
Abstract
Objective:
To investigate the efficacy of ureteral tailoring with or without ureteral bladder reimplantation in the treatment of primary megaureter (MGU) in children by transvesicoscopic ureteral reimplantation.
Methods:
Clinical data from 21 children with primary MGU who were treated with pneumo-bladder ureterovesical reimplantation in Anhui Children's Hospital from January 2019 to August 2022 were retrospectively analyzed. Thereafter, children were divided into two groups according to whether intraoperative ureteral tailoring was performed, including 9 in the trimmed group and 12 in the nontrimmed group. In the meantime, there were 16 males and 5 females, with the age of 4.7 ± 2.12 years. Furthermore, there were 17 obstructive MGU cases, 2 reflux MGU cases, and 2 obstructive with reflux MGU cases, with 16 cases on the left side (including 1 case of Y-shaped ureter in the left duplicated kidney), whereas 5 on the right side. All children underwent transvesicoscopic ureteral reimplantation (the Cohen procedure). Thereafter, changes in operation time, duration of retained catheterization, hematuria time, renal pelvis and ureteral dilatation, and tortuosity between two groups were compared 3 months after Double-J tube removal.
Results:
All children were effectively treated with transvesicoscopic ureteral reimplantation, the operation time (p = 0.02, p < 0.05), postoperative hematuria time (p = 0.00, p < 0.05), and retained urinary catheter time (p = 0.00, p < 0.05) were shorter in the nontrimmed group, and the mean postoperative follow-up time was 27.6 (3–22) months. Moreover, the postoperative anteroposterior diameters of the affected renal pelvis in both groups were 0.31 ± 0.39 cm and 0.27 ± 0.29 cm, respectively, whereas the postoperative maximum ureteral diameters were 0.33 ± 0.31 cm and 0.27 ± 0.36 cm, separately, which were significantly reduced compared with the preoperative counterparts. All children recovered well, with no postoperative complications.
Conclusion:
Whether intraoperative ureteral clipping is performed or not does not significantly affect the outcome of transvesicoscopic laparoscopic ureteral bladder reimplantation for primary MGU in children. Both groups of children improved with satisfactory surgical results, but the nontrimmed group has shorter operation time, simpler operation, and less trauma.
Introduction
Primary megaureter (MGU) is a general term for a condition where the ureter is tortuously dilated due to primary vesicoureteral reflux (VUR), primary obstructive megaureter (POM), or both (or neither). It is commonly seen in boys, with the ureteral diameter >7 mm, usually on the left side. 1 MGU is frequently detected by recurrent urinary tract infections (UTIs), abdominal pain, or physical examination. It can lead to hydronephrosis, UTI, and subsequent renal dysfunction. This comparative study aimed to examine the efficacy of intraoperative ureteral reimplantation with or without intraoperative ureteral trimming in the treatment of children with primary MGU.
Materials
Clinical data of 21 children undergoing transvesicoscopic ureterovesical reimplantation for MGU at our department from January 2019 to August 2022 were retrospectively analyzed. The patients were later divided into two groups according to whether intraoperative ureteral trimming was performed or not, including 9 in the trimmed group and 12 in the nontrimmed group. There were 17 cases of obstructive MGU, 2 of reflux MGU, and 2 of obstructive MGU with reflux, with 16 cases on the left side (including 1 case of Y-shaped ureter of the left duplicated kidney), whereas 5 on the right side, and a total of 22 ureters were treated.
The primary symptoms included UTI in 1 case, abdominal pain in 14 cases, and findings on medical examination in 6 cases. The bladder volumes in both groups, preoperative and postoperative ureteral diameters, renal cortical thicknesses and pelvic separation, operation time, postoperative hematuria time, and retention of catheterization time were compared between the two groups. In this study, clinical data were collected with the approval and consent of the Ethics Committee of our hospital.
Inclusion criteria: MGU with POM, primary reflux MGU, or both. Cases aged ≥1 year with the presence of clinical manifestations such as UTI or abdominal pain. Imaging findings suggestive of tortuous ureteral dilatation and ureteral diameter >7 mm.
Exclusion criteria:
All the secondary causes of MGU, such as posterior urethral valves, and neurogenic bladder.
