
Abstract
Introduction:
With the rise in the detection of incidental small renal masses (SRM), the management paradigm for these patients has become an issue of increasing concern. We aim to identify areas of consensus, controversy, and opportunities for improvement among recently published guidelines and assess the strength of evidence for the management of SRMs.
Methods:
We reviewed practice guidelines for SRMs promulgated by the American Urological Association, European Association of Urology, National Comprehensive Cancer Network, American Society of Clinical Oncology, European Society for Medical Oncology, and the Chinese Society of Clinical Oncology. Levels of evidence and strength of recommendations for evaluation, management and follow-up were analyzed with regard to consensus, conflict, and neglect.
Results:
There is consensus among guidelines for the initial evaluation and treatment of SRMs; however, discrepancies exist with regard to indications for active surveillance, thermal ablation, and timing/method of follow-up after treatment. Routine renal mass biopsy is not recommended by any guideline. Overwhelmingly, guideline statements are based on low to moderate levels of evidence; only 23% of the reviewed guidelines were based on high-level evidence, 38% based on moderate-level, and 39% on low-level evidence or expert opinion.
Conclusions:
Despite all six guidelines sharing a consensus on most management topics regarding SRMs, the ongoing lack of high-level evidence precludes gold standard recommendations in the areas of diagnosis, treatment, and follow-up. More high-quality studies are needed to develop a stronger, data-supported universal guideline for the management of SRMs.
Introduction
With an increased number of renal tumors being detected due to widespread use of CT, there are many reasons to develop high-quality, evidence-based, and cost-effective strategies for the evaluation and treatment of small (i.e., ≤4 cm) renal masses (SRMs). 1 The management of SRMs is an issue of major concern for several reasons. First, the majority of SRMs are asymptomatic and incidentally detected. 2 Second, more than 20% of excised SRMs are benign and would likely never require therapy. 3 Removal of a benign SRM invariably leads to partial or complete nephron loss of the affected kidney. Lastly, malignant SRMs tend to be of a lower histologic grade, have a favorable prognosis, and could be considered for a nonsurgical surveillance or a less invasive thermal ablative approach. 4
Despite the foregoing observations, with the increased incidence of SRM, there has been a concomitant increase in surgical procedures performed. Not surprisingly, the increase in surgical removal of SRMs has not led to a proportional improvement in the overall survival in patients affected by renal cancer. 5 Clinical tools such as renal mass biopsy (RMB) that allow clinicians to risk stratify patients continue to be used at a low rate, and thus, routine pretreatment RMB continues to be controversial. 6 The traditional paradigm of initial extirpative surgery for all renal tumors detected on imaging, followed by a histopathologic diagnosis, is at odds with the management of other solid masses (e.g., lung, prostate, breast, bladder, liver, colon), which are first biopsied and, only if proven malignant, proceed to surgical excision.
This inverted approach in urologic practice seems to have evolved from a time when the vast majority of renal masses were large and presented with symptoms; indeed, before the age of CT scanning, incidental renal tumors were a rarity, and the vast majority of renal masses were beyond T1a and almost invariably malignant.
Clinical practice guidelines (CPGs) are systematically developed disease-specific statements designed to assist clinicians and patients in making decisions about appropriate health care. 7,8 Several local, national, and international urologic and oncologic societies have developed CPGs for the management of kidney cancer. 9 Due to the varying ways in which the literature is reviewed and the strength of evidence is assessed, the resulting recommendations in some areas vary greatly. The following review aims to assess the recommendations and strength of evidence of recently published guidelines for the diagnosis and management of SRMs to identify areas of consistency, controversy, and neglect. We sought to overcome the challenges of comparing guidelines with heterogenous methodologies for evaluating evidence by developing a standardized grading scale. Using this system, all guidelines could be equally analyzed in an evidence-based systematic manner allowing us to assign a high, moderate, or low level of evidence (LOE) to each recommendation.
Methods
Selection of guidelines
The guidelines included for review were selected based on a 2019 study by Hou et al., which used the Appraisal of Guidelines for Research and Evaluation (AGREE II) instrument to assess the methodologic quality and reporting of the latest available CPGs for kidney cancer. 9,10 The authors identified 2 out of 13 CPGs on kidney cancer that they would recommend (AGREE II score >60%), and an additional eight guidelines that they would recommend with modifications (AGREE II score 30%–60%). We reviewed the 10 recommended guidelines and gleaned the CPG recommendations specific to the diagnosis and management of SRMs. In addition, we reviewed the respective societies' websites for more recent updated versions of their CPGs.
