
Abstract
Purpose:
We report our experience with 100 patients who underwent an innovative prostate enucleation technique that spares the complete urethral—plate from the veru montanum to the bladder neck using a low-energy thulium laser emission. The aim of our study was to evaluate the short-term effects of this procedure on ejaculation preservation and urinary obstruction.
Materials and Methods:
The International Prostate Symptom Index (IPSS), quality of life (QoL), and Male Sexual Health Questionnaire Ejaculatory Dysfunction (MSHQ-EJD) Short Form were used as validated instruments to quantify ejaculatory dysfunction before and 6 months after the surgery.
Results:
The median IPSS score pre- and postoperatively was 20 and 5, respectively (p < 0.0001); QoL dropped from a median of 4–1 (p < 0.0001); and the mean preoperative maximal flow rate improved significantly (8.5 vs 21.2 mL/min) (p < 0.0001). Furthermore, there was significant reduction in postvoid residual postoperatively (p < 0.0001). Postoperative ejaculatory function was preserved in 92/100 patients (92%). According to the MSHQ-EJD score, patients reported a slight nonsignificant decrease in frequency of ejaculation (item 1), force of expulsion (item 2) and reduction in semen volume during ejaculation (item 3), with the exception of ejaculation discomfort (item 4).
Conclusion:
According to our results, complete removal of the apical tissue, which has been advocated as an integral part of the so called ejaculatory hood, does not interfere with ejaculation if the ventral lissosphincter remains intact.
Introduction
Benign prostatic hyperplasia (BPH) is a common condition that affects ∼50% of men older than 50 years of age. Each year, one in 20 of these men experiences progression of symptoms, and one in 100 undergoes surgery for symptomatic relief or BPH complications. 1 The prevalence of ejaculation disorders (EJDs) is ∼70%, with the vast majority of patients losing antegrade ejaculation. 2 This has significant negative effects on the quality of life (QoL), not only regarding orgasmic function but also regarding fertility due to the relatively early onset of BPH. 3 Several studies have investigated the effects of prostatic surgery on sexual function, 4 –6 even if none specifically addressed ejaculation as the primary outcome. Recently, a better understanding of the physiology and mechanisms of ejaculation has resulted in the emergence of modified surgical techniques 7 –9 and therapeutic options 10 –12 that aim to preserve antegrade ejaculation.
We report our experience in 100 patients without significant middle lobe who underwent an innovative Ejaculation-Sparing Transurethral Enucleation of the Prostate with Thulium laser technique using a low-energy laser emission, which spares the entire urethral—plate from the veru montanum to the bladder neck. The aim of our study was to evaluate the short-term effects of the new endoscopic technique on ejaculation preservation as well as obstructive symptoms.
Materials and Methods
Between April 2019 and May 2021, 100 men with BPH were treated with ES-THULEP by a single operator. The exclusion criteria were the following: presence of significant middle lobe enlargement (Intravesical Prostatic Protrusion—IPP index grade >1), history of prostate cancer, urethral stenosis, and previous surgeries of the prostate. All patients were sexually active and with normal ejaculation before starting any alpha-blocker therapy.
Patient demographics, including comorbidities and medications, were noted. The International Prostate Symptom Index (IPSS), QoL, and Male Sexual Health Questionnaire Ejaculatory Dysfunction (MSHQ-EJD) Short Form (abridged version of the 25-point MSHQ focused on ejaculation) were used as validated instruments to quantify EJD before and 6 months after the surgery. 13 Prostate and adenoma volume measured using transrectal ultrasound, serum prostate-specific antigen levels, maximal flow rate (Qmax), and postvoid residual (PVR) were examined preoperatively and 6-months postoperatively.
The baseline patient characteristics are summarized in Table 1. The median age was 64 years (range, 53–71). The mean prostate volume was 55 (range, 33–71) mL. All patients had grade 1 IPP. The mean volume of the adenoma was 36 (range, 20–47) mL.
