
Abstract
Introduction:
We sought to examine the practice patterns of pain management in the emergency room (ER) for renal colic and the impact of opioid prescriptions on return ER visits and persistent opioid use.
Methods:
TriNetX is a collaborative research enterprise that collects real-time data from multiple health care organizations within the United States. The Research Network obtains data from electronic medical records and the Diamond Network provides claims data. We queried the Research Network for adults who visited the ER for urolithiasis, stratified by receipt of oral opioid prescriptions, to calculate the risk ratio (RR) of patients returning to the ER within 14 days and persistent opioid use ≥6 months from the initial visit. Propensity score matching was performed to control for confounders. The analysis was repeated in the Diamond Network as a validation cohort.
Results:
There were 255,447 patients in the research network who visited the ER for urolithiasis, of whom 75,405 (29.5%) were prescribed oral opioids. Black patients were less likely to receive opioid prescriptions than other races (p < 0.001). After propensity score matching, patients who were prescribed opioids had an increased risk of a return ER visit (RR 1.25, confidence interval [95% CI] 1.22–1.29, p < 0.001) and persistent opioid use (RR 1.12, 95% CI 1.11–1.14, p < 0.001) compared with patients who were not prescribed opioids. These findings were confirmed in the validation cohort.
Conclusions:
A significant proportion of patients presenting to the ER for urolithiasis receive opioid prescriptions, which carries a markedly increased risk of return ER visits and long-term opioid use.
Introduction
Acute renal colic in the emergency setting poses a challenging management dilemma for providers. It requires clinicians to weigh several factors, including the safety, efficacy, availability, and cost of medications, as well as patient and provider preferences. 1,2 The analgesics most used for renal colic include opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), and acetaminophen/paracetamol. Each of these drugs comes with its own advantages and disadvantages and the perfect algorithm for analgesic control remains elusive.
Opioids are commonly used because of their availability, rapid onset, route of administration, and ability for dose titration. However, they pose significant acute and chronic risks. Immediate adverse effects are common and can include gastrointestinal discomfort, sedation, respiratory depression, and hypotension. 3 Furthermore, the negative consequences of opioid administration may be long-lasting, with significant rates of new addiction and abuse seen after medical prescription of even a single course. In fact, 9% of patients receiving opiates at the time of kidney stone diagnosis remain on narcotics after three to six months. 4 Alternatively, NSAIDs have been shown to provide superior pain control for renal colic with a decreased need for rescue analgesics and a lower rate of adverse effects. 5 The role of acetaminophen/paracetamol for renal colic is less clear, but it has a superior safety profile and possibly even demonstrates comparable analgesic affects. 3
Although the European Association of Urology (EAU) recommends nonopioid analgesics such as NSAIDs as first-line therapy, opioids still play a significant role in the treatment strategy for renal colic. 6,7 Given the trepidations about opioid overuse, it is vital to understand practice patterns regarding opioid administration for renal colic in the emergency setting. The objective of this study was to identify the incidence of opioid prescription for acute renal colic, risk factors, and the impact of opioid prescriptions on return visits and persistent opioid use.
Methods
The TriNetX Analytics Network (Cambridge, MA) was utilized for this analysis. TriNetX is a collaborative research enterprise that collects real-time data from multiple health care organizations (HCOs) within the United States and comprises a Research Network and a Diamond Network. The Research Network obtains data from electronic medical records and is represented primarily by academic facilities. As of May 2022, this network contains 87 million patients in 58 HCOs. The Diamond Network provides claims data but captures a much wider patient population, with 212 million patients from 92 HCOs.
Exploratory analysis was performed using the Research Network, followed by validation using the Diamond Network. The rationale for these analyses, despite some inevitable overlap between the two databases, was to check the robustness of the findings in the Research Network (exploratory cohort) with the less detailed Diamond Network (validation cohort). The same search terms and statistical methods were applied in both analyses. The database was queried for adults (≥18 years) who visited the emergency room (ER) for urolithiasis between January 1, 2010 and December 31, 2019, stratified by receipt of oral opioid prescriptions.
