
Abstract
Objective:
We investigated whether pathological outcomes improved with experience and surgeon generation after robot-assisted laparoscopic prostatectomy (RALP).
Materials and Methods:
The study included 1338 patients who underwent RALP between February 2010 and April 2020. We created learning curves for pelvic lymph node dissection (PLND), number of lymph nodes (LNs) removed, and positive surgical margin (PSM) after adjustment for confounders. We compared the outcomes between the first and second generation of surgeons in regression models.
Results:
The learning curve regarding PLND indications showed a significant increase with experience for the first generation, whereas the second generation had a learning curve that remained flat at a higher level (92.3%) and significantly better than the first generation (p < 0.001). Similarly, the number of LN removed showed a significant increase with experience in both generations, but the overall median number of LN removed was significantly higher in the second generation compared with the first generation (12 vs 10, p < 0.001). However, the learning curve for PSM remained flat at ∼20% after adjustment and did not show improvement with experience in both generations of surgeons (p = 0.794).
Conclusions:
Surgeons showed improvement with experience and education with RALP with respect to the indications for PLND and number of LNs removed. However, there was no improvement over time and generations for PSM. Experience based solely on the number of patients operated on is not an intrinsic factor in the pathological quality of RALP. Factors other than experience may also play a role in oncologic improvement.
Introduction
Surgical procedures, particularly radical prostatectomy, require skill and expertise that are acquired with experience. Previous studies of open and laparoscopic surgery have shown that surgeon experience and generation improve perioperative, oncologic, and functional outcomes. 1 –7 The term “experience” is often used to refer to the number of patients operated on. Our aim is to investigate this claim with respect to pathological outcomes after robot-assisted laparoscopic prostatectomy in our tertiary care academic center.
In the context of prostate cancer surgery, we hypothesize that the learning curves for performing pelvic lymph node dissection (PLND), the number of lymph nodes (LNs) removed, and the rate of positive surgical margins (PSMs) improve progressively with surgeon experience until they reach a plateau. We also hypothesize that surgeon generation will impact outcomes, increasing the likelihood of performing PLND, increasing the number of LNs removed, and decreasing the rate of PSM.
Materials and Methods
The retrospective study cohort consisted of 1338 patients who underwent robot-assisted laparoscopic prostatectomy (RALP) between February 2010 and April 2020 at a single tertiary care academic center, Charité University Hospital in Berlin, Germany. Six surgeons performed the operations, three of whom performed RALPs between 2010 and 2014 and the other three between 2015 and 2020. The first-generation surgeons had no prior experience with robot-assisted surgery but had experience with open or conventional laparoscopic radical prostatectomy, whereas the first-generation surgeons for RALP procedures trained the second-generation surgeons. This training took place during their Residency program and more intensively during their Fellowship for 2 years.
All patients gave prospective consent for the recording of preoperative, intraoperative, and postoperative data for retrospective analyses. Institutional Ethics Committee approval was obtained (EA2/022/22).
Preoperative work-up for all patients consisted of a prostate biopsy. MRI scans before surgery were introduced and implemented starting from the year 2014 at our center. All patients who underwent surgery from the second generation onward received an MRI as part of their evaluation. Data collected for each patient included initial prostate-specific antigen (PSA) level, TNM clinical stage, final Gleason score of the prostate specimen, use of a frozen section according to the Neuro-SAFE strategy, 8 completion of PLND, number of LNs removed, and the presence of a PSM. The PLND template followed in this study involved limited dissection of external iliac nodes and obturator fossa for all patients, irrespective of tumor stage or Gleason score.
All patients in the study underwent PLND concurrent with prostatectomy. The surgeries were conducted ∼2 to 3 months after the initial diagnosis for all patients. The time taken to perform the PLND intraoperative was never documented. Dedicated uropathologists analyzed the surgical specimens. In this regard, it is important to mention that as a definition, a PSM in NeuroSAFE analysis is reported when at least one invasive malignant gland comes into contact with the linked surgical margin. 8 The use of Neuro-SAFE in our institution started at the end of 2013.
Statistical analyses
Continuous variables were presented as mean and standard deviation or median (interquartile range), depending on the distribution. Student's t-test or Mann–Whitney U test was used to compare the difference between groups. Categorical variables were presented as frequencies and percentages and compared using the chi-square test.
