
Abstract
Purpose:
To investigate the efficacy and safety of single-port (SP) robotic transperitoneal (TP) and retroperitoneal (RP) partial nephrectomy.
Materials and Methods:
We sequentially analyzed 30 partial nephrectomy performed after the SP robot was introduced to the hospital in September 2021 to June 2022. All patients were found to have T1 renal cell carcinoma (RCCs) and were operated by a single expert in conventional robot with da Vinci SP platform.
Results:
Total of 30 patients underwent SP robotic partial nephrectomy with 16 (53.33%) by TP approach and 14 (47.67%) by RP. Body mass index was slightly higher in TP group (25.37 vs 23.53, p-value = 0.040). The other demographic information was not significantly different. There was no statistical difference in ischemic time (727.41 ± 561.18 seconds for TP and 698.56 ± 299.23 seconds for RP, p-value = 0.812), and console time (67.97 ± 24.06 minutes for TP and 69.71 ± 28.66 minutes for RP, p-value = 0.724). There was no statistical difference in perioperative and pathologic outcomes either. Postoperative renal function calculated from diethylenetriaminepentacetate was 103.33 mL/min/1.73 m2 for TP and 101.33 mL/min/1.73 m2 for RP (p-value = 0.214). And 90.36 mL/min/1.73 m2 for TP and 87.74 mL/min/1.73 m2 for RP at 90 days after surgery (p-value = 0.592).
Conclusion:
SP robot partial nephrectomy can be performed effectively and safely regardless of the approach. TP and RP approach offers similar perioperative and postoperative outcomes for T1 RCC.
The Clinical Trial Registration number KC22WISI0431.
Introduction
In 2021, 6,244 and 76,080 patients were newly found to have kidney cancer in the Republic of Korea 1 and the United States, 2 respectively. The prevalence of kidney cancer has increased with the development of imaging techniques and diagnostic methods. 3 The detection rate of early kidney cancer also shows a steep increase. In particular, 90% of newly discovered kidney cancers are renal cell carcinomas (RCCs). 4 RCC is a disease with a big difference in prognosis between early and late detection. The prognosis of patients with RCC is good if detected early. 5
Partial nephrectomy is a well-known standard treatment for T1 (≤7 cm) RCC. 6 Partial nephrectomy is a safe procedure with few side effects and prevents the transition to chronic kidney disease. With the advent of the era of robots, robotic nephrectomy is now widely used. In 2018, a single-port (SP) robot was approved by the U.S. Food and Drug Administration (FDA). Since then, various techniques have been tried using this robot. 7 Partial nephrectomy using an SP robot is one of those attempts, and its stability has been proven in several studies. 8,9
Urologists know that transperitoneal (TP) and retroperitoneal (RP) approaches are possible in partial nephrectomy. They can choose the approach depending on the location of the tumor and their preference. However, a comparison of these two surgical methods in SP robots has not been made to the best of our knowledge. Thus, the objective of this study was to investigate the efficacy and safety of SP partial nephrectomy.
Materials and Methods
Study population
From September 2021 to June 2022, 30 sequential cases of partial nephrectomy performed after an SP robot was introduced to our hospital were analyzed retrospectively. All patients were found to have T1 RCC by CT scans or MRI. Surgeries were performed by a single expert with many years of experience with the da Vinci Xi platform. All operations were performed with the da Vinci SP platform (Intuitive Surgical, Sunnyvale, CA). Indications for SP other than da Vinci Xi were a T1a of 4 cm or less. However, even in T1b, SP was selected when it was exophytic and when the nephrometry score was low. The study protocol was reviewed by Seoul St. Mary's Hospital Institutional Review Board (KC22WISI0431). Informed consent was waived because of its retrospective design. Regardless of the surgical method, pre- and postoperative care was performed using the same type of critical pathway.
Surgical technique
The TP approach surgery was performed as follows. After making an incision line next to the umbilicus, a 25-mm gel port was inserted for air-docking, and a pneumoperitoneum was constructed. After checking the abdominal cavity using a camera, an 11-mm assist port was added according to the location of the tumor. The camera was placed at 12 o'clock, and monopolar scissors were placed at 3 o'clock when surgery was started. When performing medial mobilization of the intestine, Cadiere forceps were placed at 6 o'clock, and Maryland forceps were placed at 9 o'clock in both left and right tumor cases. When approaching the renal hilum, the position of the Cadiere forceps and scissors was changed in the case of a left tumor. Cadiere forceps and Maryland forceps were changed in the case of a right tumor to lift the kidney with Cadiere forceps.
