
Abstract
Introduction and Objectives:
Mini-percutaneous nephrolithotomy (PCNL) has gained popularity over the last decade due to its stone-free rate comparable to traditional PCNL but with decreased risk of complications. While the data on mini-PCNL has been favorable thus far, no study today has evaluated outcomes in obese patients.
Methods:
All patients undergoing mini-PCNL at our institution since we began its use in 2019 were included in this study. Mini-PCNL was defined as access sheath ≤22F in size. An obese group with body mass index (BMI) ≥30 was compared to a nonobese group with BMI <30. A patient was considered relatively stone free if residual fragments were <4 mm on follow-up CT with ≤3 mm cuts. Fisher exact test was used to compare dichotomous differences between variables, and t-test to compare continuous variables.
Results:
We identified 67 patients who underwent mini-PCNL during the study period with 33 patients in the obese group. Median BMI in the obese group was 36.4 kg/m2 compared to 25.05 kg/m2 in nonobese. There were no blood transfusions in either group during the study period. There was no statistical difference between the obese vs nonobese group for age, access sheath size, change in hemoglobin, same day discharge, percent relatively stone free, emergency department visit within 30 days, and median largest single stone diameter. There was a significant difference in the sum of all treated stone diameter in the obese group (median 15 mm) vs nonobese (median 18 mm, p = 0.02) (Table 1).
Conclusion:
Mini-PCNL appears to be equally safe and effective in obese and nonobese patients alike. While there was a statistically significantly higher amount of overall stone burden in the nonobese groups, the overall difference is not clinically significant. Further research is needed to validate our experience.
Background
Percutaneous nephrolithotomy (PCNL) is the recommended treatment for large kidney stones >2 cm, or lower pole stones >1 cm in size. 1 While the procedure is known for its ability to endoscopically remove large stone burdens, there are some potential complications that limit its use more liberally. These include bleeding (both periprocedurally and delayed), infection, pneumothorax or hydrothorax, and potential for injury to nearby visceral organs. 2 Given these risks, mini-PCNL has gained attraction by offering smaller sheath options, which are believed to minimize trauma to the kidney that may have otherwise occurred with the large sheath sizes of standard PCNL, thereby reducing the number of complications. 3 In addition to its lower complication risk, mini-PCNL achieves similar stone-free rates to standard PCNL 4,5 and greater than that of standard ureteroscopy. 6,7
Given the increasing prevalence of obesity, and it being a known risk factor for kidney stone formation, many patients presenting with kidney stones are obese. 8 –10 PCNL in the obese patient may pose several challenges, including difficulty with positioning and adequate access sheath length owing to increased skin to stone distance. In addition, PCNL in the obese patient may have longer operative times, reduced stone-free rates, and thereby higher retreatment rates than in the nonobese patient. 11,12 Obese patients also carry an increased cardiovascular complications, thromboembolic events, and wound infections. 13,14 Given the challenges and risks involved with PCNL in the obese population, urologists may be hesitant to offer this surgery for the obese patient, particularly when stone size is borderline manageable with ureteroscopy.
While there are established risks of performing standard PCNL in obese patients, the risks and outcomes of mini-PCNL in obese patients have not been described. We hypothesize that when compared to nonobese patients, obese patients will have similar stone-free rates than with mini-PCNL.
Methods
After IRB approved the study (IRB protocol #12081), we identified all patients who underwent mini-PCNL at our institution since we began its use in October 2019 to December 2021. Mini-PCNL was defined as access sheath ≤22F in size. The ©KARL STORZ minimally invasive percutaneous system, Mini-PCNL set was used for these cases which consisted of a single step dilator and access sheath size options of 16F, 17.5F, and 22F. The included rigid nephroscope with a 6F working channel was utilized in these cases. An obese group defined as body mass index (BMI) ≥30, was compared to a nonobese group, defined as BMI <30.
Preoperative CT scans were reviewed and the largest diameter of a kidney stone on any of the three planes (Axial, Transverse, Sagittal) on the side of the mini-PCNL was measured and reported as “largest stone diameter.” When there were multiple stones present on the side of the surgery, the largest diameter of each of the stones was totaled and reported as “sum of all stone diameters” and used as an estimate of total stone burden. A patient was considered relatively stone free (Grade C) if residual fragments were <4 mm on follow-up CT with ≤3 mm cuts performed within 3 months of the original surgery.