Learning curves were created for PLND, number of LNs removed, and PSM. Multiple logistic regression models were used to evaluate the association between PLND or PSM and surgical experience (entered as a continuous variable). A linear regression model was performed to assess the association between the number of LNs removed and surgical experience. As the relationship between surgical experience and outcomes is likely nonlinear, surgical experience was modeled using restricted cubic splines with four knots for both models, as mentioned above. 9 Adjustments were made based on the following covariates: preoperative PSA (continuous), pTNM stage (2, 3a, 3b), NeuroSAFE frozen section (yes/no), and Gleason score (continuous). The learning curve for the number of LNs removed was produced by the predicted mean, and the learning curve for PLND and PSM was produced by the predicted probability of PLND and PSM for each level of surgical experience, with all covariates set at the mean. All p-values were two sided, and all statistical tests were performed using Stata IC15 (StataCorp, 2017, College Station, TX).
Results
A total of 1344 patients were included in the study, with 666 (49.5%) operated on by first-generation surgeons and 678 (50.5%) operated on by second-generation surgeons. The three first-generation surgeons operated on 347, 242, and 77 patients, respectively, whereas the three second-generation surgeons operated on 541, 74, and 63 patients, respectively. Table 1 shows the clinical and pathological characteristics of the study cohort. A multivariable prespecified model was used to control case mix by adjusting for clinical and pathological variables.
Patients' Clinical Characteristics According to Surgeon's Generation
IQR = interquartile range; LN = lymph node; PLND = pelvic lymph node dissection; PSA = prostate-specific antigen; PSM = positive surgical margin; TNM = tumor, nodes, metastasis (globally recognised classifications of malignancies).
Initial PSA and pathological stage did not differ significantly between the two generations. However, the Gleason score of specimens operated on by first-generation surgeons was statistically higher compared with second-generation surgeons (p < 0.001).
Initial descriptive analysis showed that PLND was performed in 1027 patients (76.4%). PLND was performed in 401 (60.2%) of the 666 patients operated on by first-generation surgeons and in 626 (92.3%) of the 678 patients operated on by second-generation surgeons (Fig. 1; p < 0.0019). A statistically significant improvement in the number of PLNDs performed was observed during the experience of first-generation surgeons. In comparison, second-generation surgeons had a flat learning curve during their experience and overall performed at a significantly higher level than the first generation (Fig. 2; p < 0.001).
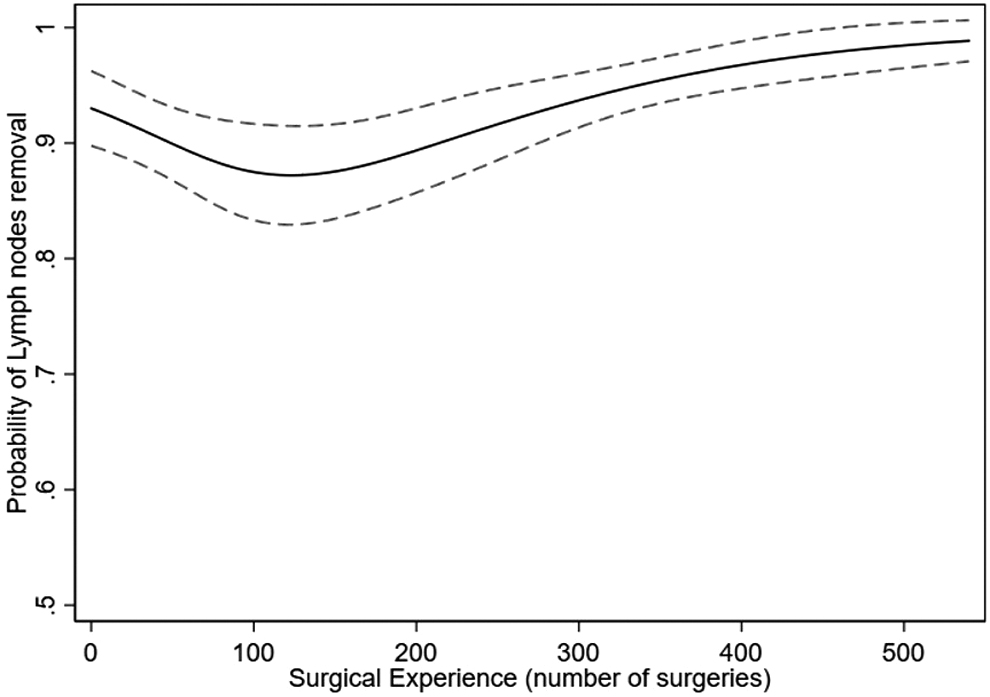
Overall learning curve for pelvic lymph node dissection performed, controlling for PSA, pathological stage, frozen section, and Gleason score. Predicted probability (solid line) and 95% confidence intervals (dashed line) are plotted against increasing surgeon experience. PSA = prostate-specific antigen.