Review of guideline recommendations
Five researchers (S.N.A., A.P., A.B., R.B.A., J.L., and L.X.) evaluated the CPGs for inclusion into the study. Recommendations pertaining to the management of SRMs were tabulated using Microsoft Excel (Seattle, WA) correlating guideline statements in the following areas: initial evaluation, pretreatment biopsy, management, and follow-up. The extracted recommendations were further analyzed by three additional reviewers (S.N.A., P.J., and Z.O.) for consistency and accuracy of interpretation.
Review of LOE and strength of recommendations
Information on the associated LOE and strength of recommendations (SOR) for each of the guideline recommendations was extracted (Table 1). As there were variations in how individual guidelines provided grading scales on LOE and SOR, standardized grading scales (Tables 2 and 3) were created for the purpose of comparison. Levels of evidence were analyzed, and the number of high-, moderate-, and low-evidence statements was quantified for each guideline (Fig. 2).
Individual Grading Scales for Levels of Evidence and Strength of Recommendations
ASCO = American Society of Clinical Oncology; AUA = American Urological Association; CSCO = Chinese Society of Clinical Oncology; EAU = European Association of Urology; ESMO = European Society for Medical Oncology; LOE = level of evidence; NCCN = National Comprehensive Cancer Network; RCT = randomized control trial.
Standardized Grading Scale for Levels of Evidence
Standardization of Grading for Strengths of Recommendations
Results
Seven CPGs from six separate societies were reviewed: American Urological Association (AUA, 2013, 2017), European Association of Urology (EAU, 2015), National Comprehensive Cancer Network (NCCN, 2017), American Society of Clinical Oncology (ASCO, 2017), European Society for Medical Oncology (ESMO, 2016), and the Chinese Society of Clinical Oncology (CSCO, 2015). Three guidelines were excluded due to their primary focus on the management of metastatic disease. Recommendations from four updated versions of the guidelines were also included: AUA 2021, EAU 2022, NCCN 2022, and ESMO 2019 (Fig. 1).
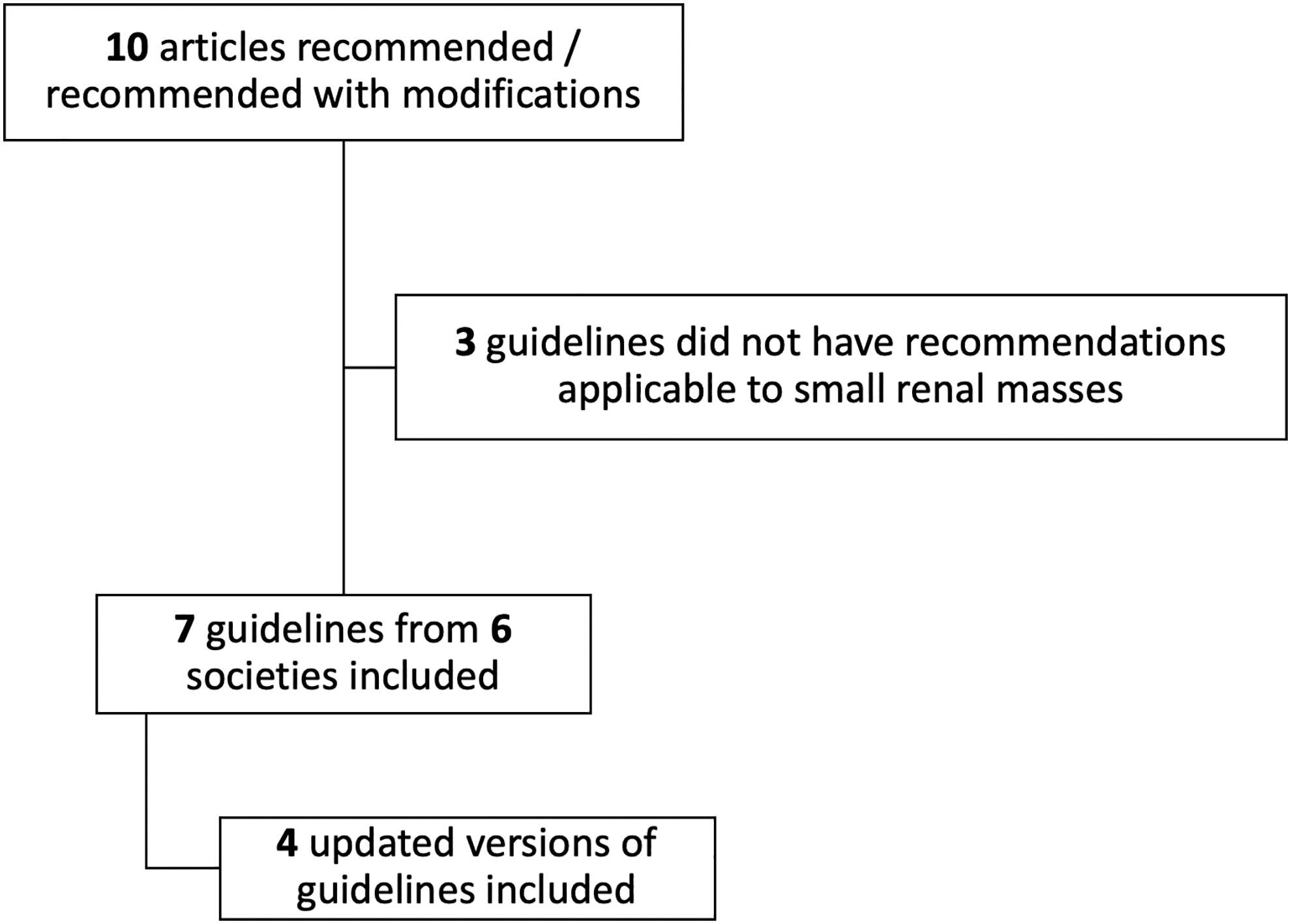
Flowchart for CPG inclusion. CPG = clinical practice guideline.
Characteristics of CPGs and quality of evidence
