
Abstract
Introduction:
Outcomes after ultrasound-only percutaneous nephrolithotomy (PCNL), in which no fluoroscopy is used, are not well known. The goal of this study was to compare outcomes of ultrasound-only and fluoroscopy-directed PCNL.
Materials and Methods:
Prospectively collected data from the Registry for Stones of the Kidney and Ureter database were reviewed for all patients who underwent PCNL at one academic center from 2015 to 2021. Primary outcomes were complications and stone-free rates (no residual fragments ≥3 mm).
Results:
Of the 141 patients who underwent ultrasound-only PCNL and 147 who underwent fluoroscopy-directed PCNL, there was no difference in complication rates (15% vs 16%, p = 0.87) or stone-free status (71% vs 65%, p = 0.72), respectively. After adjusting for body mass index, American Society of Anesthesiologists (ASA), stone size, and stone complexity by Guy score, ultrasound-only PCNL was not associated with any increased odds of complications (odds ratio [OR] 0.7, 95% confidence interval [CI] 0.3–1.6, p = 0.41) or residual stone fragments ≥3 mm (OR 1.0, 95% CI 0.5–1.9, p = 0.972) compared with fluoroscopy-directed PCNL. Ultrasound-only PCNL was associated with shorter operative time (median 99.5 vs 126 minutes, p < 0.001), and the use of ultrasound remained a significant predictor of short operative time (<100 minutes) after controlling for supine positioning, stone size, and stone complexity by Guy score (OR 2.31, 95% CI 1.01–5.29, p = 0.048). Patients in the ultrasound-only group were spared a mean radiation exposure dose of 10 mGy per procedure.
Conclusions:
Ultrasound-only PCNL is safe and achieves similar stone-free rates compared with fluoroscopy-directed PCNL with the added benefit of avoidance of radiation.
Introduction
Percutaneous nephrolithotomy (PCNL) is the standard minimally invasive surgical procedure for removal of kidney stones >2 cm. 1 More recently, the use of ultrasound for renal access has been gaining popularity. A systematic review including six randomized controlled trials, three case–control trials, and three meta-analyses found similar outcomes for ultrasound-guided renal access compared with fluoroscopic-guided renal access during PCNL. 2 Benefits of ultrasound-guided renal access include decreased radiation, decreased cost, and decreased learning curve compared with fluoroscopic-guided renal access. 3 –5
While the use of ultrasound for gaining renal access is gaining more widespread acceptance, the use of ultrasound for all steps of PCNL is less common. In cases in which ultrasound is used for gaining access, fluoroscopy is still commonly used for retrograde pyelogram (for access planning), tract dilation, stent/nephrostomy tube placement, and/or to check for residual stones at the end of the case. This necessitates access to fluoroscopy, which may not be as readily available compared with ultrasound at all sites. Switching from ultrasound to fluoroscopy during PCNL can also be cumbersome and add to operative time. Our group has previously shown that ultrasound-guided tract dilation can be safely performed with similar complication and stone-free rates to fluoroscopic-guided dilation. 6
However, in this cohort, fluoroscopy was still frequently used for retrograde pyelogram (for access planning), stent/nephrostomy tube placement, and/or to check for residual stones at the end of the case. At our center, forgoing fluoroscopic-guided placement of nephrostomy tube/stents and use of fluoroscopy to check for residual stones represented the final step in achieving ultrasound-only PCNL. However, it remains to be seen whether stone-free rates and complications (in particular related to stent/nephrostomy tube placement) were acceptable when these steps were omitted. The objective of this study was to evaluate stone-free rates and complication rates in those who underwent ultrasound-only compared with fluoroscopy-directed PCNL at one high-volume tertiary care center.