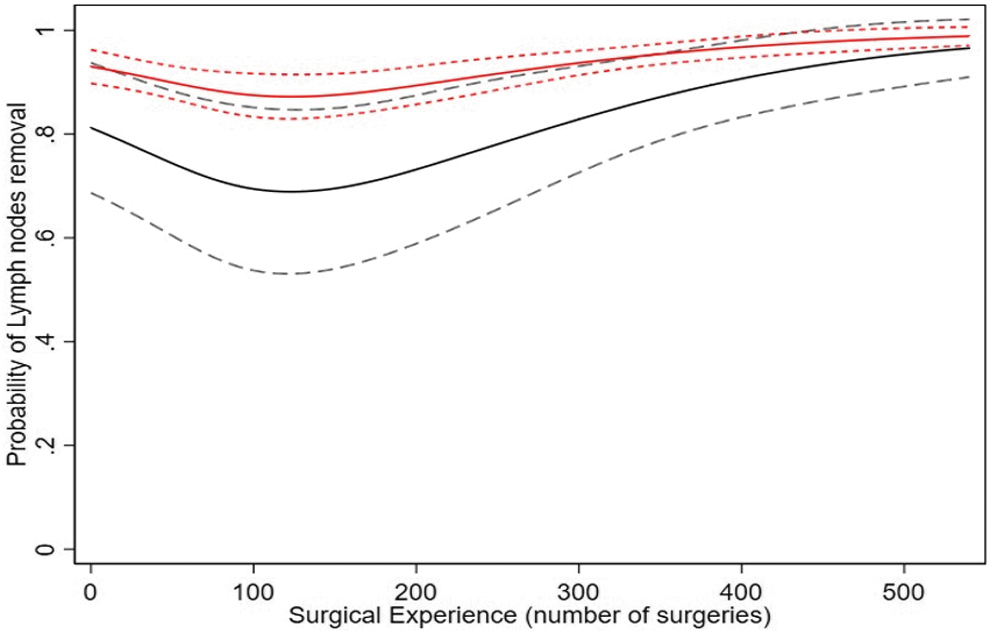
Learning curve for pelvic lymph node dissection performed according to surgeons' generation, controlling for PSA, pathological stage, frozen section, and Gleason score. Predicted probability (solid line) and 95% confidence intervals (dashed line) are plotted against increasing surgeon experience: first-generation surgeon (black lines) vs second-generation surgeon (red lines).
Similarly, the number of LNs removed increased significantly with experience (Fig. 3). In addition, the median number of LNs removed was significantly higher in second-generation surgeons than in first-generation surgeons (Fig. 4; 12 vs 10, p < 0.001).