Preoperative hemoglobin was compared to a hemoglobin laboratory checked within 24 hours postoperatively and was reported as “hemoglobin decrease.” Fisher exact test was used to compare dichotomous differences between variables and t-test to compare continuous variables.
Results
We identified 67 patients who underwent mini-PCNL during the study period; there were 33 patients in the obese group and 34 patients in the nonobese group. Median BMI in the obese group was 36.4 kg/m2 compared to 25.05 kg/m2 in nonobese. There was no statistical difference between the obese vs nonobese group for age, access sheath size, change in hemoglobin, same day discharge, percent relative stone free, emergency department visit within 30 days, and median largest single-stone diameter (Table 1). In the obese group 51.52% of patients were discharged home the same day, compared to 58.85% in the nonobese group (p = 0.628). Relative stone-free rates were 84.85% in the obese group and 67.67% in the nonobese (p = 0.152), which resulted in secondary procedures (all ureteroscopy) in 12.12% and 20.59%, respectively (p = 0.512).
Patient Characteristics and Outcomes
Values are presented in median (standard deviation) unless otherwise specified.
P values reaching significance (p < 0.05) have been bolded.
BMI = body mass index; ED = emergency department.
Upper pole access was obtained in 18.2% of the cases in the obese group and 29.4% in the nonobese group (p = 0.392), the remainder were lower pole access. Antegrade flexible ureteroscopy was performed in 64.7% of the cases in the obese group and 61.8% of cases in the nonobese group (p = 0.800). Combined antegrade and retrograde ureteroscopy was performed in only one patient overall, otherwise the rigid nephroscope alone was used. Overall, laser lithotripsy with a Lumenis Moses Holmium laser was used in 67% of the cases, Venturi evacuation with or without stone basket extraction was used in 22% of the cases, and LithoClast Trilogy was used in 10% of cases.
There was a significant difference in the sum of all treated stone diameter in the obese group (median 15 mm) vs nonobese (median 18 mm, p = 0.02) (Table 1). There were no significant differences in overall complications or complication type. There were no blood transfusions in either group during the study period. The two Clavien-Dindo grade III complications included a pleural effusion requiring interventional radiology drainage, and an obstructing stone fragment that required ureteral stent placement. The patient with the reported pleural effusion had upper pole access between the 11th and 12th ribs that was obtained by interventional radiology at the surgeon's request due to the existence of an ileal conduit urinary diversion.
Discussion
In this retrospective review, we are the first to demonstrate the safety and efficacy of mini-PCNL in the obese population that included a BMI of up to 53.6 kg/m2. It appears from the data that the recognized lower risk of complications associated with mini-PCNL compared to standard PCNL may outweigh the otherwise higher risks of performing PCNL in the obese patient. There was no observed difference in complication rates between obese and nonobese patients. While there were two grade III complications in the obese group, and none in the nonobese group, this was still too low a rate of occurrence to reach statistical significance. Notably, there were no grade IV or V complications in either group.
In a large multicenter study on over 5803 undergoing PCNL, Fuller and colleagues found that compared to nonobese patients, obese patients had a significantly longer operative time, reduced stone-free rate, and higher retreatment rate. 11 We did not find these outcomes significantly different in our study on mini-PCNL, which is consistent with published standard PCNL outcomes of 1152 patients at our institution showing no difference in case duration, stone-free rate, or secondary procedures among obese and even superobese (BMI >50) patients. 15 It is unclear why the discrepancy in stone-free rates and secondary procedures in both the mini and standard PCNL experience and that reported in the Fuller study as there was no difference in stone size between the groups in all of the studies.