Ureteral diameter ≤7 mm, as suggested by ultrasound despite the tortuous dilatation of the ureter.
Children with combined ureteropelvic junction obstruction or multiple ureteral strictures.
Children aged <1 year.
Surgical method
After general anesthesia, each case was placed in the supine position with the buttocks slightly elevated and both the lower limbs being abducted. After urinary emptying, the cystoscope was inserted and a pneumovesicum tube was connected to inject the carbon dioxide gas to maintain the pneumovesicum pressure at 8 to 10 mm Hg. Then the bladder was filled and the full bladder was touched below the umbilicus in the midline of the abdomen. Then about 2 cm below the umbilical level, two stitches of 2-0 absorbable sutures were used for percutaneous fixation of the bladder to the anterior abdominal wall (a 5-mm trocar was inserted into the bladder between the two sutured sites). The second and third 3-mm trocars were inserted 3 cm lateral to the 5-mm trocar on both sides in a similar manner (use of 3-mm operating instruments). Then the cystoscope was withdrawn.
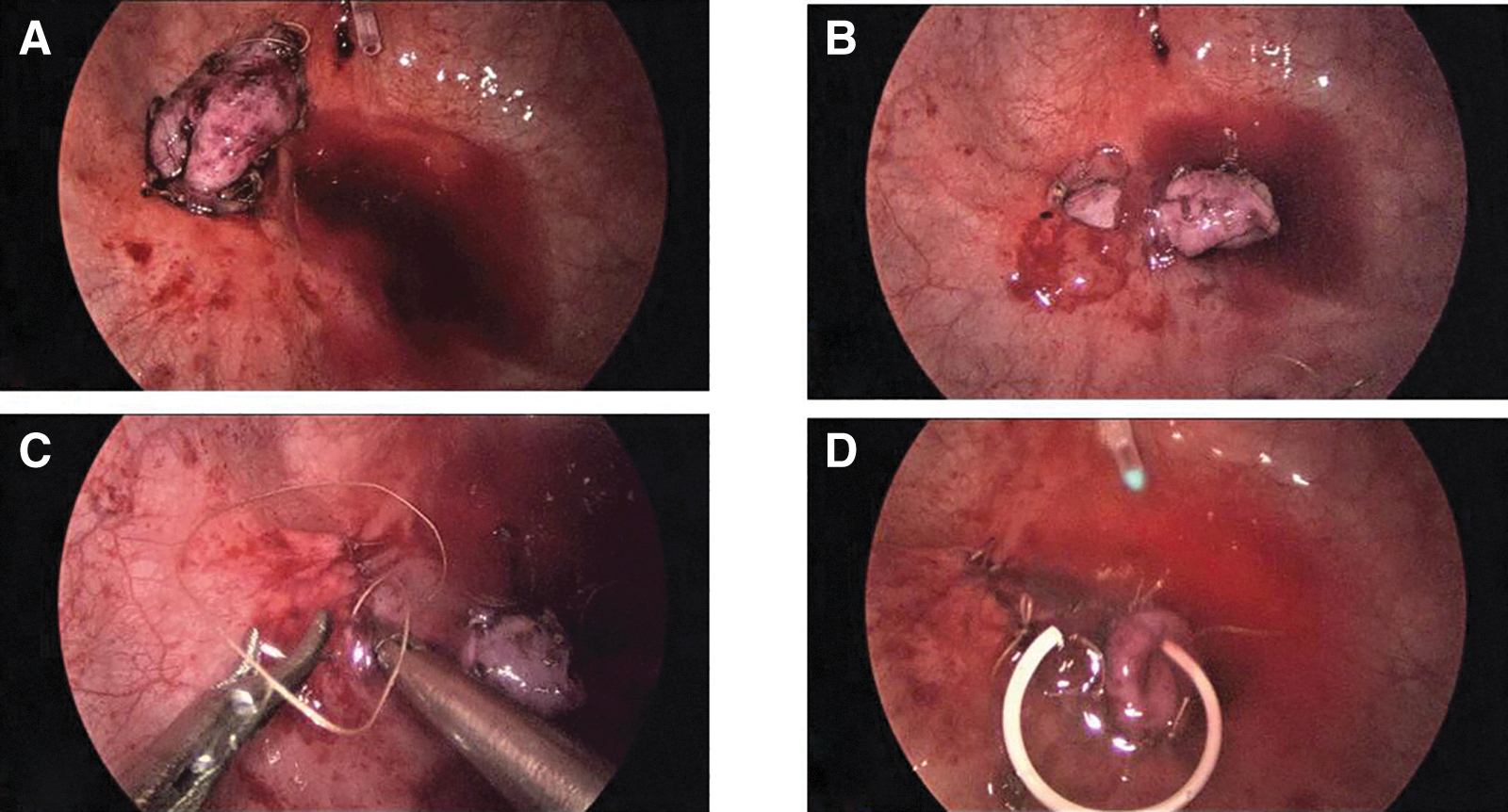
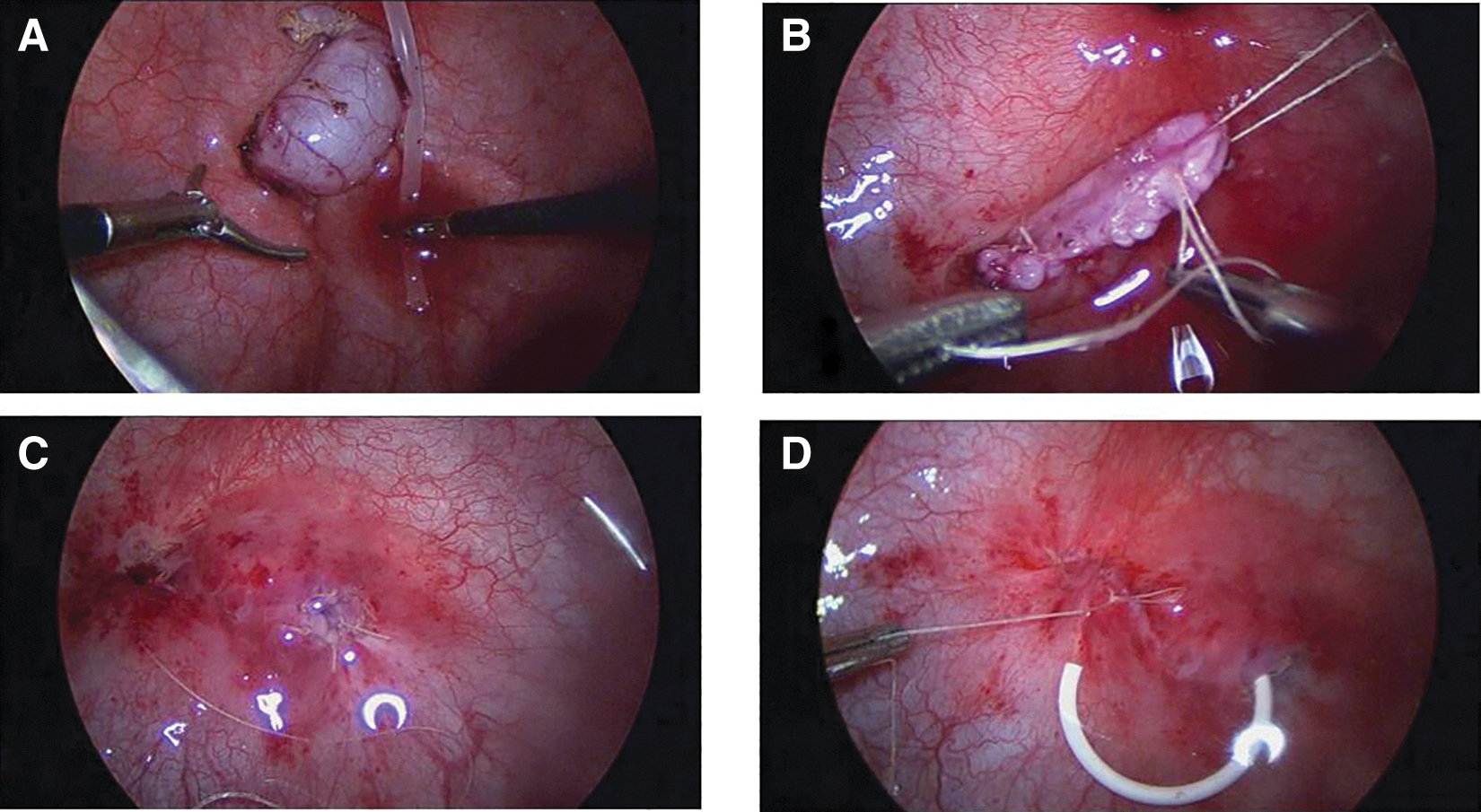
The 5-mm laparoscope was later connected and inserted into the bladder, later the bilateral ureteral openings were observed, the bladder mucosa was circumferentially incised along the opening of the affected ureter, and the ureter was fully freed, with its distal end being sutured to the contralateral bladder wall for traction in the ureteral cut group. Then, the ureter was cut along the ureteral alignment, and the post cut ureter was sutured with the 5-0 absorbable thread (this step was omitted in the nontrimmed group, see Fig. 1; for the trimmed group, see Fig. 2).