Baseline Patient Characteristics
BMI = body mass index; EJDs = ejaculation disorders; PSA = prostatic specific antigen; SD = standard deviation.
The operative time, laser energy delivered during surgery, weight of the removed tissue, intraoperative findings, duration of indwelling catheter, and length of hospitalization were also analyzed.
Immediate complications, according to the Clavien classification, 14 were evaluated in the immediate postoperative period and at 1-month postoperative.
The duration of follow-up was 6–19 months (median, 13 months).
The equipment for THULEP included RevoLix 120-W thulium:YAG laser (LISA laser products OHG—Katlenburg-Lindau/Germany) with 800-μm end fire laser fiber and a 26F SHARK continuous-flow resectoscope and 12° telescope (Richard Wolf GmbH, Knittlingen, Germany). Continuous power of 30 W was used in noncontact mode for enucleation, while 5 W was used for hemostasis. The enucleated tissue was removed using a 26F morcescope, in combination with SHARK outer sheaths, 0° telescope (Richard Wolf GmbH), and Piranha system (Richard Wolf GmbH). A 20F Bard three-way drainage catheter with continuous saline irrigation was used until the day after the surgery and, when possible, the catheter was removed on postoperative day 2 and the patient was discharged. All descriptive analyses of pre-, intra-, and postoperative parameters were performed using an independent Student's t-test and chi-square test. A p-value <0.05 was considered statistically significant. All statistical analyses were performed using MedCalc software (Medcalc, Mariakerke, Belgium).
The results are obtained from a retrospective analysis of all data collected prospectively.