All guidelines are evidence based (Table 1); however, the quality of evidence has a broad range with inclusion of expert opinion and clinical principles where evidence is lacking. When examining the quality of evidence used to inform all six societies' guideline statements, only 23% (90/393) are based on high-level evidence, while the remaining 77% are based on moderate (148/393)- and low-level evidence or expert opinion (155/393) (Fig. 2). Final recommendations are decided by panel consensus for the CSCO and NCCN guidelines. The ASCO guideline specifically focuses on SRMs, while other guidelines were broader, including localized renal cancer (AUA), or all forms of renal cancer (EAU, NCCN, CSCO, ASCO, ESMO). The AUA, EAU, NCCN, CSCO, and ESMO guidelines are comprehensive and include all aspects of diagnosis, treatment, and follow-up. Of note, despite the prevalence of SRM, only the ASCO guideline specifically focuses on biopsy and treatment options for SRM.

All guideline statements stratified by LOE (See Supplementary Material for references to guidelines). LOE = level of evidence.
Recommendations on initial evaluation
All the guidelines (except ASCO, which does not address initial SRM evaluation) recommend abdominal CT with contrast as the primary imaging modality to diagnose and characterize renal tumors, or alternatively, an abdominal MRI with gadolinium-based contrast (Table 4). The above recommendations although strong are based on moderate-level evidence (NCCN, EAU, ESMO) or clinical principle alone (AUA). ESMO strongly recommends a pelvic CT as mandatory, while it is optional for NCCN (moderate). The updated EAU guidelines also recommend contrast-enhanced ultrasound as a viable imaging modality in cases where contrast-enhanced CT has indeterminate findings (strong). Only EAU and CSCO recommend renal function imaging in patients with comorbidities, solitary kidney, or bilateral tumors (moderate).
Recommendations on Initial Evaluation
X = not specified in guideline.
MRI was also discussed as an alternative imaging modality.
CXR = chest x-ray.
All guidelines, except ASCO, make strong recommendations regarding chest imaging as necessary to rule out pulmonary metastasis, however, evidence level is low; only ESMO recommends chest CT as mandatory, whereas the EAU suggests that CT imaging may be omitted in asymptomatic patients' T1a lesions and no nodal involvement. All the guidelines agree, with moderate- to low-level evidence, that a bone scan for bone metastasis is only required if clinically indicated by symptoms or laboratory results (e.g., bony pain or elevated alkaline phosphatase). Basic laboratory studies such as complete blood count, comprehensive metabolic panel (including lactate dehydrogenase), and urinalysis are recommended by all the guidelines with low-level evidence to support the recommendation.