During tumor resection, because Maryland forceps are sharp with a risk of tumor violation, the Maryland and Cadiere forceps were exchanged. Maryland forceps were used for traction, and Cadiere forceps were used as the left main instrument for resection. When additional traction was required because the intestine obscured the field of vision, the intestine was sutured using a Carter-Thomason device, and a thread was fixed outside the skin for traction. If the angle was not sufficient, the Cobra mode was also used (Fig. 1). The following step was performed similarly to the multiport or laparoscopic procedure, but with minor modifications.

Instruments configuration of RP approach. Red dot: assist port, blue dot: docking port. RP = retroperitoneal. Color images are available online.
The RP approach was performed in a similar way to that introduced by Maurice et al. 10 An incision line was made between the 11th rib and the pelvic limb but placed slightly biased toward the rib to prevent the robotic arm from colliding with the pelvic bone. After securing sufficient RP space using a balloon, a 25-mm gel port was inserted. An 11-mm assist port was inserted 2 cm anteriorly and 2 cm inferiorly from the anterior superior iliac spine. At the start of surgery, the camera was positioned at 12 o'clock, and Maryland forceps were placed at 6 o'clock. In the case of a left tumor, Cadiere forceps were positioned at 9 o'clock, and monopolar scissors were placed at 3 o'clock to directly access the renal hilum by lifting the kidney.
In the case of a right tumor, Cadiere forceps were positioned at 3 o'clock, and monopolar scissors were placed at 6 o'clock. When the space dissection was inadequate, Gerota's fascia was sutured using a Carter-Thomason device and fixed outside the skin for traction. When performing tumor resection, similar to TP, Maryland forceps and Cadiere forceps were exchanged to use Maryland forceps for traction and Cadiere forceps as the main left-handed instrument. If the angle was not good, the Cobra mode of the camera was used as in TP (Fig. 2).
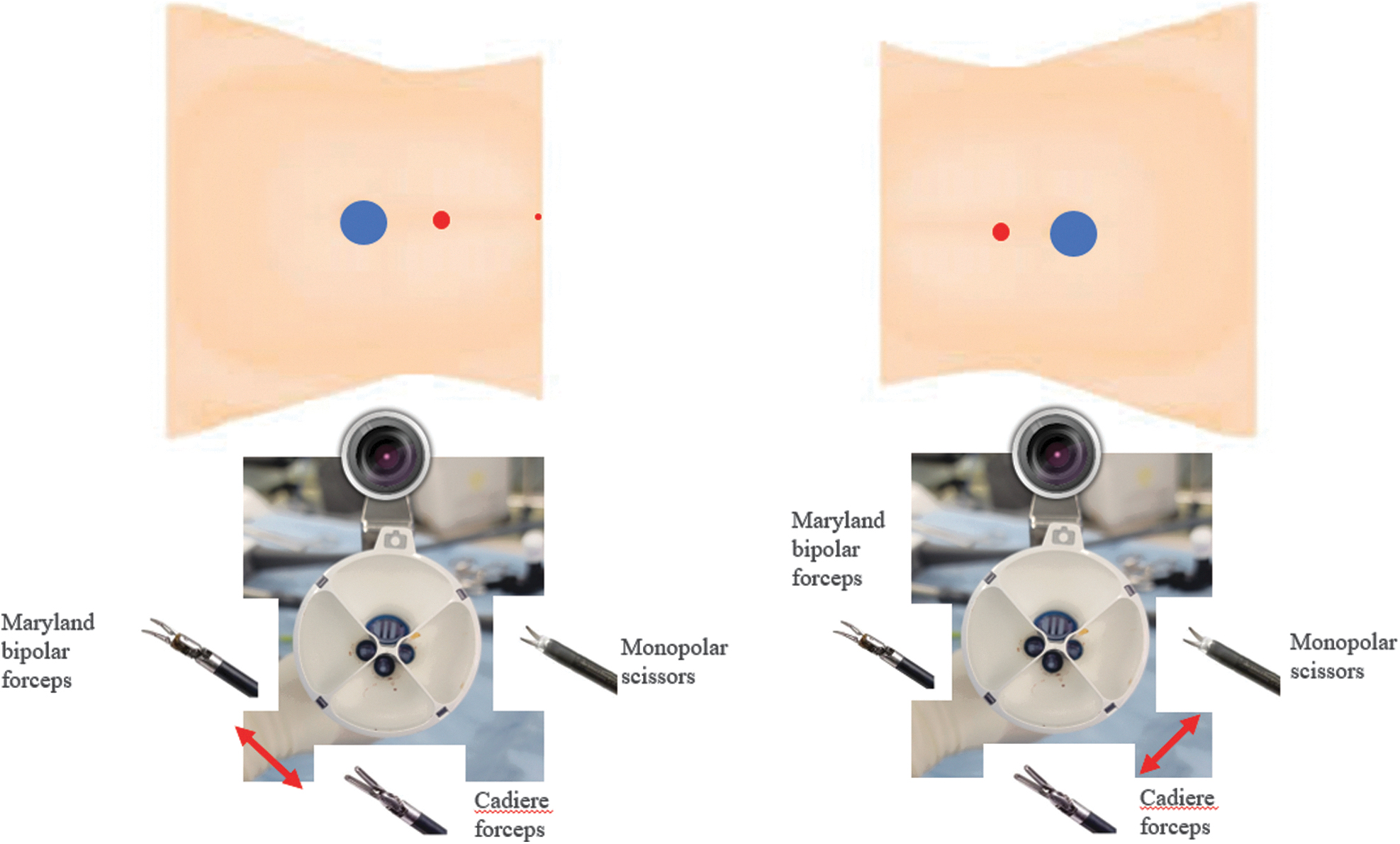
Instruments configuration of TP approach. Red dot: assist port, blue dot: docking port. TP = transperitoneal. Color images are available online.
In both TP and RP procedures, the renal artery was dissected and marked as a vessel loop. After exposing the tumor and confirming it using ultrasound, if necessary, the renal artery was blocked using a bulldog clamp, and the tumor was removed. The resection bed was sutured using a barbed thread. Renorrhaphy was then performed.
Study outcomes
We recorded all patients' basic characteristics, total surgery time, console time, and warm ischemic time. The R.E.N.A.L nephrometry score (radius, endophytic/exophytic, nearness, anterior/posterior, localization) 11 and tumor size were also collected. The patients' postoperative complications were classified according to the Clavien–Dindo classification. 12 The length of hospital stay was calculated immediately after surgery. All patients received postoperative care following the same critical pathway.