Materials and Methods
Study design
This was a retrospective review of prospectively collected data from the Registry for Stones of the Kidney and Ureter (ReSKU) database on all patients who underwent PCNL at one academic center from 2015 to 2021 at the University of California, San Francisco Helen Diller Medical Center, a tertiary referral center for stone disease. We obtained institutional review board approval and patient written consent to prospectively collect demographic and clinical data (CHR no. 14-4533). 7 Patients were divided into two groups: ultrasound-only (in which no amount of fluoroscopy was used) and fluoroscopy-directed (in which fluoroscopy was used for any portion of the case).
Surgical technique
Our surgical technique for ultrasound-guided PCNL access and tract dilation has been described previously. 8,9 In brief, an externalized ureteral stent was placed into the ipsilateral ureter via a flexible cystoscope for retrograde saline injection to induce caliceal dilation. Patients were positioned prone or in a modified supine lithotomy position as described in the literature. 10 A 3.5 MHz range curved array ultrasound transducer (Hitachi Aloka Medical America, Wallingford, CT) was used to visualize the renal parenchyma, pelvicaliceal system, stones, and surrounding organs. An 18-gauge echogenic needle (Cook Medical) was advanced into the target calyx under ultrasound guidance. The needle stylet was removed, and either an extra stiff wire (mini-PCNL) or a J-tip coaxial guidewire (regular PCNL) was inserted into the renal pelvis under ultrasound guidance.
The needle was removed, and a 1-cm skin incision was created surrounding the guidewire. Tract dilation proceeded with fluoroscopic guidance or ultrasound guidance. The tract was dilated first using a 10F fascial dilator (Cook Medical), followed by either a 16F Clearpetra sheath (mini-PCNL; Micro-Tech Endoscopy USA, Ann Arbor, MI) or 24–30F high-pressure balloon dilator and sheath (regular PCNL; BARD X-Force, Bard Medical). Ultrasound attempts at dilation were abandoned in favor of fluoroscopy if at any point ultrasound visualization of the kidney or access instrumentation was felt to be poor enough to be unsafe to proceed by the operating surgeon. An offset rigid nephroscope and lithotripter was used for stone fragmentation and removal. In the ultrasound-only technique, the presence of remaining stone fragments was determined by ultrasound imaging or direct visualization using a nephroscope, antegrade flexible cystoscope, or ureteroscope at the end of the case.
In fluoroscopic-directed PCNL, fluoroscopy was used to determine the presence of remaining stone fragments in addition to direct visualization. Kidney drainage was achieved using a 10F antegrade nephrostomy tube, ureteric stent, or occasionally no stent or nephrostomy tube. For nephrostomy tube placement without fluoroscopy, the nephrostomy tube was placed through the access sheath, saline was injected through the nephrostomy tube to create bubbles and confirm proper location in the renal pelvis under ultrasound, and the sheath was then cut away leaving the nephrostomy tube in place.
Data acquisition
Demographic, perioperative, and primary outcomes were collected as part of ReSKU. Demographic characteristics included age, gender, and body mass index (BMI). Perioperative data included preoperative stone size, procedure laterality, surgical position, calix puncture location, number of tracts dilated, and operative time. Primary outcomes of interest were complications and stone-free status. Complications were defined using the Clavien–Dindo classification system. 10 Stone-free status was defined as no residual fragments ≥3 mm on postoperative imaging, including plain radiographs, renal ultrasound, or CT scan of the abdomen, at the first clinical visit within 90 days of the operation. Patients without postoperative imaging were excluded from the analysis. Patients scheduled for future second-stage procedures were categorized as not stone free.
Statistics
Descriptive statistics were used for baseline characteristics and outcome data. Continuous baseline variables were checked for normality. A two-sided Student's t-test was used for normally distributed continuous data. Fisher's exact test was used for categorical data. Univariate and multivariable logistic regression analyses were performed. Data were analyzed using R (R Core Team; Vienna, Austria).