Recommendations on biopsy
Based on moderate- to low-level evidence or solely clinical principle, all guidelines strongly recommend against routine biopsy for incidentally detected SRMs (Table 5). All recommendations are based on one of two principles. First, if the results of an RMB will change patient management, only then do most guidelines recommend biopsy. Second, if patients are scheduled to undergo ablation, then the AUA, EAU, NCCN, ASCO, ESMO, and CSCO recommend RMB (moderate to low). All guidelines agree that RMB may be offered in select cases if the origin of the mass is suspected to be hematologic, metastatic, inflammatory, or infectious (expert opinion). RMB is also recommended before systemic therapy to guide treatment.
Recommendations on Biopsy
In cases where biopsy results may alter management.
RMB = renal mass biopsy.
Recommendations based on moderate- to low-level evidence are made for RMB before active surveillance (AS) by the EAU, ESMO, and NCCN (weak, moderate, and moderate recommendations, respectively). In contrast, ASCO considers RMB as elective before AS and the AUA recommends RMB only if the oncologic benefits of no intervention outweigh the risks of treatment (moderate). The CSCO makes no recommendation on RMB before AS.
All guidelines differ in recommendation for when RMB is not required. The AUA and EAU discourage RMB in patients with significant comorbidities (expert opinion). Also, predominantly cystic masses are considered a contraindication to RMB according to the EAU and ASCO guidelines.
With moderate levels of evidence, the use of core biopsy, as opposed to a fine needle aspiration, is strongly recommended by the EAU and ASCO, and moderately recommended by the AUA, ESMO, and NCCN. Only the EAU provides a specific recommendation as to the number of cores to be taken, that is, two cores (moderate) and that a coaxial cannula be used to avoid biopsy tract seeding (weak).
Recommendations on treatment
Surgical management
All guidelines recommend that partial nephrectomy (PN), when technically feasible, should be prioritized over radical nephrectomy (RN) for the surgical treatment of SRMs (Table 6). This is a strong recommendation based on high-level evidence by the EAU, ASCO, and ESMO, and a moderate recommendation based on moderate-level evidence by the AUA, NCCN, and CSCO. In addition, the AUA, NCCN, CSCO, ASCO, ESMO, and EAU stress that PN should be pursued among patients with significant comorbidities, bilateral tumors, chronic kidney disease, and in situations through which preservation of renal function is of primary importance (e.g., solitary kidneys) (moderate, moderate, moderate, no recommendation, no recommendation, and no recommendation, respectively). All six guidelines recommend RN when PN is not technically feasible.
Recommendations on Treatment
PN = partial nephrectomy; RCC = renal-cell carcinoma; SRMs = small renal masses.
Thermal ablative therapies
The AUA, NCCN, and ESMO recommend thermal ablation (TA) as an alternative option for SRMs ≤3 cm, whereas the CSCO uses ≤4 cm as a cutoff; ASCO does not provide a specific size limitation, however, the EAU does not recommend radiofrequency ablation for masses >3 cm and cryoablation for lesions >4 cm (weak). The ESMO and EAU present strong and weak recommendations, respectively, for TA as a treatment option only for patients who are of high surgical risk and/or frail. ASCO recommends ablation if there is high confidence that complete ablation will be achieved (moderate). CSCO limits TA to patients not suitable for surgery with peripherally located tumors (moderate). When TA is the selected therapy, radiofrequency ablation or cryoablation are equally noted as viable treatment options.
Active surveillance
All the guidelines recommend that AS may be considered initial management for SRMs ≤2 cm in size especially among elderly patients or those with significant comorbidities (Table 6). These recommendations are either weak (AUA, EAU) or moderate (NCCN, ASCO, ESMO, CSCO). Evidence cited by the EAU includes single-center comparative reviews and multicenter prospective trials that show no significant differences in overall survival or cancer specific survival for AS vs surgical management for T1a renal masses in older patients (>75 years). In contrast, with moderate- to low-level evidence (AUA, NCCN) most guidelines fail to make recommendations for AS among patients otherwise suitable for surgery despite robust data indicating slow growth rate, low risk of progression and metastasis for SRMs, and the resultant loss of nephrons, in part, or completely from the affected kidney.
As described above, risk stratification tools such as RMB are only conditionally recommended based on expert opinion and are reserved only for patients in whom risk of AS is equivocal or outweighs the risk of intervention (e.g., AUA 2021).