It may be, in part, due to the multicenter nature (96 locations) which included low-volume centers as opposed to the high-volume single-center experience with fellowship trained endourologists, highlighting the impact specialty training in this area can have. Similar to our mini-PCNL findings, both of these studies did not find a significant difference in complication rates or need for transfusion among the obese patients. 11,15
Overall, our mini-PCNL relative stone-free rate outcomes were in line with those in the reported literature. A study by Kokov et al. out of Germany followed 146 patients with CT after mini-PCNL and with a stone-free cutoff of ≤3 mm found rates to be 25% to 50.5% depending on stone size, with the highest rate in patients with 10 to 20 mm of stone burden and a 25% rate for stones >20 mm. 16 Other reports in the literature show stone-free rate following mini-PCNL to vary from 70% to 96%, although stone parameters for undergoing mini-PCNL vary widely and criteria to declare a kidney stone-free range from residual stones of size 2 to 4 mm. 17,18
Our relative stone-free rates of 68% to 85% as confirmed by postoperative CT and a cutoff of <4 mm are therefore within expected for this procedure, and obese patients in our series having a relative stone-free rate of 85% would suggest that obesity was not a limitation.
The only significance between the two groups, apart from BMI, was the sum of all stone diameters (Table 1). Finding that this was lower in the obese group raises the possibility of selection bias against proceeding with mini-PCNL with a low tolerance for allowable stone burden in obese patients. While there was a statistical difference between the two groups, a difference of only 3 mm is of questionable clinical significance and is unlikely to have been a confounding variable behind the otherwise equivalent outcomes of the two groups. Further, using sum of all stone diameters is not a perfect estimate of total stone volume but was selected as a practical surrogate used by many urologists due to its quick reproducibility during consultation visits when decision-making is being performed.
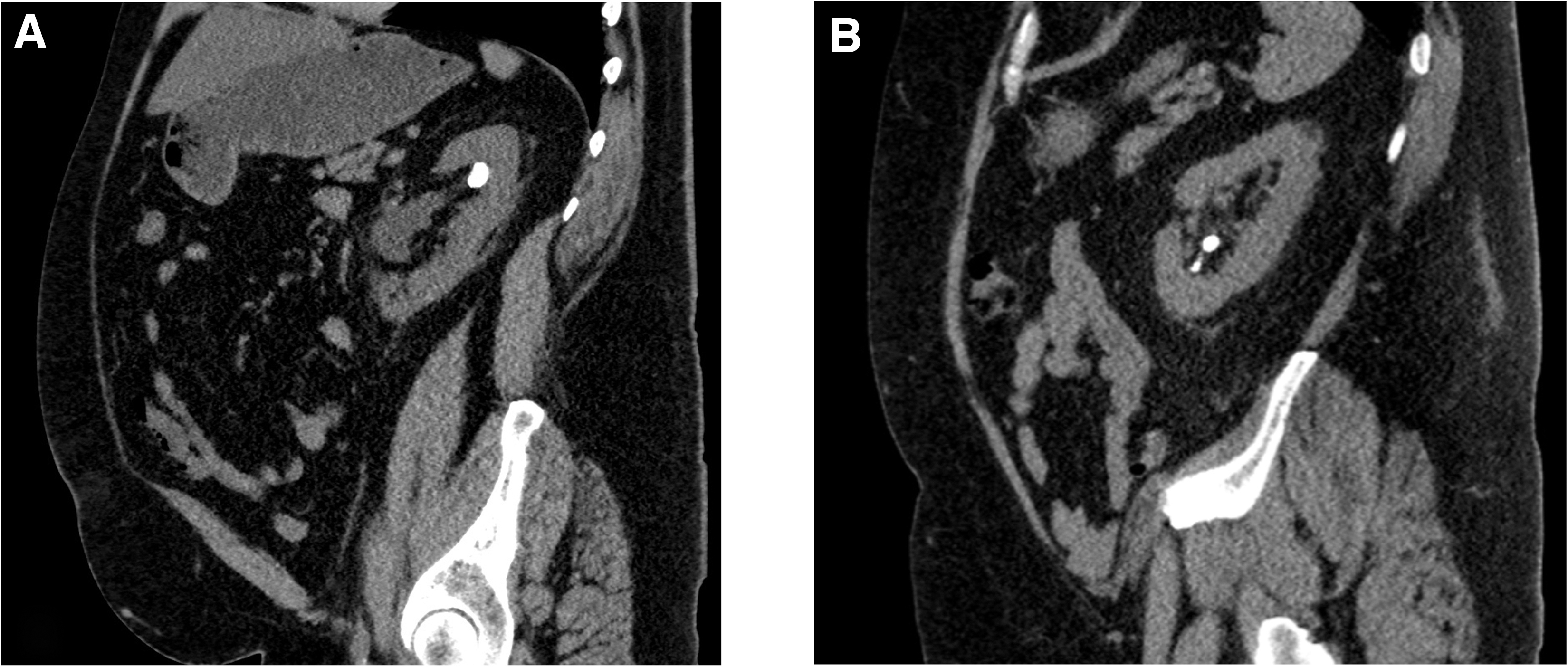
Using the sum of all stone diameters becomes increasingly problematic as quantity of stones rises. As demonstrated in Figure 1, both patients have 1.6 cm of total stone diameters, but patient A has a higher true stone volume than patient B. A single 1.6 cm stone has a volume of 2.14 cm3 and four 4 mm stones while having the same additive total diameter only have a total volume of 0.13 cm3. Such a difference in true stone volume makes the sum of stone diameters an unreliable method for truly comparing the stone burden between the two groups. Unfortunately, total stone volume is not routinely described on imaging reports and is not readily producible at the time of consultation, especially when multiple stones are present.
Therefore, while sum of all stone diameters was selected as the surrogate for stone volume given its widespread use, the statistically significant difference observed between the two study groups, is uncertain to be of clinical significance given its shortcomings in true stone volume estimation. By not representing true stone volume, the offered measurement of largest diameter can also be misleading as oblong or irregularly shaped stones would be overestimated.