Ethical approval was waived by the local Ethics Committee of our institution in view of the retrospective nature of the study and all the procedures being performed were part of the routine care.
Surgical technique
The technique adopted, with a special attention to preserving ejaculatory function, involves the following two steps to improve the ejaculatory outcomes: (1) preservation of bladder neck muscle fibers from the 7 to 5 o’ clock positions; and (2) preservation of the entire posterior urethral plate, from the colliculus seminalis to bladder neck.
The spared rectangular urethral plate started at the bladder neck, which remained untouched ventrally and ended 0.5 cm lateral to the seminal colliculus, including the ejaculatory triangle and the precollicular openings of the prostatic ducts that drain the peripheral part of the prostate glands.
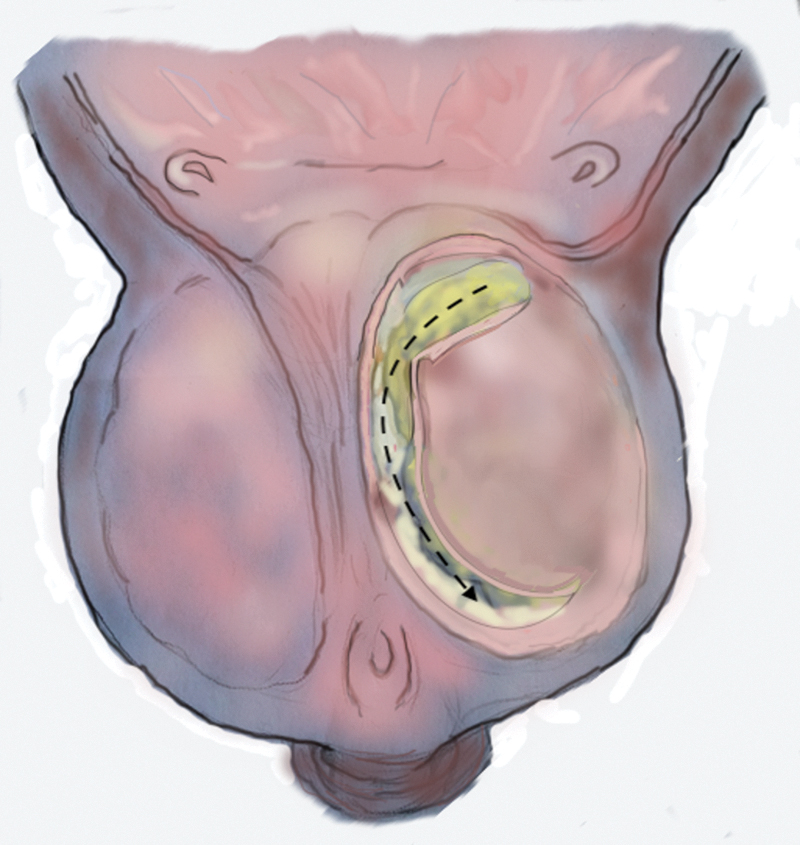
The surgical procedure begins with a dorsal longitudinal incision at the 12 o'clock position from the bladder neck to the opposite side of veru montanum to differentiate the right and left lateral lobes. Subsequently the laser is used to delimitate the urethral plate with an incision starting from the bladder neck at 5 and 7 o'clock positions (Fig. 1), progressing downwards while maintaining a distance of ∼0.5 cm from the lateral urethral folds, and ending bilaterally ∼5 mm lateral to the seminal colliculus (Fig. 2). From there, a semicircular incision of the urethral mucosa covering the apical part of the adenoma is performed bilaterally and deepened to reach the anatomical plane between the prostatic capsule and adenoma (Fig. 3).