Recommendations on follow-up
Recommendations on follow-up among patients undergoing AS largely rely on low-level evidence or expert opinion (Table 7). The AUA and NCCN recommend abdominal imaging within 3–6 months of AS initiation and then annually: NCCN specifies that the abdominal imaging should be CT/MRI with contrast, if there are no contraindications. The AUA and NCCN recommend an annual chest X-ray, with the NCCN providing CT as an additional option. ASCO recommends a more rigorous schedule for patients undergoing AS: chest x-ray and CT abdomen (or ultrasound [US]) every 3 months for the first year, then every 6 months for the next 2 years, and annually thereafter.
Recommendations on Follow-Up
US = ultrasound.
Specific imaging modalities and timing of follow-up after surgical or ablative treatment vary among the guidelines. Most guidelines attempt to risk stratify patients based on varying risk stratification systems. The AUA and NCCN risk stratify based on clinical stage (AUA (pT1 + ISUP 1/2 = low risk, pT1 and ISUP 3/4, or any pT2 = intermediate risk, pT3 = high risk, pT4 or pN1, or adverse features sarcomatoid, rhabdoid = very high risk) and NCCN (Stage I = low risk, Stage II = intermediate risk and Stage III, IV = high risk)). The EAU uses Leibovich scores (Leibovich 0–2 = low risk, Leibovich 3–5 = intermediate risk, Leibovich >6 = high risk) for clear cell renal cell carcinoma (ccRCC) and the UCLA integrated staging system for non-ccRCC in determining risk of recurrence.
Following surgery for low-risk disease, the AUA recommends an abdominal CT or MRI and CXR at 12, 24, 48, and 60 months for PN and RN. For intermediate-risk disease, imaging is recommended every 6 months for the first year, and then annually for 4 years. For high-risk disease, follow-up is more involved with imaging recommended every 6 months for the first 4 years and annually thereafter. For very high-risk diseases, the AUA recommends abdominal imaging every 3 months for the first year, then every 6 months up to 3 years, and annually thereafter. CT chest is recommended in lieu of CXR for intermediate- and high-risk disease. Imaging follow-up after TA is recommended within 6 months, and then follows the previously stated intermediate-risk schedule. Follow-up after 60 months for all risk categories is based on informed/shared decision-making. All the above recommendations are based on expert opinion.
While the EAU strongly recommends that follow-up should depend on risk stratification, it suggests a general schedule for follow-up imaging and makes no differentiation among patients treated with PN, RN, or TA. For low-risk disease, CT chest and abdomen are suggested at 6, 18, and 30 months with the option to terminate surveillance at 3 years. For intermediate-risk disease, a CT chest and abdomen are recommended every 6 months for the first year and then annually up to 5 years. For high-risk disease, they recommend CT abdomen and chest every 3 months for the first 6 months, then every 6 months for up to 3 years, and annually thereafter.
For clinical stage I, the NCCN recommends CXR or chest CT annually for 5 years and abdominal CT/MRI 3–12 months of treatment, then annually for 5 years. For clinical stage II, the NCCN recommends a baseline abdominal and chest CT or MRI within 6 months, then every 3–6 months for 2 years, and annually up to 5 years. For clinical stage III, the NCCN recommends a baseline abdominal and chest CT or MRI within 3–6 months, then every 3–6 months for 3 years, and annually up to 5 years. Interestingly, the NCCN lists the US as a viable surveillance option for stage III disease.
Like the AUA, the NCCN makes a distinction between surgery and TA and recommends an abdominal CT or MRI within 1–6 months following TA, and then, CT, MRI, or US annually up to 5 years. A CXR is recommended annually for 5 years for patients with biopsy-proven low-risk renal-cell carcinoma (RCC), nondiagnostic biopsy, or no prior biopsy.
ESMO recommends follow-up time intervals based on risk factors but gives no further specifics; a yearly CT scan is “probably” sufficient in low-risk patients and CT scan every 3–6 months for 2 years in high-risk patients (expert opinion). For low-risk disease, the CSCO recommends an abdominal CT/MRI 3–12 months from the date of surgery, with abdominal US, CT, or MRI and chest X-ray performed every year for 3 years. For high-risk disease, CT imaging is recommended every 6 months for 3 years and then yearly for 5 years.