The coding query used to identify patients is listed in Supplementary Table S1. Persistent opioid use was defined as having an active prescription for opioids at a time point 6 months from the index ER visit. Baseline clinicodemographic characteristics were compared using comparative statistics (Student's t-test, χ 2 test). Propensity score matching in a 1:1 manner using the greedy nearest neighbor algorithm was performed to control for confounders. The risk ratio (RR) of patients returning to the ER within 14 days and of persistent opioid use ≥6 months from the index ER visit was calculated.
This study is considered exempt by the Johns Hopkins Institutional Review Board because of the deidentified nature of the data. All analyses were performed using software within the TriNetX platform, and statistical significance was set at α = 0.05.
Results
Exploratory cohort
We identified 255,447 patients in the TriNetX Research Network who visited the ER for urolithiasis, of whom 75,405 (29.5%) were prescribed oral opioids (“A” in Table 1). Patients receiving oral opioids were younger (47.6 years vs 48.3 years, p < 0.001) and comprised more women (48.0% vs 47.0%, p < 0.001) than those who did not receive oral opioids. A higher proportion of White patients received opioid prescriptions than any other race (p < 0.001).
Clinicodemographic Characteristics of the Exploratory Cohort, Stratified by Administration of Oral Opioids at the Index Emergency Room Visit
Significant differences were noted in all aspects of the listed medical history; notable differences included a higher rate of new oral opioid prescription among those with a history of anxiety (25.0% vs 15.2%, p < 0.001), chronic pain (14.0% vs 7.8%, p < 0.001), substance abuse (24.3% vs 13.7%, p < 0.001), and urolithiasis (35.9% vs 21.4%, p < 0.001). Oral opioid administration was also higher among those with a documented history of an ER visit (62.1% vs 41.1%, p < 0.001) and prior urologic surgery (14.7% vs 10.4%, p < 0.001). Finally, patients receiving oral opioids at the time of the index ER visit had higher rates of analgesic medication use, including acetaminophen, benzodiazepines, NSAIDs, and opioids.