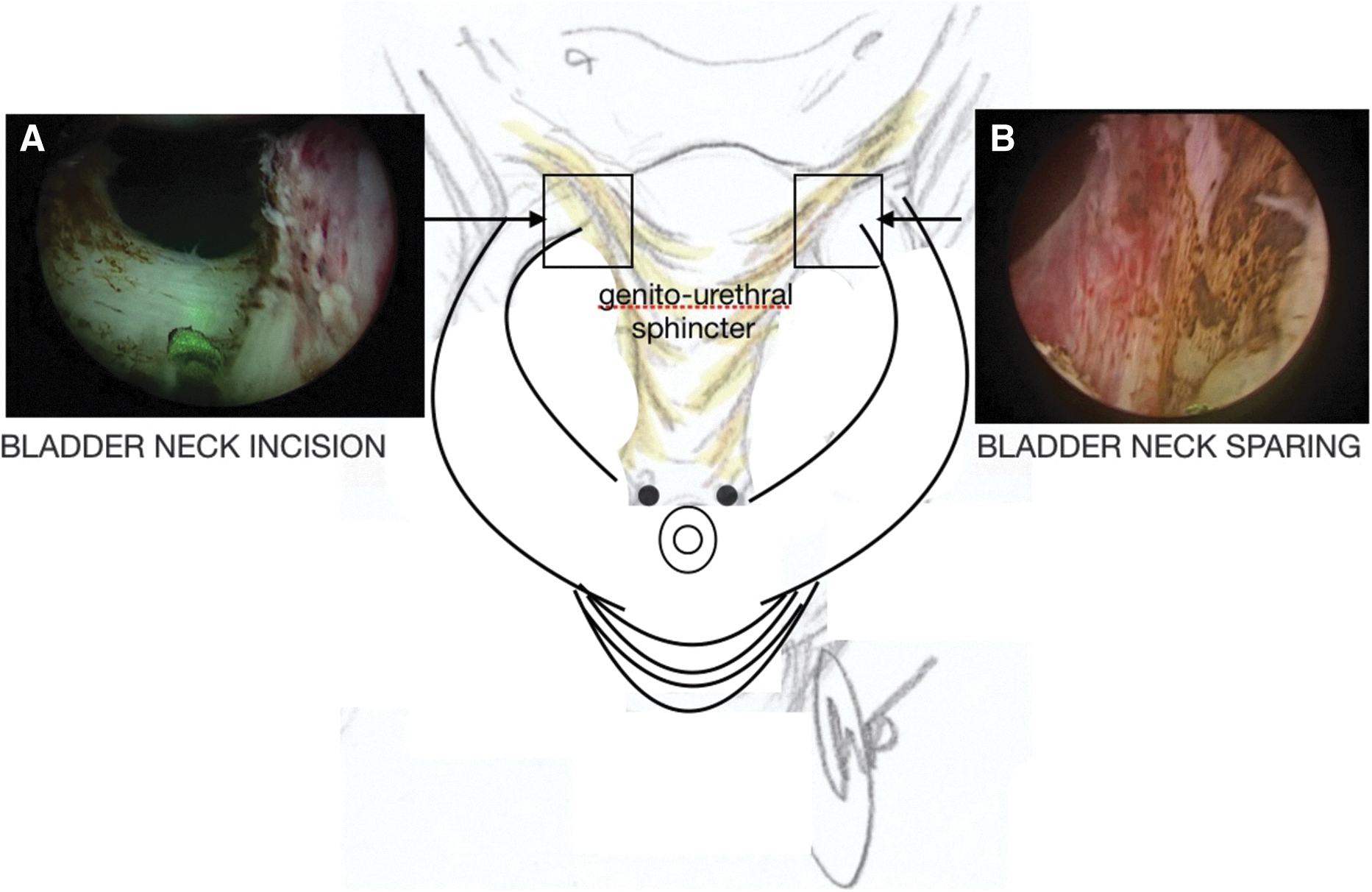
Endoscopic view near the bladder neck:
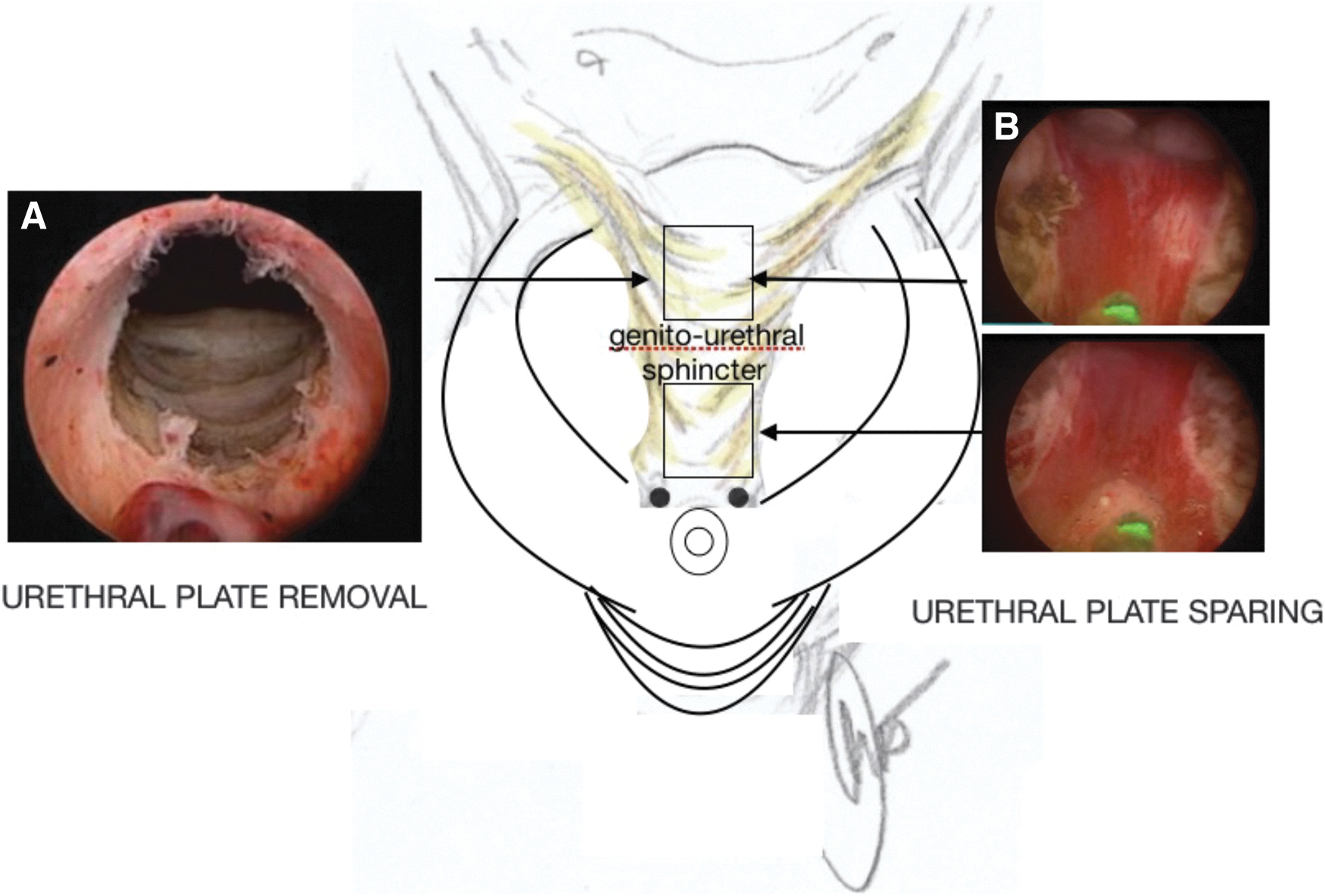
Postoperatively endoscopic view from the colliculus seminalis:

Laser incision starts from the bladder neck at 1 o'clock position, goes down laterally to the ventral prostatic mucosa which is left intact, saving the prostatic lateral groove and ends ∼5 mm laterally to the seminal colliculus, leaving intact the orifices of the peripheral prostate glands (ejaculatory hood saving). The dissection is then deepened to reach the anatomical plane between adenoma and prostatic capsule. Soon after, a semicircular incision of the urethral mucosa covering the apical part of the adenoma is performed and deepened to reach the anatomical plane between apical prostatic capsule and adenoma and extended cranially to realize the rendezvous with the previous lateral incision started from the bladder neck at 3 o'clock position.
Before starting with the enucleation, an oblique laser incision of the mucosa is placed at the level of the bladder neck to save the muscular fibers and directed toward the dorsal 12 o'clock longitudinal incision. After the mucosal release, the laser incision is deepened using blunt dissection and reaching the prostatic capsule to separate the lobe from the bladder neck. The aim of this maneuver is to preserve as much of the smooth muscles as possible that run under the mucosa at the bladder neck (lissosphincter muscle) (Fig. 4).
After the mucosal release, the laser incision is deepened using blunt dissection and reaching the prostatic capsule to enucleate the prostatic lobe.
