
Abstract
Background:
There is a paucity of guidelines for prostate-specific antigen (PSA) monitoring after simple prostatectomy (SP) despite these patients remaining at risk for prostate cancer (PCa). Our objective was to determine if PSA kinetics can be a potential indicator of PCa after SP.
Methods:
A retrospective review was performed of all simple prostatectomies at our institution from 2014 to 2022. All patients who met criteria were included in the study. Relevant clinical variables were collected preoperatively, including PSA value, prostate size, and voiding symptoms. Surgical and urinary function outcomes were analyzed.
Results:
A total of 92 patients were divided into two groups based on malignancy status. Sixty-eight patients did not have PCa, while 24 patients had known PCa before surgery (14) or were diagnosed as having incidental PCa from the pathological specimen (10). Patients with benign prostates had an initial postoperative PSA value of 0.76 ng/mL compared with 1.68 ng/mL for those with cancer (p < 0.01). PSA velocity for the first 24 months after surgery was 0.042 ± 1.61 ng/(mL·year) for the benign cohort compared with 1.29 ± 1.02 ng/(mL·year) for the malignant cohort (p = 0.01). Voiding improvements were noted by objective (postvoid residual and flow rate) and subjective (American Urological Association symptom score and quality of life score) measures in both groups.
Conclusions:
PSA interpretation and monitoring after SP have not been well established. Our study indicates that initial postoperative PSA value and PSA velocity are important indicators of underlying malignancy in patients after SP. Further efforts are needed to establish threshold values and formal guidelines.
Introduction
Men suffering from lower urinary tract symptoms (LUTS) with associated benign prostatic hyperplasia (BPH) have several treatment options, including medical therapy, catheterization, or surgical intervention. According to American Urological Association (AUA) guidelines, simple prostatectomy (SP) may be recommended for men with prostates larger than 80 g. 1 These men with enlarged prostates often have an elevated prostate-specific antigen (PSA) level, which is nonspecific and also a marker of prostate cancer (PCa). 2,3 PSA interpretation in these men is challenging. 4 –10
The surgical pathology from the removed adenoma in SP is insufficient for diagnosing PCa compared with radical prostatectomy, and SP is not an oncological therapy. These patients remain at future risk of cancer, so the ability to risk stratify patients remains a necessity. Currently, the PSA value after SP deemed concerning for malignancy, recommended PSA surveillance, and worrisome PSA trends are yet to be established.
Prior literature on BPH surgery indicates that the initial postoperative PSA level can guide urologists on which patients need to be monitored more closely for malignancy. 11 –13 However, research in pure SP cohorts is limited. Patients who undergo SP have larger prostates than those undergoing transurethral resection of the prostate (TURP) and often (although not always) holmium laser enucleation of the prostate (HoLEP).
The remaining peripheral zone (PZ) from a 100-g prostate is larger than the PZ from a 40-g prostate. Therefore, postoperative PSA findings from other BPH procedures cannot be generalized to this patient population. Particularly for men aged 55 to 69 years who undergo SP, a better understanding of PSA monitoring is of utmost importance.
In this study, we hypothesized that there will be a difference in the PSA trends after SP for patients who have BPH only compared with patients with known or incidentally found PCa.
Methods
A retrospective review was performed of patients who underwent SP at a single institution from 2014 to 2022. The study design was approved by the Institutional Review Board. Both open simple prostatectomy (OSP) and robotic simple prostatectomy (RASP) were included. All men included in the study had documented pre- and postoperative PSA values. Men with biopsy-proven, but untreated, PCa were included in the study, although they were excluded from PSA evaluation if/when they began cancer treatment.
All patients were seen before surgery to capture subjective and objective voiding parameters. History of prostate biopsy, prior PSA tests, known PCa, and other relevant clinical variables were recorded. Patient prostate volume was calculated by MRI, transrectal ultrasound, or CT. Medical treatment of BPH was documented pre- and postoperatively. Patients taking a 5-alpha reductase inhibitor had their PSA value corrected in data analysis according to established standards. 14
Indications for surgery included a markedly enlarged prostate gland (>80 g) and catheter dependence, acute urinary retention, refractory gross hematuria, or intractable LUTS. Prostatic tissues from all procedures were sent for pathological analysis.
Postoperatively, PSA velocity was calculated for patients with at least 2 PSA values within the 24 months after surgery. PSA doubling time was also calculated. 15 Subjective and objective voiding parameters were collected. For patients undergoing further PCa treatment, the treatment course was recorded.
