
Abstract
Introduction:
Electromotive drug administration (EMDA) delivers a drug deeply into targeted tissues, such as the bladder. EMDA has never been applied to the ureter.
Methods:
In four in vivo porcine ureters, a unique EMDA catheter containing a silver conducting wire was advanced for the infusion of methylene blue. In two ureters, a pulsed current was delivered through an EMDA machine, whereas the other two ureters served as a control. After 20 minutes of infusion, the ureters were harvested.
Results:
In the EMDA ureter, there was diffuse staining of the urothelium; penetration of methylene blue occurred in the lamina propria and muscularis propria. In the control ureter, there was only patchy staining of the urothelium.
Conclusion:
In this first report of ureteral EMDA, a charged molecule penetrated beyond the urothelium into the lamina propria and muscularis propria of the porcine ureter.
Introduction
The delivery of a therapeutic agent directly to diseased tissue avoids systemic side effects. A prime example of this is the treatment of superficial urothelial cancer with intravesical Bacille Calmette-Guérin or other topical chemotherapeutic agents. 1 Systemic absorption is scant (1%–5%). 2
Urothelium, which lines the renal pelvis down to the proximal urethra, is covered by a thick layer of glycoproteins and proteoglycans (i.e., glycosaminoglycan layer), which protects it from toxin absorption and diminishes bacterial adherence. 3 By the same token, it is a barrier to local therapy using chemotherapeutics or smooth muscle relaxants. Different approaches have been developed to overcome this barrier. Electromotive drug administration (EMDA) uses an electrical current to create electroporation, electrophoresis, and iontophoresis to induce faster and more directional movement of chemotherapeutics such as mitomycin C (MMC) into the urothelium and wall of the bladder than topical intravesical MMC. 4,5
Current density, current mode (pulsed vs direct), molecular weight, pH, and ionic strength affect EMDA performance. 6 In superficial bladder cancer, EMDA/MMC has a high response rate and improved progression-free rate; side effects are minimal. 7,8
Although EMDA in the bladder has been demonstrated to be safe and effective, its application in the ureter has never been investigated. 9 Ureters are anatomically designed to rapidly propel urine from the kidney to the bladder; maintaining contact with an infused medication with ureteral tissue remains challenging. By developing a novel approach, we sought to learn whether EMDA could be effectively applied to the ureter providing for diffuse penetration of drugs into the ureteral urothelium and deeper ureteral tissues and thus possibly deliver effective doses of chemotherapeutic agents in the case of ureteral transitional cell cancer or smooth muscle relaxants among patients undergoing ureteroscopic treatment of large renal stones.
Methods
The Institutional Animal Care and Use Committee (IACUC) at the University of California, Irvine, approved this study (UCI-IACUC No. AUP-21-131). Two female juvenile Yorkshire pigs were placed under general anesthesia. In the supine position, flexible cystoscopy was used to introduce a 0.035-inch guidewire (Sensor™ Boston Scientific®) into each ureter. The cystoscope was removed, and a 5F open-ended ureteral catheter was passed. The guidewires were removed, after which a retrograde pyelogram was performed. The guidewires were then replaced, and the 5F catheters were removed.
In all four ureters, a novel in-house fabricated 10F EMDA catheter with equidistant fenestrations (0.5 mm each) in three longitudinal rows over the distal 20 cm of the shaft of the catheter was advanced over both guidewires (Fig. 1) The guidewires were removed, and a 22-gauge silver conducting wire was passed into each of the four EMDA ureteral catheters; the conducting wire was advanced to the end hole of the catheter to prevent fluid from exiting the catheter's tip. The bladder was drained throughout the experiment with a 10F Foley catheter placed. A large skin dispersive conduction pad (11.5 inches × 7.5 inches) was placed on the planned treatment side of each of the two pigs and connected to the EMDA generator (negative electrode).

Schematics of the custom-designed catheter for upper urinary tract EMDA.
In the experimental EMDA ureters, the conducting wire was connected to the positive electrode of the EMDA electrical current generator (Physion® MINI, 30N2, Mirandola, Italy). Methylene blue (Biopharm Inc.), a water-soluble thiazine dye with a molecular weight of 319.85 g/mol and a net positive charge was diluted with sterile water (0.1% concentration). This solution was instilled simultaneously through both catheters at 5 mL/min using drug infusion pump (BYS-820 Changsha, China). Intraureteral pressure was observed by connecting the catheter to a central vein pressure column that was fractured at the 40 cm mark to protect the ureter and kidney from any potential backflow. 10
In each of the two experimental EMDA ureters, a positive pulsed electrical current was applied for 20 minutes while the methylene blue was being infused (Fig. 2). Based on previous safety studies for EMDA in the bladder, a current density of 0.5 mA/cm2 was chosen. 11 Accordingly, we used an electrical current of 10 mA to achieve a current density of 0.5 mA/cm2 based on the 20 cm2 of ureteral surface [20 cm (length) and a circumference of ≈1 cm] being treated. For each of the two control ureters, no electrical current was applied. At the end of the procedure, the EMDA catheters were removed, the pigs were euthanized, and all four ureters were harvested, bivalved, and frozen in liquid nitrogen for histopathologic analysis.