Results
Of 443 patients initially identified who underwent PCNL, 155 were excluded as they did not have any follow-up imaging available (Fig. 1). Of the remaining 288 patients, 141 (49%) underwent ultrasound-only PCNL and 147 (51%) underwent fluoroscopy-directed PCNL. In the fluoroscopy-directed PCNL group, access was achieved by ultrasound in 75 (51%) cases, fluoroscopy in 37 (25%) cases, and a combination of ultrasound and fluoroscopy in 35 (24%) cases. In the fluoroscopy-directed group, ultrasound was used for both the puncture and dilation in 32 (22%) patients. In cases in which ultrasound was used for both puncture and dilation, reasons for use of adjunct fluoroscopy were to aid nephrostomy tube placement (66%), check for residual stones (47%), and to perform retrograde pyelogram (31%).
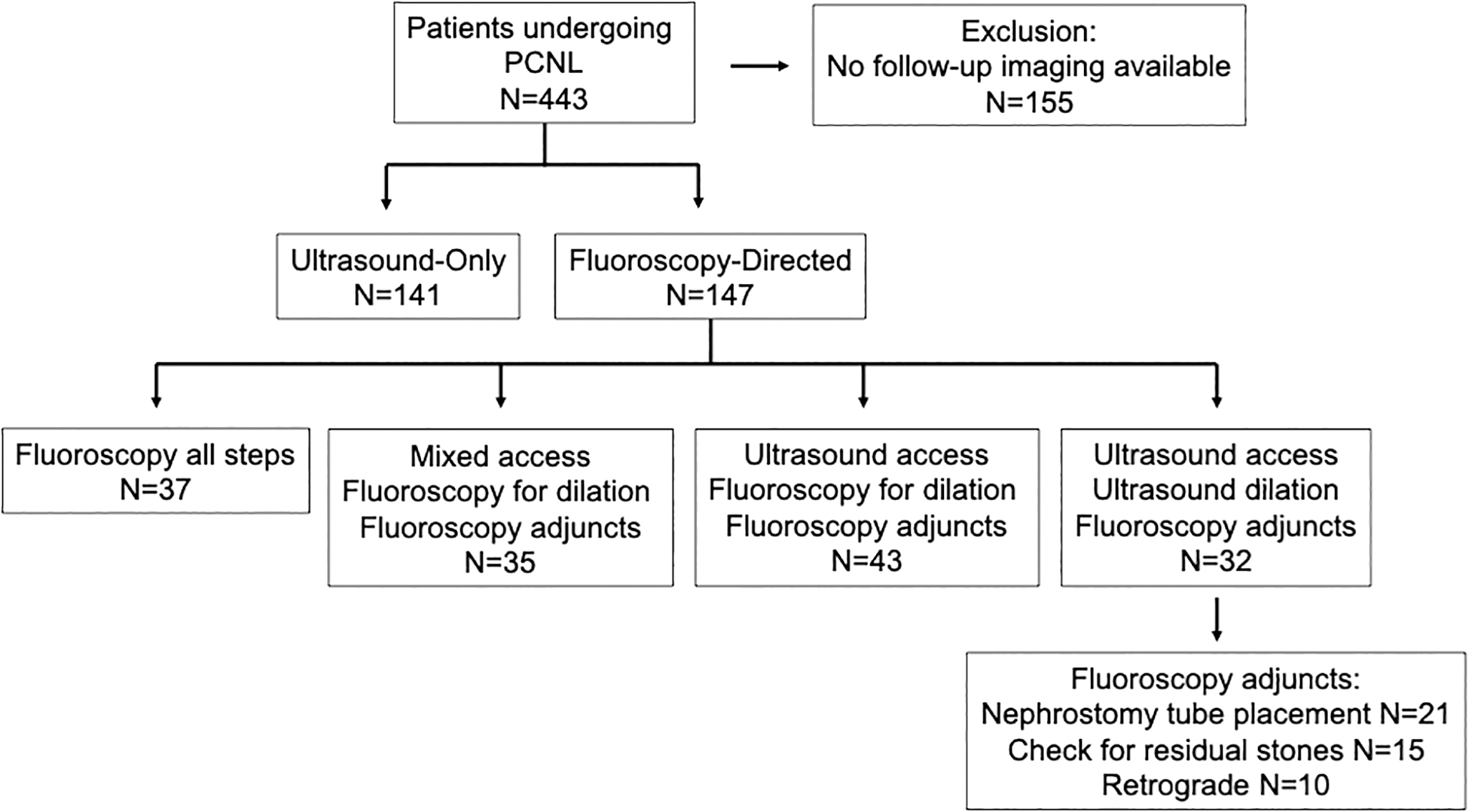
Patient flow diagram showing the use of fluoroscopy during certain steps of PCNL cases. Fluoroscopy adjuncts included fluoroscopy used for retrograde pyelogram, nephrostomy tube placement/stent placement, and to check for residual stone fragments. PCNL = percutaneous nephrolithotomy.