The primary outcome of the study was to compare postoperative PSA levels in patients with BPH vs PCa after SP.
The statistical analysis compared pre- and postsurgical measures within groups as well as differences between benign and malignant groups. Categorical variables were assessed using the chi-square test, and continuous variables were compared using paired and independent t tests or Wilcoxon signed rank test after assessment of data normality using the Shapiro–Wilk test.
Data analysis was performed using Prism—GraphPad, version 9.5.0 (GraphPad Software, Boston, MA).
Results
A total of 141 patients underwent SP during the study period. Of these, 92 patients met inclusion criteria and 49 were excluded due to the absence of both pre- and postoperative PSA data in our records (being a referral center, most of these patients chose long-term follow-up closer to home). Thirty-one patients underwent OSP (34%) and 61 underwent RASP (66%).
Patients were stratified into groups based on malignancy status. Sixty-eight patients did not have PCa, while 24 patients either had known PCa preoperatively (14) or were diagnosed as having PCa as a result of the pathological analysis of tissue from surgery (10). Within the benign group, 51/68 had preoperative PSA levels >4 ng/mL.
Twenty-three patients underwent MRI, 37 underwent biopsy, and 14 underwent both without a diagnosis of PCa. Of the 10 patients with incidentally found PCa, 7 had a PSA level >4 ng/mL. Eight men underwent biopsy (including all 7 with elevated PSA) and 3 underwent MRI. All patients in the known PCa group had biopsy-proven disease before SP.
Patients without PCa had an average age of 70 years and median follow-up of 360 days. These patients had an average prostate size of 151.6 g, preoperative PSA level of 11.4 ng/mL, and PSA density of 0.08 ng/mL 2 . Patients with prostate malignancy had an average age of 70 years with a median follow-up of 305 days. These patients had an average prostate size of 126.4 g (p = 0.08), preoperative PSA level of 13.8 ng/mL (p = 0.32), and PSA density of 0.1 ng/mL 2 (p = 0.04).
Of the 14 patients with known PCa, 5 started androgen deprivation therapy before surgery and were excluded from PSA analysis. There was no difference in PSA values before surgery between patients with known and incidentally discovered malignancy (p = 0.67) (Table 1).
Baseline Patient Characteristics
5-ARI = 5-alpha reductase inhibitor; IQR = interquartile range; PSA = prostate-specific antigen.
Urinary outcomes are shown in Figure 1. A total of 17 patients (25%) required an indwelling catheter and 6 (8.8%) required intermittent catheterization in the benign group. Postoperatively, no patients required either of these adjuncts. The flow rate improved significantly for the first 90 days and was durable over the 1st year. Postvoid residual (PVR) was also significantly improved at both 0 to 3 and 3 to 12 months postoperatively.
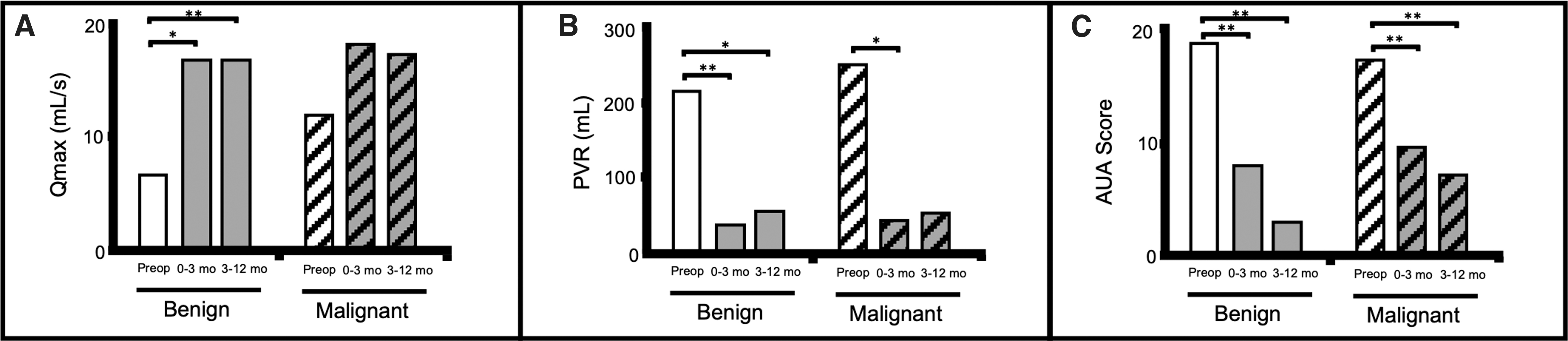
Urinary outcomes. Comparison of
The average AUA symptom score (AUA-SS) before surgery was 19.1 with a quality of life (QoL) index of 3.9. These were both improved after SP. In the malignancy group, 5 patients (20.8%) required a catheter before surgery and 3 (12.5%) required clean intermittent catheterization. After SP, no patients required a catheter. The flow rate improved, although this was not significant.