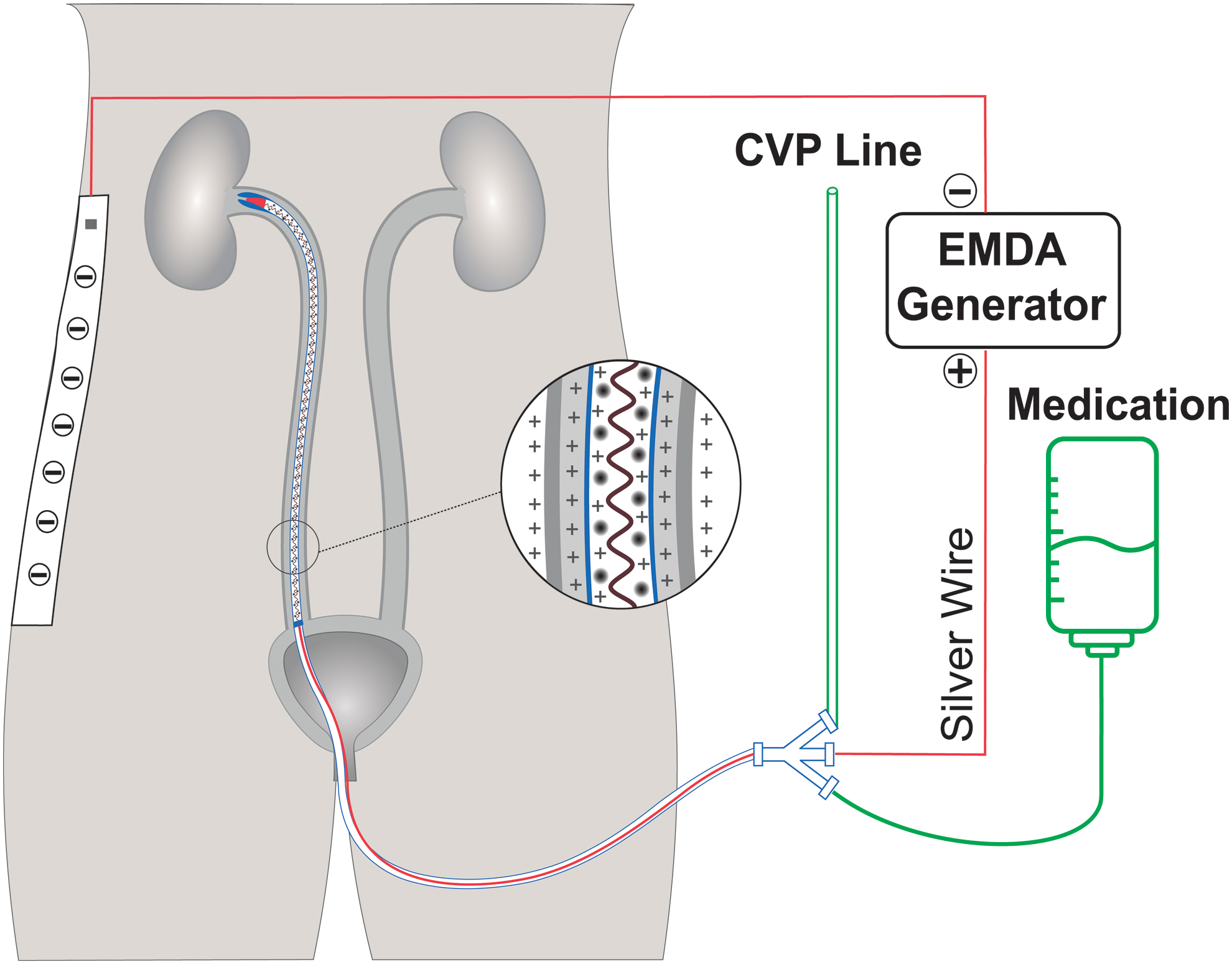
Schematic image of EMDA as applied to the experimental ureter. Silver conducting wire is connected to the positive electrode; the dispersive pad is connected to the negative electrode. Color images are available online.
Results
Both animals tolerated the procedure without incident. Macroscopically, the urothelium of the experimental EMDA ureters was visibly stained throughout the length of the ureter while there was only patchy staining of the urothelium of the control EMDA ureters (Fig. 3A). Microscopy of hematoxylin and eosin-stained sections of the ureters showed mild urothelial cell denudation that did not extend to the basal layer of the urothelium or the deeper tissues for the EMDA and control ureters (Fig. 3B, C).