The mean maximum summative stone diameter was 30 mm, and 44% were Guy score 3 or 4. Stone and patient characteristics were similar between both groups (Table 1). Ultrasound-only PCNL was associated with shorter operative time (median 99.5 vs 126 minutes, p < 0.001), higher success rate of access achieved by resident (38.3% vs 16.3%, p < 0.001), and more frequent use of supine positioning (69% vs 25%, p < 0.001) compared with fluoroscopy-directed PCNL (Table 1). In the fluoroscopic-guided group, the mean radiation exposure dose was 10 mGy per procedure.
Baseline and Perioperative Characteristics of Patients who Underwent Ultrasound-Only vs Fluoroscopy-Directed Percutaneous Nephrolithotomy
ASA = American Society of Anesthesiologists; BMI = body mass index; IQR = interquartile range.
The overall complication rate was 18%, of which 79% were Clavien–Dindo grade 1 or 2 (Table 2). There was no difference in complication rates (15% vs 16%, p = 0.87) or stone-free status (71% vs 65%, p = 0.72) between those who underwent ultrasound-only PCNL and fluoroscopy-directed PCNL, respectively (Table 2). There was no difference in complications related to nephrostomy/stent malposition, with 2 (1.4%) nephrostomy tube dislodgements occurring in the ultrasound-only group and 1 (0.7%) in the fluoroscopy-directed group. Ultrasound-only PCNL was associated with a lower percent drop in hematocrit compared with fluoroscopic-directed PCNL (2.7% vs 4.9%, p = 0.02; Table 2).
Postoperative Outcomes of Ultrasound-Only vs Fluoroscopy-Directed Percutaneous Nephrolithotomy
UTI = urinary tract infection.
After adjusting for BMI, American Society of Anesthesiologists (ASA), stone size, and stone complexity by Guy score, ultrasound-only PCNL was not associated with any increased odds of complications (odds ratio [OR] 0.7, 95% confidence interval [CI] 0.3–1.6, p = 0.41) or residual stone fragment ≥3 mm (OR 1.0, 95% CI 0.5–1.9, p = 0.97) compared with fluoroscopy-directed PCNL (Tables 3 and 4). BMI >40 (OR 10.1, 95% CI 2.8–36.4, p < 0.001) and need for multiple punctures (OR 5.8, 95% CI 1.4–23.5, p = 0.013) were associated with increased odds of complications (Table 3). Stone size >4 cm was associated with decreased odds of complications (OR 0.247, 95% CI 0.07–0.8, p = 0.02; Table 3). Upper pole access was associated with decreased odds of residual stone fragments (OR 0.3, 95% CI 0.2–0.8, p = 0.016; Table 4).
Multivariable Analysis for Complications Within 6 Weeks of Surgery (n = 288)
CI = confidence interval; OR = odds ratio; US = ultrasound.
Multivariable Analysis for Residual Stone Fragments 3 mm or Larger on Imaging at 4–6 Weeks After Surgery (n = 288)
A sensitivity analysis examining factors affecting short operative time (<100 minutes) showed that ultrasound-only technique was significantly associated with short operative time after controlling for supine positioning, stone size, and stone complexity by Guy score (OR 2.31, 95% CI 1.01–5.29, p = 0.048, Table 5).