Discussion
The prevalence of kidney cancer continues to rise: in 2018, globally there were an estimated 403,262 new cases of kidney cancer and 175,098 deaths from renal cancer. 11 This increase may to some extent be explained by higher detection of SRMs due to more advanced imaging techniques. With increased detection, there has been an increase in surgical procedures despite the probability of an SRM being benign is upward of 30%; furthermore, when malignant, the likelihood of metastatic disease from an SRM is low. 12 Nonetheless, an extirpative treatment-first/diagnose-later strategy has persisted and risk stratification tools such as RMB and conservative management in the form of active surveillance remain underutilized.
The present review of all available societal guidelines regarding the diagnosis and treatment of SRMs outlines areas of contention between the various guidelines and highlights the generally poor quality of evidence that informs current practice recommendations. Ideally, CPGs created by various societies would provide strong recommendations on the management of SRMs and be supported by high-level evidence-based studies; however, this is not always the case, mostly due to lack of high-quality studies. As an example, in the 2021 AUA renal mass guideline, nearly 66% of the guideline statements (32/48) are based solely on expert opinion or clinical principle, and indeed, only one statement is based on Grade A evidence.
Evident from our review is a lack of level 1 evidence for conservative treatment strategies such as active surveillance and the role of RMB suggesting the need for high-quality prospective multi-institutional clinical studies as have been done or are ongoing for prostate cancer. 13,14
As previously illustrated, the rate of benign pathology after PN is well over 20%, and yet, RMB with its high diagnostic accuracy remains underutilized. 15,16 Richard et al. in a multicenter retrospective study found that 16% of excised SRMs were benign at centers that used RMB selectively (i.e., only 12% of SRMs underwent RMB) compared with only a 5% benign lesion rate at centers that favored routine preoperative RMB (i.e., 63% of SRMs underwent RMB). 3,17 Other studies have corroborated that RMB reduces the percent of SRM patients undergoing surgical excision and concomitantly increases the number of patients amenable to AS. 18,19 Additional lack of consensus surrounds the use of TA of a SRM. The guidelines cite this approach as an option usually reserved for elderly or high-risk patients due to the slightly higher rates of recurrence.
Realizing that the guidelines always lag the current literature, it is of note that evidence favoring the expansion of TA for SRM is mounting due to improvements in technique, better imaging, expanded operator experience, and advanced technologies; it is our contention that as RMB becomes more widespread, TA may well become the first-line therapy for SRM of questionable or low-grade malignancy. Areas of concern regarding RMB include its negative predictive valve (NPV) and nondiagnostic rate. In a systematic review by Patel et al., the NPV of RMB was ∼63%, suggesting that up to 37% of patients with a negative biopsy may harbor a malignant tumor. 15 However, more recent meta-analyses note a more favorable NPV of 80%. 20
Similarly, RMB in older series had a nondiagnostic rate of ∼14%; however, Okhunov et al. demonstrated that in patients with a SRM undergoing US-guided biopsy the overall diagnostic rate was 80% on the initial biopsy, which improved to 93% on subsequent repeat biopsy. 19,20 As such, with increasing experience, the accuracy and precision of RMB continue to improve.
The overtreatment of SRMs has multiple detrimental effects including surgical complications, psychosocial stress, financial loss, and reduced renal function. Surgical therapies such as PN despite excellent oncologic outcomes have a complication rate of 18.6%, making the case for the expansion of pretreatment RMB, risk stratification, and active surveillance. 21 Further on the horizon are emerging technologies such as radiomics and computer-based deep learning algorithms, which have shown promising results in detecting renal cancer by imaging alone, in which case the need for RMB could be called into question and yet this approach is tempered by the fact that even in prostate cancer, among patients with a PIRADS 5 lesion, biopsy still precedes treatment. 22
Conclusion
In the case of SRMS, while all six guidelines share a consensus on many management topics, the ongoing lack of high-level evidence precludes the gold standard recommendations on diagnosis, treatment, and follow-up. This reflects a need for the institution of national and international SRM registries to create a data-driven universal guideline for the management of SRMs. 23 Lastly, the ongoing morbid practice of “treatment before diagnosis” for SRM remains a conundrum in a world in which all other solid tumors (with the exception of the testis and adrenal tumors) require biopsy proof of malignancy before extirpative therapy.
Footnotes
Authors' Contributions
J.L. and R.V.C. conceived the project and were involved in reviewing the data and editing the article. S.N.A., A.P., A.B., R.B.A., and L.X. compiled the guidelines and extracted the data. S.N.A., P.J., and Z.O. were involved in reviewing the data for accuracy. S.N.A., A.P., D.B., R.B.A., P.J., and Z.O. were involved in writing and editing the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.