Ureters post-EMDA.
In the experimental EMDA ureters, methylene blue was noted to extend beyond the urothelium and into the lamina propria and muscularis propria (Fig. 3D). In the control EMDA ureters, patchy methylene blue staining of the urothelium was seen without penetration into the wall of the ureter (Fig. 3E).
Discussion
In this in vivo animal model, using an in-house fabricated EMDA ureteral catheter, we documented significant penetration of methylene blue deep into the ureteral wall upon application of electrical current. To the best of our knowledge, this is the first study showing the effective application of EMDA in the ureter.
Because ureters are lined by urothelial cells with similar histologic and physiologic properties to the bladder, we applied the same principles to ureteral EMDA as are used for bladder EMDA. Our custom-designed EMDA catheter had the electrical conducting silver wire running through the middle of the catheter to ensure the distance from the conducting wire to the urothelium would be consistent along the length of the ureter. To ensure more uniform drug penetration and prevent skin burns and erythema beneath the pad, a large skin dispersive pad was placed on the flank of the pig. 12
There may be numerous areas of potential application for EMDA in the ureter; however, there are two areas that immediately come to mind: topical chemotherapy for ureteral transitional cell cancer and ureteral smooth muscle relaxation to facilitate passage of a ureteral access sheath (UAS) during ureteroscopic treatment of renal calculi. Topical chemotherapy has become an established approach for preventing tumor recurrence after transurethral resection of superficial bladder cancer. For upper tract transitional cell cancer (UTTCC), there is one product designed to enhance the dwell time of a chemotherapeutic agent: Jelmyto™.
This mitomycin-containing reverse thermal gel is a viscous liquid at room temperature but becomes semisolid at body temperature, thereby providing sustained exposure of the renal pelvis urothelium to the mitomycin. 13 In a phase 3 trial, Jelmyto was effective in controlling UTTCC in 59% of cases; however, there were significant side effects: ureteral strictures (44%), urinary tract infection (32%), hematuria (31%), flank pain (30%), and nausea (24%). 14 To date, there have been no published data with regard to using this formulation in the treatment of UTTCC of the ureter. Ureteral EMDA could represent a potentially unique form of topical therapy with minimal side effects.
The second area in which EMDA drug delivery to the ureter might play a role is for inducing acute ureteral smooth muscle relaxation for UAS placement during ureteroscopic lithotripsy. Studies have shown that the use of a larger UAS allows improved operative efficiency with no increased risk of ureteral stricture. 15 Unfortunately, placement of the largest UAS (16F) is accomplished in only 50% of ureters; indeed, in most cases, if one wishes to place the 16F access sheath, the patient is often subjected to a week of prestenting of the ureter. 16 Attempts at pharmacologically induced ureteral relaxation using an alpha blocker (i.e., tamsulosin) have provided conflicting results. 17,18
EMDA may allow for a variety of smooth muscle relaxing drugs to deeply penetrate the ureter, thereby possibly resulting in acute smooth muscle relaxation. If this were to occur, then larger access sheaths, rivaling or exceeding the size of current mini-percutaneous nephrolithotomy tracts, could be placed. The urologist could then approach even large renal calculi through a natural orifice transurethral approach, thereby avoiding the significantly higher complication rate incurred by a percutaneous transrenal approach. 19,20
This proof of concept pilot study has several limitations. First, it is an acute pilot study; hence there are no data on potential long-term adverse effects of EMDA drug administration on the ureter (stricture, muscle impairment, etc.). Second, we did not assess blood levels of methylene blue to determine systemic absorption. Lastly, it is undetermined whether the electric current might have altered the composition of methylene blue.
Conclusion
Using a unique EMDA ureteral catheter, methylene blue penetrated the porcine urothelium, lamina propria, and muscularis propria along the length of the ureter without incurring any acute tissue injury. This is the first report of the effective application of in vivo ureteral EMDA.
Footnotes
Acknowledgment
Dr. Zohreh Esam at the Pharmaceutical Science Research Center, Department of Medical Chemistry, Mazandaran University, provided valuable comments regarding the design of this study.
Authors' Contributions
S.H.H.S. contributed to conceptualization, methodology, supervision, writing—original draft. S.N.A. carried out supervision and methodology. Y.X.W. was involved in resources, observation, and project administration. Z.E.T. carried out investigation, methodology, and writing—review and editing. S.A.M.L. was involved in data curation and writing—original draft. M.N. took charge of validation and writing—review and editing. P.J. took charge of supervision and methodology.
R.M.P. carried out supervision and methodology. J.L. was in charge of funding acquisition, writing—review and editing, and validation. R.V.C. was in charge of conceptualization, supervision, funding acquisition, writing—review and editing, and validation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.