The submucosal bladder tunnel was made, and the affected ureter was dragged to the opposite side via this tunnel, intermittently anastomosing the ureteral opening to the bladder mucosa, and the original ureteral opening was fixed with a single suture between the bladder muscle and the ureteral pulp muscle layer, for the sake of preventing retraction of the ureter. A Double-J tube was routinely placed in the ureter via the urethra. The catheter was retained postoperatively.
Statistical analysis
Statistical analysis was performed using SPSS 16.0 software. After testing, continuous variables conformed to a normal distribution, which were expressed as x ± s and compared between two groups by the t-test, and variables not conforming to a normal distribution were expressed as median and range. p-Value <0.05 was considered statistically significant.
Results
Both groups of children were performed the laparoscopic procedure in the pneumovesicum without intermediate opening, and all of them had their internal Double-J tubes removed 1 month after surgery. All children were advised to take a prophylactic dose of antibiotics at bedtime during the postoperative period, to prevent medically induced VUR due to the Double-J tube. The mean follow-up period after surgery was 27.6 (3–22) months. Ultrasound findings were compared with those 3 months after removal of the Double-J tube. There was no significant difference in bladder volume between the two groups, and no recurrence of reflux was revealed with VCU examination in all children. All children did not report any postoperative complications such as urinary leakage or restenosis, with no recurrence of clinical manifestations such as UTI and abdominal pain.
Corresponding data were compared, which suggested statistical differences between the two groups in terms of operation time (p = 0.02, p < 0.05), postoperative hematuria time (p = 0.00, p < 0.05), and duration of indwelling urinary catheter (p = 0.00, p < 0.05), which were lower in the nonclipped group than in the clipped group. In addition, the anterior and posterior diameters (APD) of the affected renal pelvis were 0.31 ± 0.39 cm and 0.27 ± 0.29 cm, respectively, and the maximum diameters of the ureter were 0.33 ± 0.31 cm and 0.27 ± 0.36 cm, respectively, in the two groups after surgery, both of which were significantly reduced compared with those before surgery (p < 0.05). There was no statistically significant difference in terms of recovery after surgery between the two groups (p = 0.66) (Table 1).
Comparison of Demographic Characteristics Between the Two Groups
There was no statistical difference in age between the two groups.
p-Values of 0.00 and 0.02 for preoperative and postoperative APD and ureteral diameter statistical comparisons in the trimming group, respectively, both p < 0.05.
p-Values for preoperative and postoperative APD and ureteral diameter statistical comparisons in the no-trimmed group were 0.001 and 0.00 respectively, both p < 0.05.
APD = anterior and posterior diameters of renal pelvic; POM = primary obstructive megaureter; UTI = urinary tract infection; VUR = vesicoureteral reflux.