The day after surgery, the Foley catheter was removed from all patients, and they were allowed to drink water. The Jackson–Pratt drain was removed. Patients were discharged on the third or fourth day after surgery. The collected specimens were analyzed by the pathology department. Cell type and margin invasion were recorded separately. Continuous variables were analyzed with Mann–Whitney U tests. Categorical variables were compared with the chi-squared test or Fisher's exact test. All statistical analyses were conducted using SPSS version 24 (IBM, Chicago, IL). Statistical significance was considered for p-values of <0.05.
Results
A total of 30 patients underwent SP robotic partial nephrectomy, including 16 (53.33%) by the TP approach and 14 (47.67%) by the RP approach. The mean age of the patients was 50.13 years, 48.13 years in the TP approach group, and 52.43 years in the RP approach group (p-value = 0.344). Body mass index was slightly higher in the TP group than in the RP group (25.73 in the TP group vs 23.53 in the RP group, p-value = 0.040). Other demographic characteristics showed no significant differences between the two groups. There was no difference in operation time, ischemic time, or console time (Table 1).
Baseline Demographic Information
BMI = body mass index.
In perioperative outcomes, there was no significant difference in estimated blood loss (136.25 mL in the TP group vs 136.43 mL in the RP group, p-value = 0.997). The R.E.N.A.L nephrometric score was 4.19 in the TP group and 4.36 in the RP group, showing no significant difference (p-value = 0.319). Cell type was confirmed as a clear cell type in 26 of 30 patients. It was a chromophobe type in one patient in the RP group. Angiomyolipoma was found in two patients in the TP group and one patient in the RP group. Again, no statistically significant differences were seen between the two groups. No positive surgical margins were found in patients in either group (Table 2).
Perioperative Data
AML = angiomyolipoma.
Postoperative complications classified by the Clavien–Dindo classification occurred only in one patient in the RP group. This patient was discharged on the ninth day after surgery because triglycerides were observed in the drainage tube after surgery.
We also evaluated renal function using serum creatinine and the estimated glomerular filtration rate, as well as a diethylenetriamine pentaacetic acid kidney scan. There were no significant differences in preoperative, postoperative, or follow-up test results at 3 months between the two groups (Table 3).
Pre- and Postoperative Renal Function
DTPA = diethylenetriaminepentacetate; eGFR = estimated glomerular filtration rate.