There were 26,874 patients (10.5%) who visited the ER within 14 days of the index visit, of whom 9925 patients were prescribed oral opioids and 16,949 were not prescribed oral opioids. Unmatched analysis demonstrated that patients who were administered oral opioids at the index visit were 40% more likely to return to the ER than patients who did not receive oral opioids (RR 1.40, confidence interval [95% CI] 1.37–1.43, p < 0.001) (“A” in Table 2). Among those who returned to the ER, the majority did so only one time (Fig. 1). Furthermore, among those with a return ER visit, patients who received oral opioids at the index visit were more likely to visit the ER more often than those who did not receive oral opioids (1.23 return visits vs 1.16 return visits, p < 0.001).
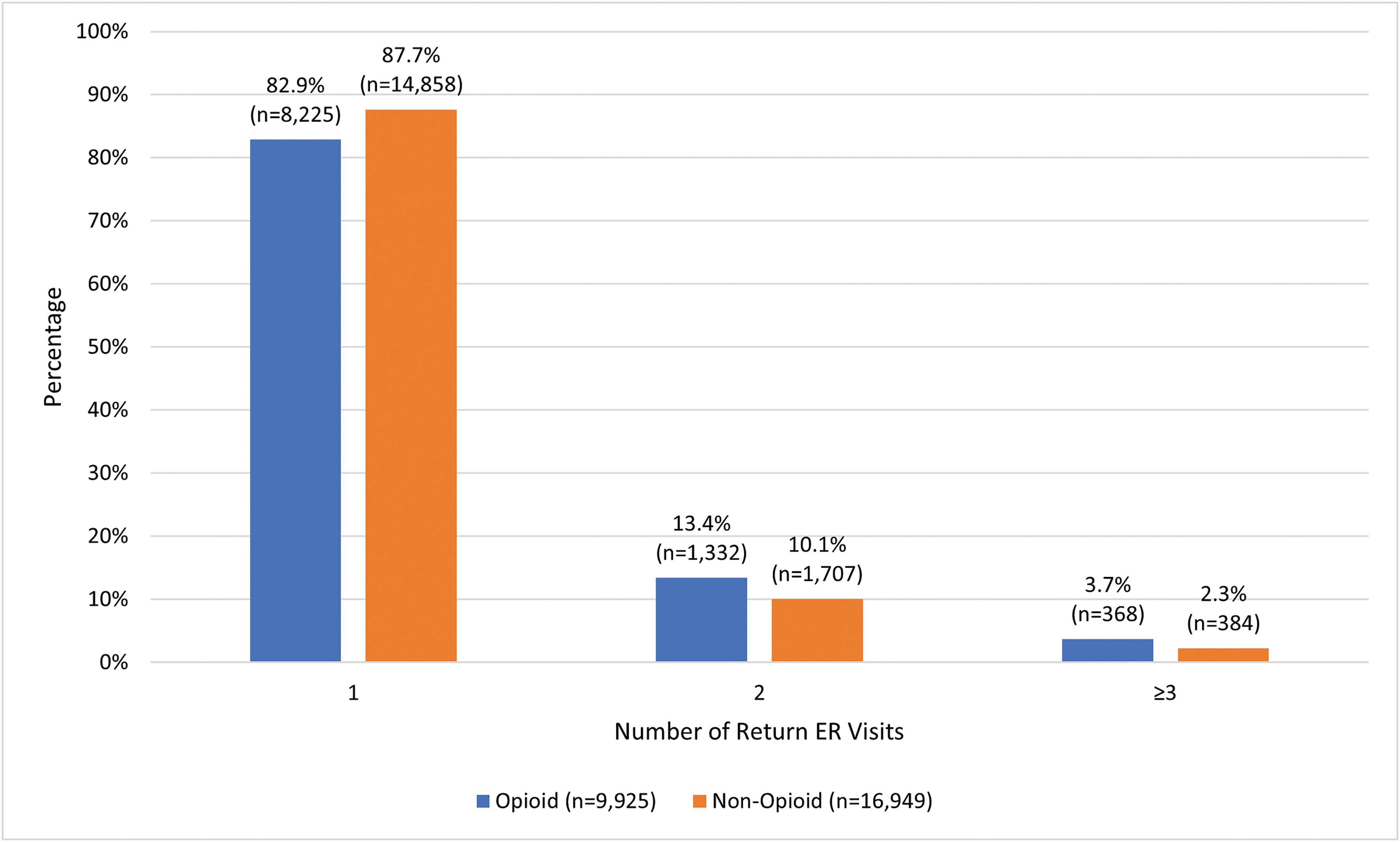
Proportion of patients with the outcome of a return ER visit within 14 days in the exploratory cohort, stratified by the number of return visits. Patients with zero return visits were not included in this calculation. The values listed above each bar represent the number of patients in that group. ER = emergency room. Color images are available online.
Risk Ratios of a Return Emergency Room Visit Within 14 days and of Persistent Opioid Use ≥6 Months Among Patients in the [A] Exploratory Cohort and [B] Validation Cohort
CI = confidence interval; ER = emergency room; RR = risk ratio.
A total of 116,372 patients (45.6%) were noted to have an active prescription for opioids ≥6 months from the index ER visit. Among this cohort, oral opioids were prescribed at the index ER visit in 41,430 patients, whereas the remaining 74,942 did not initially receive oral opioids. Administration of oral opioids at the index visit was thus associated with an increased risk of persistent opioid use on unmatched analysis (RR 1.32, 95% CI 1.31–1.33, p < 0.001) (“A” in Table 2).
Propensity score matching yielded 68,640 patients in each group, for a total of 137,280 patients (“B” in Table 1). Statistically significant differences remained between the groups with respect to gender and race, but the disparity was narrowed considerably after matching. Statistical balance was achieved on age and several key comorbidities, including a history of anxiety, chronic pain, substance abuse, and urolithiasis. Although patients with a history of opioid use still received oral opioids at a higher rate than those without, the difference between the two groups narrowed from 20.2% before matching to 1.5% after matching.
Upon matching, the risk of a return ER visit within 14 days was 25% higher (RR 1.25, 95% CI 1.22–1.29, p < 0.001) and the risk of persistent opioid use was 12% higher (RR 1.12, 95% CI 1.11–1.14, p < 0.001), among those who received oral opioids at the index visit compared with those who did not (“A” in Table 2). Matched analysis, therefore, exhibits the same associations as the unmatched analysis, although at an attenuated rate.