Discussion
For the surgical treatment of MGU in children, it is necessary to consider the age of the children, the diameter of the ureter, the cause of the disease, as well as the presence of clinical symptoms and renal function. Reflux MGU in children may heal spontaneously, but it should be treated conservatively first. If a breakthrough febrile UTI develops during the course of conservative treatment, or if a renogram shows increased renal scar formation during follow-up, surgical treatment is required. 2 As POM also has the potential to heal spontaneously, it has been suggested that POM children younger than 1 year of age may be placed on conservative observation, 3 but it is controversial whether antibiotic treatment is needed during conservative observation. 4
Braga et al. 5 followed up 80 children with POM younger than 24 months of age, and ∼76% of children with giant ureters resolved at a median age of 19 months, which suggested that a ureteral diameter ≥17 mm was an indication to consider the need of surgical intervention. The following conditions are considered by the British Association of Pediatric Urologists for surgical intervention in children with MGU: (1) the presence of recurrent UTIs, abdominal pain and discomfort, (2) increased dilatation of the pelvic ureter in children at follow-up, and (3) renal charts showing renal function below 40%. 6 Deng et al. 7 discovered that early surgical intervention for hydronephrosis in infants and children (before renal function was <40%) resulted in superior recovery of renal function to intervention after renal impairment (renal function <40%).
In our opinion, surgical intervention is required for children aged <1 year with asymptomatic MGU if the renal function is <40%; while for those aged ≥1 year with symptomatic MGU, surgical intervention can be considered even if the renal function is ≥40%, so as to help the postoperative renal functional recovery in the children. All children in this study group were treated surgically for clinical manifestations such as UTI and abdominal pain.
The following treatment modalities can be selected for primary MGU in children: (1) endoscopic treatment with injection or balloon dilation, (2) ureteral bladder reimplantation outside the bladder, and (3) ureteral bladder reimplantation inside the bladder. 1,2,8 Surgical treatment is still required for children with long end-stenotic segments of the ureter or with poor endoscopic results. Moreover, there are various surgical approaches to ureteral bladder reimplantation via the extravesical route. 9 –11 Esposito et al. 12,13 found that robot-assisted extravesical reimplantation could be a first-line surgical approach for children with VUR, and there was no significant difference between laparoscopic extravesical ureteral reimplantation and robot-assisted extravesical reimplantation in short-term bladder dysfunction, in their series, bilaterality, preexisting bladder and bowel dysfunction and duration of surgery were confirmed on univariate and multivariate analyses as predictors of postoperative bladder dysfunction.
Some scholars have compared ureteral bladder reimplantation between ex vivo ureteral tailoring and in vivo tailoring via the laparoscopic route, and their results demonstrate that laparoscopic in vivo ureteral tailoring is safe and feasible. 14 Li et al. 15 compared the results of laparoscopic repair of ureterovesical junction malformations in children between two routes, as a result, the internal bladder approach was more suitable for children with significant ureteral tortuosity and dilatation and for those with combined ureteral dilatation and voiding difficulties. Typically, the Cohen and Politano-Leadbetter approaches are the most used for the intravesical approach. In children with MGU, the ureteral diameter is too gross, and the bladder space is too limited to make a long enough submucosal tunnel at a ratio of 5:1; therefore, it is necessary to trim the ureter intraoperatively to achieve a better antireflux effect. 16,17
The megaureteral folding methods, which involve the expansion of Starr and Kalcinsky procedures, reduce the damage to the ureteral blood supply intraoperatively, decrease the diameter of the ureter while keeping the tunnel length constant, and increase the ratio of submucosal tunnel to ureteral diameter, thus reducing the incidence of postoperative reflux to some extent. 18 In the nontrimmed group, the tortuously dilated ureter was pulled directly through the submucosal tunnel of the bladder, so that the ureter itself received compression within the tunnel and folded itself, similar to the ureteral fold reimplantation, and this phenomenon also partially reduces the incidence of postoperative VUR.
Regarding submucosal tunnels, the ratio of 1:5 is required for gas vesicoureteral bladder reimplantation, but our experience suggests that the ratio of 1:5 cannot be achieved in MGU children with or without ureteral trimming. The principle of endoscopic injection for VUR is to inject an injection into the ureteral orifice or the submucosa of the inner segment of the ureteral bladder wall under the direct cystoscopic vision, for the sake of elevating and narrowing the ureteral orifice, thereby artificially forming an antireflux biologic flap and relatively extending the length of the intervestibular segment of the ureteral bladder wall for antireflux purposes. However, it remains uncertain whether the ureteral wall interstitial length to ureteral diameter ratio of 1:5 is achieved. 19
Han et al. 20 analyzed 214 children undergoing Cohen's procedure for POM or VUR and divided them into two groups according to the ratio of submucosal tunnel length to ureteral diameter ≥5 or <5. As a result, there was no statistical difference between the two groups and it was concluded that the submucosal tunnel length to ureteral diameter ratio ≥2.5 might be effective against reflux. Babu 21 used “minireimplantation” to treat 28 children with MGU and achieved good results and high success rates, with the intraoperative ureteral diameter to submucosal tunnel ratio of 1:2. These are comparable with our results. In our study, it was concluded that the intraoperative ureteral diameter to submucosal tunnel ratio ≥1:3 prevented postoperative VUR.