While not statistically significant (p = 0.512), there was a lower percentage of patients requiring secondary procedures in the obese group (12.12%) than in the nonobese group (20.59%), which would be in line with the lower sum of all stone diameters noted in the obese group. It is worth noting that the rates of secondary procedures in either group is much lower than published secondary procedure rates following unilateral standard PCNL at our institution, which was shown to be 44%. 19 The lower relative reoperation rate we have experienced is felt to be due to lessened stone size and complexity that are offered mini-PCNL rather than any intrinsic superiority, but does highlight mini-PCNL capabilities in the appropriately selected patient.
There are notable limitations to this study. First is the retrospective nature of the design, although without the ability to randomize patients to either the obese or nonobese group, and there would be a limited benefit to a prospective study. Second, there is uncontrolled bias for who is felt to be a candidate for a mini-PCNL, and there is a subjective assessment based on body habitus, stone volume, and stone location that determines who is offered this procedure. It is possible that there were more selective criteria applied subconsciously to the obese patients that resulted in there being otherwise equivalent outcomes between the two groups. Future work on this subject would benefit from structured criteria for assigning patients to undergo traditional vs mini PCNL in an effort to control for this otherwise biased selection.
Conclusion
Mini-PCNL is a safe and effective treatment option for the appropriately selected obese and nonobese patients alike. Although there are shortcomings to estimations of stone volume, our outcomes were seen with an average overall total stone burden of 18.6 mm, which was associated with high relative stone-free rates and low secondary procedure rates in both groups. The ideal mini-PCNL candidate remains to be defined; obesity does not appear to be a limitation. Future work should focus on accurate stone volumetric estimation and how this and other stone parameters correlate with mini-PCNL outcomes.
Footnotes
Acknowledgment
The abstract to this study was previously published in Abstracts of the 39th World Congress of Endourology: WCE 2022.
Authors' Contributions
A.S. performed chart review to collect data, performed the statistical analysis, and primarily authored the abstract and the article. M.R. devised the project, reviewed the protocol, interpreted the data, and reviewed and edited the abstract and the article. T.L. was involved in study design, data interpretation, and article review. E.S. produced list of patients meeting inclusion criteria, was involved in chart review and data collection, and reviewed the abstract/article.
Author Disclosure Statement
Dr. Marcelino Rivera is a consultant for Boston Scientific Corporation and Cook Medical. Dr. Tim Large is a consultant for Boston Scientific Corporation and Lumenis. Dr. Austen Slade is a consultant for Cook Medical.
Funding Information
No funding was received for this article.