient, and is readily available in most operating rooms worldwide. Therefore, we have implemented RT positioning in our own practice and suggest that urologists should consider placing patients in the RT position to reduce ureteral stone retropulsion.
Conclusions
The RT position is effective in reducing the rate of retropulsion during URSLL for ureteral stones, with the added benefit of reducing operative time and the need for conversion from semirigid to flexible ureteroscopy. Future studies should corroborate our results by using different irrigation methods, laser devices, and laser settings.
Footnotes
Authors' Contributions
H.A.: Data curation, drafting of the article, writing, review and editing, methodology. A.J.Y.: Data curation, writing, review and editing, methodology. J.A.K.: Writing, review and editing, investigation. R.C. and A.S.: Data curation, investigation. D.L.: Methodology, formal analysis. J.N.B., B.G., and R.S.: Project administration. W.M.A.: Conceptualization, investigation, writing, review and editing. M.G.: Conceptualization, investigation, writing, review and editing, supervision.
Author Disclosure Statement
M.G. acts as a consultant for the following companies: Olympus America, Cook Medical, Boston Scientific Corporation, and Travere Therapeutics. W.M.A. acts as a consultant for Boston Scientific Corporation.
Funding Information
No funding was received for this article.