Validation cohort
There were 2,112,324 patients in the TriNetX Diamond Network who met the inclusion criteria, of whom 396,373 (18.8%) were prescribed oral opioids (“A” in Table 3). The differences between the opioid and nonopioid groups were similar to that seen in the exploratory cohort, as patients who were prescribed oral opioids had higher rates of medical comorbidities, ER utilization, prior urologic surgeries, and analgesic medication use. Notably, the distribution of race was such that the majority were of an unknown race. Nevertheless, White patients still received oral opioids at a significantly higher proportion than all other races.
Clinicodemographic Characteristics of the Validation Cohort, Stratified by Administration of Oral Opioids at the Index Emergency Room Visit
A total of 254,204 patients (12.0%) had a return visit to the ER, of whom 65,171 were prescribed oral opioids and 189,033 were not prescribed oral opioids at the index ER visit. On unmatched analysis, patients prescribed oral opioids had a 49% increased risk of a return ER visit (RR 1.49, 95% CI 1.48–1.51, p < 0.001) (“B” in Table 2). As seen in the exploratory cohort, among individuals with a return visit, those prescribed opioids were more likely to have multiple visits compared with those not prescribed opioids (1.30 return visits vs 1.16 return visits, p < 0.001) (Supplementary Fig. S1).
There were 692,081 patients (32.8%) who filled an oral opioid prescription ≥6 months from the index ER visit. Opioids were provided at the index ER visit in 196,036 patients, and the remaining 496,045 did not initially receive oral opioids. Administration of oral opioids at the index visit was thus associated with a 71% increased risk of persistent opioid use on unmatched analysis (RR 1.71, 95% CI 1.70–1.72, p < 0.001) (“B” in Table 2).
Propensity score matching yielded a total of 715,620 patients, with 357,810 patients in each group (“B” in Table 3). Using the same variables as the exploratory cohort for matching, statistical balance was achieved only with respect to age and a prior history of urolithiasis. Still, the differences in proportions were narrowed between the two groups across all variables.
Matched analysis of the validation cohort demonstrated results that reflected the exploratory cohort. Administration of oral opioids was associated with a 28% increased risk (RR 1.28, 95% CI 1.27–1.30, p < 0.001) and 37% increased risk (RR 1.37, 95% CI 1.36–1.38, p < 0.001) of return ER visit within 14 days and persistent opioid use ≥6 months, respectively (“B” in Table 2).
Discussion
In this population-based study of >2 million patients treated in the ER for urolithiasis, opioid prescriptions were associated with an increased risk of a return ER visit. In addition, and perhaps not surprisingly, the administration of opioids increased the risk of persistent opioid use. Indeed, these findings raise great concerns with regard to opioid misuse, addiction, and abuse.
The finding that patients receiving opioids for renal colic had a higher rate of return ER visits within 14 days was confirmed in our validation cohort. To our knowledge, this is only the second study to examine the association of opioid use with return ER visits in this setting. Minhaj et al. performed a single-center retrospective uncontrolled study of the impact of a multimodal analgesic regimen for renal colic in the ER. 8 The multimodal pain algorithm resulted in a mild decrease in opioid use (63% vs 71%), whereas slightly increasing the rate of return ER visit within 7 days (11% vs 7%).
However, given the study design and the high rate of crossover—only 6% of the study population adhered to the assigned treatment—these findings may not accurately portray the impact of opioids. In our study, the higher rate of return ER visits is likely caused by one of two factors: (1) opioids provided inferior analgesic control, necessitating additional emergency care, or (2) the adverse effects of opioids pushed patients to seek urgent treatment unrelated to the symptoms of urolithiasis. A previous study points to analgesic inadequacy as the cause of return ER visits, concluding that opioids increase the risk of persistent pain in ER patients with urolithiasis. 9 Those results showed an increased pain level with opioid use as far out as 90 days after the index ER visit, possibly alluding to a hyperalgesic effect of opioids. Furthermore, there was a possible dose–response relationship, with greater doses of opioids leading to increased rates of persistent pain.