Multivariable Analysis for Short Operative Time (<100 Minutes) (n = 288)
Surgeon's reasons for the use of fluoroscopy in addition to ultrasound were explored. The most common reason for utilizing fluoroscopy in addition to ultrasound was that the primary surgeons were still gaining comfort with utilizing ultrasound for each step (puncture, dilation, nephrostomy tube/stent placement, and/or to check for residual stones) at 53%. Case complexity was a factor in 38% of cases. In 9% of cases, no clear reason for use of fluoroscopy was documented.
Discussion
The use of ultrasound guidance for PCNL access has gained popularity. However, reports on ultrasound-only PCNL, in which ultrasound is used for all steps of the procedure, are limited as fluoroscopy is often used for dilation to aid stent/nephrostomy tube placement and to check for residual stone fragments. We have previously reported on our technique for transitioning to ultrasound-guided PCNL. 5 We recommend a stepwise progression of (1) successful imaging and interpretation of renal anatomy with ultrasound, (2) ultrasound-guided puncture, (3) ultrasound-guided dilation, and (4) elimination of fluoroscopy adjuncts (retrograde pyelogram, nephrostomy tube/stent placement, looking for residual stone fragments).
Our group has previously shown that ultrasound-guided tract dilation can be safely performed with similar complication and stone-free rates to fluoroscopic-guided dilatation. 6 However, fluoroscopy was still frequently used for retrograde pyelogram (access site planning), stent/nephrostomy tube placement, and/or to check for residual stones at the end of the case. In this retrospective review of prospectively collected data for 288 patients, we extend upon our previous findings by showing that ultrasound-only PCNL is safe and achieves similar stone-free rates compared with fluoroscopy-directed PCNL with the added benefit of avoidance of radiation.
Our complication rate of 18% is similar to the complication rate of 21% observed in the Clinical Research Office of the Endourological Society (CROES) global study of 5803 patients who underwent PCNL. 11 Most (79%) complications were Clavien–Dindo grade 1–2. In a systematic review of six randomized controlled trials, three case–control studies, and three meta-analyses of 8705 patients, there was no difference seen in complications after access achieved using ultrasound compared with fluoroscopy. 2 However, this systematic review was limited to studies examining the use of ultrasound for access only, not the remaining portions of the case including tract dilation and tube insertion, which can be more technically difficult under ultrasound guidance.
We found that the use of ultrasound for all portions of the PCNL procedure was associated with similar complication rates compared with PCNL utilizing fluoroscopy. Importantly, there was no difference in complications related to nephrostomy/stent malposition in the ultrasound-only group. To aid placement of nephrostomy tube under ultrasound, our technique was to place the nephrostomy tube through the access sheath, inject saline through the nephrostomy tube to create bubbles and confirm proper location in the renal pelvis, then cut away the sheath around the nephrostomy tube. These results support the use of ultrasound-only PCNL in experienced user's hands.
In our previous reports on ultrasound-guided PCNL for access and dilation, fluoroscopy was often still used for retrograde pyelogram (to aid puncture site planning) and to check for residual stone fragments. By foregoing these steps under fluoroscopy, stone-free rates could theoretically be worse if the access site did not provide optimal trajectory for stone clearance or small fragments were missed using ultrasound. Arguing against this, stone-free rates were not different between ultrasound-only and fluoroscopic-guided PCNL in the current study. Our stone-free rates were somewhat low at 68%. When we removed patients with known residual stones who were planned for second-stage procedure, our stone-free rate increased to 92%, which is favorable compared with 76% in the CROES study. 11
In the ultrasound-only group, we used a combination of ultrasound and direct visualization with rigid nephroscope, flexible cystoscope, or flexible ureteroscope to check for residual stones at the end of the case. In fluoroscopic-directed PCNL, fluoroscopy was used to determine the presence of remaining stone fragments in addition to direct visualization. These results indicate that fluoroscopic imaging of the kidney to check for stone fragments can safely be omitted, thereby saving operative time, decreasing unnecessary radiation, and expanding access to PCNL to include sites without fluoroscopic capability.