Returning to the pericollicular area, the lateral lobe was carefully raised and separated from the prostatic capsule using blunt dissection and pushing gently with the metallic sheath and/or using the tip of the laser fiber. Low-power (30 W) was used to release any fibrous bridge of tissue that was encountered. Careful attention was paid during the lateral incision of the urethral plate from the apex to the bladder neck area to spare the lateral urethral mucosal folds, which sometimes contains the ejaculatory orifices, and to keep the margins of the urethral plate intact. Laser enucleation was directed obliquely, from the bladder neck to veru montanum, to reach the capsular plane of each lateral lobe until the entire medial part of the adenoma was detached. Once obtained the respect of the urethral plate, the enucleation was completed, and the prostatic lobe was delivered within the bladder cavity.
Results
Surgical outcomes
The mean weight of the resected tissue was 26.5 (range, 16–34) g. The mean duration of surgery was 67.0 (range, 51–116) minutes, which included a mean duration of enucleation and morcellation of 52.2 (range, 40–90) and 14.7 (range, 11–26) minutes, respectively. It includes the setup of the procedure and at moment does not add time to the mean procedure time. Lateral lobe hypertrophy was slightly prominent in 66/100 (66%) patients, while bladder neck elevation or intravesical prostate protrusion was absent in 34/100 patients (34%). Three patients had bladder stones and 16 patients (16%) had severe trabeculations. Dissection was primarily performed along the surgical plane; however, several patients had ill-defined dissection planes.