The analgesic properties of opioids for renal colic are also addressed in a meta-analysis comparing the efficacy and safety of opioids, NSAIDs, and paracetamol for renal colic in the inpatient setting. In that review, NSAIDs provided superior pain control at 30 minutes with the fewest adverse effects, particularly vomiting. 3 Consistent with these findings, the EAU advises that nonopioid analgesics such as NSAIDs and acetaminophen/paracetamol be used as first-line therapy for acute renal colic, with opioids remaining as a second-line option. 6 That being said, there are certainly exceptions in which these nonopioid analgesics cannot or should not be used, such as in the case of allergies or renal insufficiency. Nevertheless, for most patients, opioids should have a more limited role in the treatment for acute renal colic. Although further investigation is needed, it may be prudent to utilize renal decompression and/or stone removal as second-line therapy over opioids.
The current results revealed that opioid prescription in the ER setting also increased the risk of persistent opioid use 6 months later. Several studies have demonstrated this same relationship, showing a 9% to 14% increased risk of persistent opioid use depending on whether the opioids were administered for trial of passage or in the postoperative setting. 9 –11 Our rate of persistent opioid use was higher than in other studies (32%–45%), which is likely related to the methodology of data extraction from diagnosis codes and limited exclusion criteria. As such, this likely overestimates the true rate of persistent opioid use because of the index ER visit.
However, the implications of this finding remain significant. Every year, >1 million ER visits in the United States are related to the abuse of pharmaceuticals. 12 Furthermore, the number of drug overdose deaths has quadrupled for the past two decades, with opioid-related deaths highest among persons aged 35 to 54 years. Patients in this age range are vulnerable to urolithiasis, with a prevalence as high as 14%, and our findings confirmed the association of younger age with opioid administration. 13,14 In addition, women have been shown to have a slightly higher risk of long-term opioid use after an acute pain event. 15 Thus, it is imperative that clinicians minimize the use of opioids in acute renal colic.
In contrast, our findings regarding the frequency of opioid prescriptions for renal colic can be seen as encouraging. We found a 19% and 29% incidence of administration in the exploratory and validation cohorts, respectively, which was lower than previously reported rates of 49% to 59%. 16,17 This may be a sign that opioid reduction initiatives are effective. The fact that the exploratory cohort, which comprised primarily academic facilities, had an opioid administration rate that was 10% lower than the validation cohort, which is more representative of the broader community, could be reflective of educational processes (i.e., residency training) informing contemporary clinical care.
Many hospital systems have changed ER pain management processes in the hope of reducing opioid prescriptions. 8,18 –20 Furthermore, there has been a wave of opioid-free Enhanced Recovery After Surgery pathways for renal colic after kidney stone surgery. 21 –24 These studies demonstrated that omitting opioids from the analgesic regimen did not have a negative impact on postoperative pain. The urologic community must remain vigilant in these efforts, as nephrolithiasis is a known risk factor for long-term opioid use. 25
Limitations of our study include the retrospective nature and reliance on the accuracy of diagnosis codes and claims data. In addition, owing to the limitation of the database, return ER visits may be because of causes other than urolithiasis, resulting in an overestimation of this parameter. However, it is theorized that a secondary ER trip within 14 days of the index visit is highly likely to be related to urolithiasis. Furthermore, the quantity of opioids administered could not be examined and is a limiting factor, as the return visit could have been caused by an inadequate supply of analgesics. Finally, the definition of persistent opioid use as filling of an opioid prescription after 6 months does not equate to dependence or addiction, nor does it indicate that additional opioid use was related to urolithiasis. However, it does provide a good metric as a risk factor for future opioid-related problems.
Conclusions
We find that a significant proportion of patients presenting to the ER with renal colic are discharged with opioids. This confers an increased risk of a return ER visit as well as persistent opioid use. This study adds to the growing body of evidence that opioids should not be first-line therapy for acute renal colic. Future efforts should be directed at understanding patient and physician factors that may be driving this prescription rate to identify action items to reduce opioid use.
Footnotes
Authors' Contributions
Conceptualization, methodology, formal analysis, data curation, and writing—original draft by R.A. Methodology, formal analysis, and writing—review and editing by R.E.N.B. Methodology, formal analysis, writing—review and editing, and supervision by J.S.W. and B.R.M. Conceptualization, methodology, formal analysis, writing—original draft, and supervision by E.G.K.
Author Disclosure Statement
B.R.M. is a consultant for the Boston Scientific Corporation, outside the scope of this research. All other authors declare that they have no conflicts of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.