Discussion
The results of this study confirmed the efficacy and safety of SP partial nephrectomy. There were no significant differences in surgical results between TP and RP approaches in partial nephrectomy using an SP robot. This means that either approach could easily be used depending on the location and surgeon's preference. In particular, the safety of the RP approach was confirmed once again through this study. Since the FDA approval of an SP robot in 2018, few reports confirming the significance of the RP approach have been published.
Palacio et al. compared the results of multiport and SP RP partial nephrectomy, but no comparisons according to the approach in SP platforms have been made. 13 The RP approach through a multiport robot is a technique that is tried frequently. However, there is a limitation to its use because the space between trocars has to be narrow. However, as the surgical safety of partial nephrectomy through an SP robot has been proven, it is expected to be used more. The operator of this study had a lot of experience with a conventional robotic platform but only completed SP procedures using animals. However, the operator had no difficulty in adapting to human surgery.
The greatest advantage of surgery using an SP is that it is the most noninvasive method known so far. When using a multiport robot, at least five trocar sites are incised, including an assist port. Also, depending on the size of the tumor, sometimes it is necessary to extend the incision. However, if an SP is used, these wounds can be minimized. In addition, an SP procedure can be performed without touching the inside of the abdominal cavity if there is a history of abdominal surgery in the RP approach. If the RP approach is performed, the operation might be a little more difficult because of the narrow space. However, there was no inferiority in surgical outcomes in this study. In addition, with a da Vinci SP platform, it is possible to overcome a case where the angle to view the tumor is not good by using the Cobra mode of the camera, and side effects, such as bleeding and hernia, can be reduced.
In this operation, we formed air-docking using a gel port. By forming air-docking, as already introduced in other studies, 8,14 we were able to secure more surgical area in a limited space. Introducing this technique can be a good way to overcome the limitations of the spatially limited RP approach. In this study, we used one additional assist port. However, it is expected that surgery can be performed without the use of additional ports using a gel port. An evaluation of these trials at a later date may be considered. By doing so, it seems that the full advantages of true SP surgery can be realized.
Glomerular filtration rates estimated from serum creatinine and diethylenetriaminepentacetate (DTPA), which were collected for evaluating renal function after surgery, showed no difference in renal function decline between the TP and RP groups. This result proves the safety of this type of surgery, regardless of the approach. In some cases, serum creatinine levels were decreased on the first day of surgery, presumably because of sufficient hydration during inpatient treatment. In DTPA, a loss of renal function of about 10% was observed at follow-ups 3 months after surgery (p-value <0.001). However, this loss was not significantly different compared with the loss of renal function that occurred during laparoscopic or open surgery reported by Dagenais et al. 15
To avoid selection bias as much as possible in this study, we selected 30 consecutive surgeries performed immediately after the SP robot was introduced into the center. Nevertheless, there were still some limitations related to the direction of the performed surgeries. In our study, almost all patients (14/16) with the TP approach underwent surgery on the right side, which might be because the authors thought tumors located on the right side and lower pole of the kidney benefit from SP surgery with a TP approach.
The TP and RP approach decisions were independent of nephrometry scores such as size or complexity. The approach was determined only depending on whether the tumor was located anteriorly or posteriorly. In the case of tumors located on the lateral side, the RP approach was preferred if it was expected that kidney dissection and mobilization would be required for tumor resection and renorrhaphy. In addition, RP surgery seemed to be able to compensate for disadvantages, such as the longer console time of upper pole surgery in TP. 16
For obese patients with thick peripheral fat, the TP approach was preferred because of space limitations. However, the advantage was anatomical rather than surgical, which was favorable to the patient. Also, what we wanted to clarify and prioritize through this study was the stability of the SP RP approach, which was not commonly performed. Thus, limitations regarding this direction cannot be said to have great meaning.
However, this study still had some limitations because of its retrospective nature and surgeries performed by a single operator. Future research is needed to overcome the limitations of this study by conducting prospective studies on a larger scale.
Conclusion
SP robot partial nephrectomy was performed effectively and stably regardless of the approach. Both TP and RP approaches offer similar perioperative and postoperative outcomes for T1 RCC. SP surgery could be a good method for treating T1 RCC with minimal invasion.
Footnotes
Authors' Contributions
Conceptualization and writing—review and editing by S.B. and S.H. Data curation by D.S., H.W.M., and U.H. Formal analysis by S.B., J.Y.L., and S.H. Methodology and writing—original draft by S.B. Project administration by H.J.C. and J.Y.L.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Research Fund of Seoul St. Mary's Hospital, The Catholic University of Korea. Grant number: ZC22RISI0851.