The average laser energy was 40.7 (range, 16–73) kJ.
Almost all patients were discharged within 2 days of the surgery. The duration of hospital stay was 2 (range, 2–4) days, and the duration of an indwelling catheter was 2 (range, 2–5) days. There were no major complications according to the modified Clavien classification. One patient developed persistent postoperative bleeding and another sustained mucosal injury during morcellation. The prostatic capsule ruptured in two patients, which resolved following delayed removal of the urethral catheter. No transient urinary incontinence was observed postoperatively and none of the patients complained of significant burning sensation; all had successive micturition. Only two patients who were prescribed new oral anticoagulants at discharge visited the emergency room subsequently for voiding difficulties secondary to persistent hematuria.
Postoperative voiding parameters
The postoperative voiding parameters improved 6 months postoperatively in all patients (Table 2). IPSS score pre- and postprocedure was 20 and 5, respectively (p < 0.0001). QoL score dropped on an average from 4 to 1 (p < 0.0001). The mean preoperative Qmax was 8.5 mL/min, which significantly improved at the final follow-up (21.2 mL/min) (p < 0.0001). As expected, there was a significant reduction in PVR from 117 to 19 mL (p < 0.0001).
Baseline and Postoperative Voiding Parameters
IPSS = International Prostate Symptom Index; PVR = postvoid residual; Qmax = maximal flow rate; QoL = quality of life.
Postoperative ejaculation function
The evaluation of postoperative ejaculatory function demonstrated an overall success rate of 92% (Fig. 5A). Of 100 patients, 68 of them (68%) reported normal antegrade ejaculation and 24 patients (24%) reported diminished ejaculation, while only 8/100 (8%) patients reported that they had no ejaculation. The MSHQ-EJD results, summarized in Figure 5B, show a slight nonsignificant decrease in the items except for ejaculation discomfort (item 4).

Discussion
Retrograde ejaculation is one of the most common complications following BPH surgeries. Surgeons are concerned about this complication when patients are sexually active. Normal ejaculation is a two-stage process based on two different subsequent phases: emission phase 15 –17 and expulsion phase. 18,19
Retrograde passage of semen was presumed to be prevented by reflex closure of the bladder neck. 19 The bladder neck closure mechanism classically was believed as the etiology of retrograde ejaculation following transurethral surgery for BPH.
Multiple reports indicate that bladder neck closure may not be crucial for maintaining antegrade ejaculation. Gil Vernet's group 20 demonstrated the importance of the muscular tissue proximal to and around the veru montanum (the high-pressure ejaculatory zone) for outward ejaculation. Furthermore, patients with retrograde ejaculation following retroperitoneal lymphadenectomy for tumors of the testes have a closed bladder neck, 21,22 and patients may maintain antegrade ejaculation following prostate-sparing cystectomy and neobladder urinary diversion. 23,24
Some reports have highlighted that colliculus seminalis has a major role in semen expulsion, 25 thus, supporting the hypothesis that the preservation of paracollicular tissue is more important than that of the bladder neck toward ejaculation preservation.
Hermabessiere et al. 26 used dynamic transrectal ultrasound following transurethral resection of the prostate and demonstrated that the ejaculate is directly expelled into the inframontanal urethra with a direct closure mechanism of the paracollicular and supracollicular tissue (ejaculatory hood).
Based on these findings, modified techniques have been introduced in BPH surgeries for ejaculation preservation 10 –12 with a reported success rate of up to 96% (range, 80%–96%).
Therefore, we can argue that the internal bladder neck appears to be not crucial for antegrade ejaculation, while the preservation of 1–1.5 cm of supramontanal tissue would not be sufficient for preventing backward flow of seminal fluid if the apical tissue laterally to the colliculus seminalis is not spared. However, the remnants of periapical tissue represent a critical part of the prostate ejaculation-sparing technique because they can result in suboptimal outcomes in terms of obstructive resolution or long-lasting voiding improvement.