Switching from ultrasound to fluoroscopy can be time consuming and fluoroscopy may not always be available at each hospital site. Indeed, we found that operative time for patients in the ultrasound-only group was 27 minutes shorter on average compared with the fluoroscopy-directed group. Supine positioning was more common in the ultrasound-only group, which may have contributed to shorter operative time in this group. In a sensitivity analysis examining factors associated with short operative time, ultrasound-only technique remained significantly associated with short operative time (<100 minutes) after controlling for supine positioning. There is evidence that access using ultrasound can be achieved more quickly than with fluoroscopy, which may partly account for the decreased operative time in the ultrasound-only group. 12 –14
Advantages of ultrasound-only PCNL over fluoroscopic-guided PCNL include avoidance of radiation and ergonomic benefits of avoiding need for lead gowns. In the fluoroscopic-guided group, the mean radiation exposure dose was 10 mGy per procedure. This is consistent with other studies and is roughly equivalent to one CT abdominal scan. 15 Although this is less than the recommended annual limit of 50 mGy/year, stone patients receive frequent imaging for work-up in addition to radiation during stone surgery and the cumulative dose may exceed the annual limit of 50 mGy/year. 16 In one study, 26% and 6% of referred patients already had >20 and >50 mGy radiation exposure, respectively, before being seen by a urologist. 17
The cumulative exposure of urologists and operating room staff to radiation can also be concerning. There are observational data of increased risk of cataracts and brain malignancy among interventional cardiologists who have a high occupational exposure to radiation similar to urologists. 18,19 Ultrasound-only PCNL offers ergonomic advantages over fluoroscopic-guided PCNL by avoiding the need for operating room staff to wear lead. This is important as higher rates of spine problems have been reported in procedural-based specialists who require frequent use of lead compared with nonprocedural specialists. 20 The rate of spine problems correlated with procedural caseload and number of years in practice. 20
Our study has important limitations to consider. First, the decision to conduct dilations, tube insertion, and check for residual stone fragments with fluoroscopic or ultrasound guidance is not necessarily stochastic. Our surgeons have gained expertise with ultrasound and often successfully complete all aspects of the procedure without switching over to fluoroscopy. However, fluoroscopy is always available as a backup if any part of the procedure proves difficult with ultrasound. It is therefore possible that the fluoroscopic-guided group was enriched for increased complexity, and therefore, a higher complication rate and lower stone-free rate might inherently be expected in this group.
Arguing against this, stone complexity as measured by Guy score and stone size was not different between groups. To further rule out selection bias masking a possible difference in outcomes between ultrasound-only and fluoroscopic-guided groups, we performed an intention-to-treat analysis in which those who had puncture initially attempted with ultrasound but required conversion to fluoroscopy were counted in the ultrasound-only group. No difference was seen in complications or stone-free rates with this intention-to-treat analysis (data not shown). Nevertheless, we hesitate to place too much weight on our findings of less blood loss, and increased trainee success with access in the ultrasound-only PCNL group given the possibility of selection bias contributing to these findings. Strengths of our study were the large sample size and prospective collection of data.
Conclusions
Ultrasound-only PCNL is safe and achieves similar stone-free rates compared with fluoroscopy-directed PCNL with added benefits of avoidance of radiation and possibly shorter operative time.
Footnotes
Authors' Contributions
Data collection, data analysis, article writing, and revision by G.W.H. Data analysis and article revision by N.H., F.H., X.C, L.C., H.Y., C.C., K.C., R.U., and W.S. Data collection, review data analysis, and review by D.B.B. and M.L.S. Supervision of the entire project by T.C.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
For David B. Bayne K12DK111028 grant was a source of funding.