PVR was significantly improved at 0 to 3 months, although not at 3 to 12 months, after surgery. AUA-SS and QoL score were improved at both time points. Four of 62 patients (6.4%) continued finasteride after surgery in the benign group compared with 1/24 (4.2%) in the malignant group.
Table 2 shows PSA kinetics. The initial postoperative PSA level was significantly lower in the benign group (0.8 vs 1.7 ng/mL, p < 0.01). PSA was reduced by 89.3% in the benign group and 76.6% in the malignant group (p = 0.10). PSA doubling time was 38.4 months for patients with BPH compared with 8.3 months for those with cancer (p = 0.47).
Prostate-Specific Antigen Outcomes and Kinetics
PSA velocity for the first 24 months after surgery showed a 0.04 ng/(mL·year) average increase for the benign cohort, compared with 1.4 ng/(mL·year) in the malignant group (on active surveillance) (p = 0.01). The mean postoperative PSA values were calculated at various time points and compared between the BPH-only and active surveillance groups (Fig. 2).

Comparison of average prostate-specific antigen levels after simple prostatectomy between benign and malignant groups at 0 to 6 months (n = 16 malignant and n = 43 benign), 6 to 12 months (n = 8 malignant and n = 16 benign), and 12 to 24 months (n = 7 malignant and n = 17 benign) postoperatively. *p < 0.05. PSA = prostate-specific antigen.
Significant differences were noted from 0 to 6 months (0.6 ± 0.7 vs 1.2 ± 1.1 ng/mL, p = 0.02), 6 to 12 months (0.6 ± 0.7 vs 1.8 ± 1.3 ng/mL, p = 0.01), and 12 to 24 months (1.0 ± 1.3 vs 3.0 ± 2.3 ng/mL, p = 0.01).
An exploratory analysis was performed that excluded patients with known PCa before SP. In the incidental PCa group, the preoperative PSA level was 14.7 ng/mL with a PSA density of 0.1 ng/mL 2 , neither of which was significantly different from the benign group (p = 0.32 and p = 0.13, respectively). The initial postsurgical PSA level was 1.6 ng/mL, which was higher than in the benign group (p < 0.01).
These patients had a PSA doubling time of 7.75 months (p = 0.55) and PSA velocity of 1.4 ng/(mL·year) (p = 0.04) over the 24 months after surgery.
Discussion
PCa screening after SP can be challenging given the paucity of data on expected PSA characteristics as well as lack of guidelines. These patients remain at risk for future malignancy and a better understanding of this clinical scenario is warranted.
In this study, we compared PSA values after SP between men with BPH only and those with PCa. Our results indicate that the initial postoperative PSA value after SP is elevated for patients with underlying PCa. Furthermore, postoperative PSA velocity is increased in patients with malignancy. Unlike prior studies, the reduction in PSA levels was not significantly different between groups.
Prior literature disagrees on the correlation between preoperative PSA and incidentally discovered PCa. In our study, preoperative PSA alone was not useful to differentiate patients with underlying carcinoma, unlike some prior studies. 16 After surgery, there was a substantial reduction in PSA whether or not a patient had histologic BPH or underlying malignancy (89.3% vs 76.6%, p = 0.10), although this difference was not significant.
As a result, our data also did not support percent reduction in PSA as a means of cancer risk stratification. This contrasts the findings of Elmansy et al. in a post-HoLEP population, who proposed that PSA reduction of less than 50% was indicative of patients who should be followed closely for early detection of PCa. 13 Notably, the preoperative PSA values of our patients were higher than those included in existing analyses, 4,11,13,17 –20 which may have influenced these findings.
Objectively, men with BPH with or without PCa had an improvement in urine flow rate and PVR after surgery. Subjectively, AUA-SS and QoL indices were significantly improved compared with preoperative values in benign and malignant groups. In fact, both AUA-SS and QoL score were improved at 0 to 3 months and continued to improve at 3 to 12 months after surgery.