Our innovative technique is based, apart from the respect of the bladder neck and the prostatic area around the veru montanum (ejaculatoy hood), on the respect of the so-called “lissosphincter” muscle described by Koraitim, 27 which helps in maintaining continence at rest via contraction of circular muscle fibers, thus, resulting in the closure of the vesical orifice and concentric narrowing of the posterior urethra. The maximum closure may be assumed to be at the level of the vesical orifice, where the lissosphincter is thickest, and in the membranous urethra, where the urethra is narrowest. Contraction of the longitudinal fibers widens the urethra during the evacuation of urine, thus, reducing the angle between the infra- and supramontanal urethra, which is ∼35°.
Complete preservation may not be necessary for continence because passive continence may be accomplished by preserving a minimal length of smooth muscle sphincter postoperatively. This could be the rationale for better continence results following radical prostatectomy in patients with longer membranous urethrae. A video of electroejaculation demonstrated that during ejaculation, the supramontanal urethra becomes shorter, which possibly increases the angle between the two parts of the urethra (supra- and inframontal). This shortening and angle modification close the supramontanal urethra and push the seminal colliculus outside the high-pressure zone. This action appears to be related to the action of the lissosphincter, which, together with the levator ani, bulbocavernous, and internal urethral sphincter, is activated synergistically during ejaculation.
Unfortunately, until now, this synergistic contraction does not explain the differences between the different actions of each muscle. Seminal fluid is projected downward where the urethra responds with ballooning and eliciting the contraction of the bulbocavernous muscle, which initiates the expulsion phase.
In our opinion, and according to our results, the complete removal of the apical tissue, which has been advocated as an integral part of the so-called “ejaculatory hood,” does not interfere with ejaculation if the lissosphincter remains intact. This may account for the good results we observed in terms of urinary flow improvement in our patients along with the maintenance of antegrade ejaculation.
The effects on voiding improvements, as evaluated by IPSS and uroflow, were similar to what has been previously reported with thulium laser enucleation, thus, confirming the efficiency of the enucleation technique.
Furthermore, the low total energy applied to the prostatic tissue may also be responsible for the almost absence of irritative symptoms that have been described in other reports with the use of high-energy output. We believe that 30 W is sufficient to perform safe hemostatic enucleation without the risk of damaging the lissosphincter.
In this pilot study, we excluded patients with a pronounced and enlarged middle lobe; therefore, we may only suggest this technique in patients without significant protrusion of the middle lobe (IPP index > grade 1) and prostates >70 g, although a modification of the technique for these prostates is under evaluation.
The present analysis was not without any limitations. First, ours was not a randomized prospective study, and this infers a selection bias despite our best efforts. Second, there was an initial learning curve for the surgical technique, which improved with time; however, these factors were not a part of our analyses, thus making it impossible to evaluate their effects. Third, the current follow-up period might not be long enough to evaluate the long-term postoperative resolution of obstruction. Nonetheless, the efficacy and feasibility of the technique is demonstrated by the results. However, further follow-up is required to verify the improvements in urinary symptoms, long-lasting duration of ejaculation preservation, feasibility in larger prostates or those with middle lobe enlargements, and the need of repeat surgeries, if any.
Conclusions
The apical remnants of the prostate during enucleation of the prostate may not be crucial if we respect the posterior urethral plate (respecting the lissosphincter action) lays the groundwork of ejaculation preservation without the risk of residual obstruction through the complete removal of the apical part of the adenoma.
Footnotes
Authors' Contributions
R.M.: conceptualization and writing—original draft. F.M.: formal analysis and review and editing (equal). M.B.: software. G.D.R.: resources. M.M.: review and editing. A.G.: conceptualization (supporting) and writing—review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.