Kalayeh et al. 22 discovered in a modeling study that the ureteral diameter to submucosal tunnel ratio of 1:5 in ureteral bladder reimplantation does not overestimate the tunnel length to ureteral diameter ratio required to prevent reflux, which is consistent with our results. The bladder mucosa was sutured at the original affected ureteral orifice in the tunnel direction in both groups, which relatively lengthened part of the submucosal tunnel length of the bladder. According to our data, reflux MGU resulted in a smaller diameter of ureteral dilatation and a smaller chance of ureteral tailoring than POM. There were 12 cases whose ureter was not trimmed, and good postoperative recovery was achieved during the follow-up period. We believe that the size of the bladder should be taken into consideration and that the ureteral diameter alone should not be used as a criterion for clipping.
Combining ureteral diameter and bladder volume, the ureter can be left untrimmed in children with MGU who have enough bladder volume for an antireflux submucosal tunnel (ureteral diameter to submucosal tunnel ratio ≥1:3), whereas in children with MGU who do not have enough bladder volume for an antireflux submucosal tunnel (ureteral diameter to submucosal tunnel ratio <1:3), ureteral trimming is beneficial. This requires the surgeon to decide which procedure to perform based on the circumstances of the operation. Double-J tube-associated UTIs are common in children. 23 Ching 24 summarized recent studies related to the use of cranberry extract/juice and probiotics in the prevention of UTIs in children. According to their results, cranberry extract/juice and probiotics are useful for the prevention of UTIs in children, but more research with a larger sample size is warranted to verify their therapeutic mechanisms and instruct the dose and method of use.
To prevent the medically induced VUR due to the Double-J tube, a prophylactic dose of antibiotics is recommended for children every night at bedtime while the Double-J is in place. Our future studies will focus on intraoperative asepsis and “tube-free surgery” to reduce the use of antibiotics and the development of drug-resistant bacteria, while improving surgical technique and success rates.
Conclusion
Our present comparative study concludes that there is no significant difference in postoperative outcomes for MGU children with or without ureter tailoring. The untrimmed group has shorter operation time, postoperative hematuria, and indwelling catheterization time, and the intraoperative operation is relatively simple and easy to perform. When performing transvesicoscopic ureterovesical reimplantation in MGU children, a ratio of ureteral diameter to submucosal bladder tunnel close to 1:5, but not <1:3, is sufficient.
Limitations
Certain limitations should be noted in this work, such as the small sample size, insufficient follow-up time, lack of nephrograms as an objective preoperative and postoperative comparison, some biases in case management, a maximum ureteral diameter of 2.2 cm being treated, and larger ureters have not yet been encountered.
Footnotes
Authors' Contributions
Conceived and designed the study: H.C. Eligible study collection, quality assessment, and data extraction: Y.-S.C. Statistical analyses, preparation of tables and figures: H.C., Q.-F.D., and C.-k.M. Wrote and revised the article: H.C. All authors reviewed the final article.
Ethics Approval and Consent to Participate
This research is retrospective and involves the collection of existing data and records. All procedures performed in this study involving human participants were in accordance with the relevant guidelines and regulations approved by the Institutional Research Ethics Board of Anhui Provincial Children's Hospital and with the Helsinki Declaration and its later amendments or comparable ethical standards. As the study was retrospective in nature and therefore did not change the clinical management of patients involved. The Institutional Research Ethics Board of Anhui Provincial Children's Hospital approved all procedures of the study and provided a waiver for the written informed consent.
Availability of Data and Materials
The data in the study are transparent and open. The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
No funding was received for this article.