Improvement in LUTS after SP is consistent with existing literature. 19,21 –23 Our study indicates that this procedure can be a therapeutic option for urinary symptoms in men independent of malignancy status. While SP has been a well-established therapy for BPH, in some instances, it may be a valuable component of therapy for men with PCa to improve urination and QoL scores.
At our institution, SP may be offered to a rare subset of men with PCa; for example, men with marked prostatomegaly with PCa desiring active surveillance or focal therapy with concomitant debilitating LUTS or those patients who refuse radical prostatectomy. In any of these scenarios, shared decision-making is imperative, and these patients meet with urology, medical oncology, and radiation oncology to help navigate their disease.
Perhaps most importantly, our findings suggest that after SP, men with histologic BPH alone have a lower initial postoperative PSA level than patients with PCa (0.8 vs 1.7 ng/mL, p < 0.01). Existing literature has not clearly established an expected or concerning postoperative PSA level after SP. The first data on PSA after SP showed an average PSA value of 1.08 ng/mL in 6 patients with BPH, 3 which has been mirrored by more recent studies. 18,19
Less is known about men with incidentally discovered PCa or who are at higher risk for future PCa. When considering postoperative PSA values, more robust data exist regarding transurethral prostate reduction surgery. In 2000, Wolff and colleagues proposed a PSA value of 2 ng/mL after TURP as a marker for patients at high risk of malignancy. 12 However, when compared with TURP, SP is performed in patients with a larger prostate, presumably leaving a larger residual PZ.
We do not think that findings from TURP literature can be applied to patients after SP. More recently, conflicting data have emerged regarding PSA after prostate enucleation. One study found no difference in PSA levels after HoLEP in 90 patients with or without prostate malignancy. 17 On the other hand, Abedali reports a higher PSA level at first postoperative measurement after HoLEP for patients with incidental PCa (1.6 vs 0.6 ng/mL for the benign group) and recommends prostate biopsy for patients with PSA value >1. 20
Similarly, Lambert and colleagues noted a concerning PSA cutoff value of 1.73 for patients with future PCa risk after HoLEP. 4 While HoLEP and SP use an enucleation plane to debulk the prostate, there are critical differences in surgical approaches and often in preoperative gland sizes. We posit that PSA monitoring after HoLEP may be similar to SP in some patients, but this is not generalizable to all patients undergoing SP. Our study indicates a difference in the initial postoperative PSA values in the malignant and benign groups after SP, although it does not have the power to provide a recommended cutoff value.
Over the 2-year follow-up period, PSA velocity after SP differed between patients with BPH and those with PCa on active surveillance [0.04 vs. 1.4 ng/(mL·year), p = 0.02]. Existing literature on this is conflicted. Marks et al. reported no difference in PSA velocity for patients with stage T1a–T1b disease and BPH after TURP, 24 while more recent data, including SP patients, have suggested that there is indeed a difference and that patients with PSA velocity >0.38 ng/(mL·year) had high specificity for PCa. 11 Our data support PSA velocity as an important indicator and that both initial postoperative PSA value and postoperative PSA velocity after SP can be used to identify higher-risk patients.
Our study is the largest to our knowledge that comprised a cohort of pure simple prostatectomies and compared postsurgical PSA values in patients with benign and malignant pathologies. We feel it is compelling in the quest to provide more formal recommendations on PSA follow-up and management after SP, especially for men aged 55 to 69 years with >10- to 15-year life expectancy and ongoing malignancy risk.
Our study is limited by its retrospective nature, and a larger study is needed to provide definitive PSA cutoff values. Given the wide range of prostate gland sizes in patients who undergo SP (>80 g), a postoperative PSA threshold may ultimately prove difficult to establish. Based on our length of PSA follow-up, we could not extrapolate our findings beyond 24 months.
Future research is warranted to strengthen our findings and further elucidate specific postoperative PSA parameters to guide urologists.
Conclusions
PSA interpretation and monitoring after SP have not been well established. Our study indicates that initial postoperative PSA value and PSA velocity are important indicators of underlying malignancy in patients after SP. Further efforts are needed to establish threshold values and formal guidelines.
Footnotes
Authors' Contributions
All authors listed in this article meet the ICMJE authorship criteria. A.J.L. was involved in conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, and writing—original draft. T.D. was involved in conceptualization, investigation, and writing—review and editing. T.N.M. was involved in conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing—original draft, and supervision.
Author Disclosure Statement
All authors have no financial conflicts of interest to disclose.
Funding Information
No funding was received for this article.