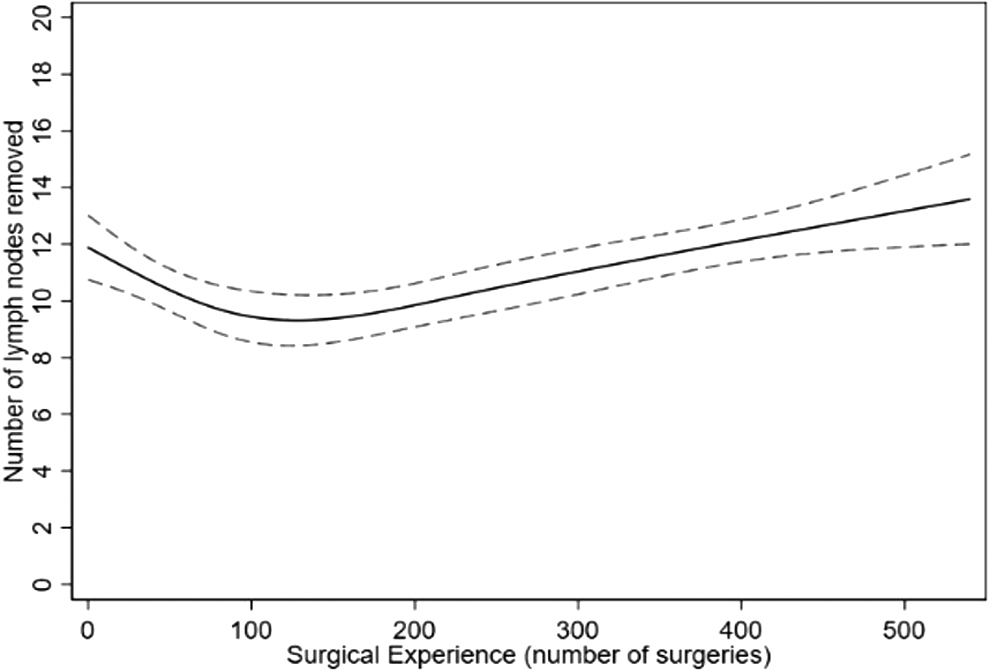
Overall learning curve for number of lymph nodes removed, controlling for PSA, pathological stage, frozen section, and Gleason score. Predicted probability (solid line) and 95% confidence intervals (dashed line) are plotted against increasing surgeon experience.
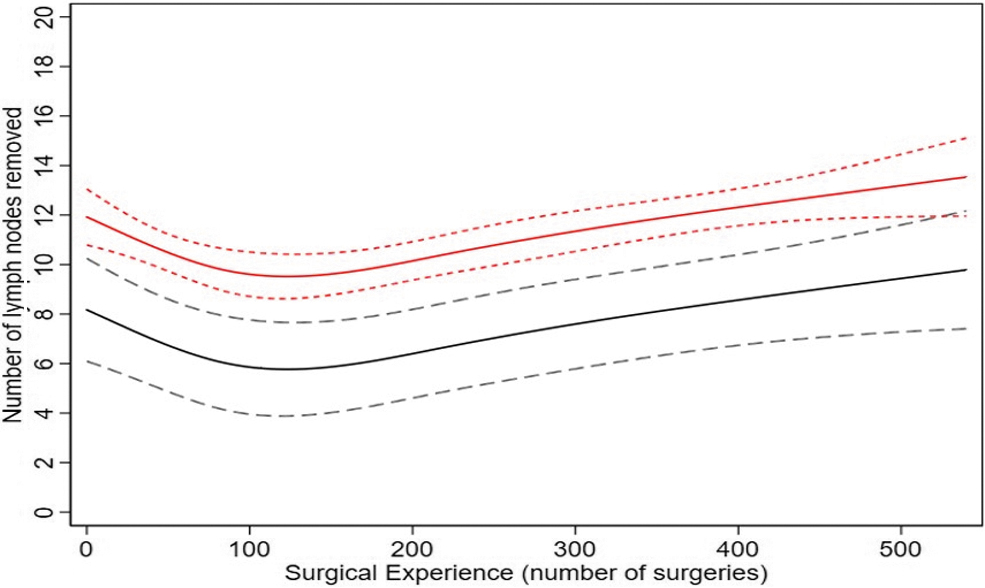
Learning curve for number of lymph nodes removed according to surgeons' generation, controlling for PSA, pathological stage, frozen section, and Gleason score. Predicted probability (solid line) and 95% confidence intervals (dashed line) are plotted against increasing surgeon experience: first-generation surgeon (black lines) vs second-generation surgeon (red lines).
PSMs were reported in 390 patients (PSM rate: 29%). The first-generation surgeons reported a PSM in 225 patients (33.8%), whereas second-generation surgeons reported a PSM in 165 patients (24.3%). After adjustment for PSA, pathological stage, frozen section, and Gleason score, there was no difference in the learning curve for PSM between the two generations (Fig. 5; p = 0.79). The learning curves after adjustment were flat, with a PSM rate of ∼20% in both generations of surgeons and showed no improvement with experience (Fig. 6).
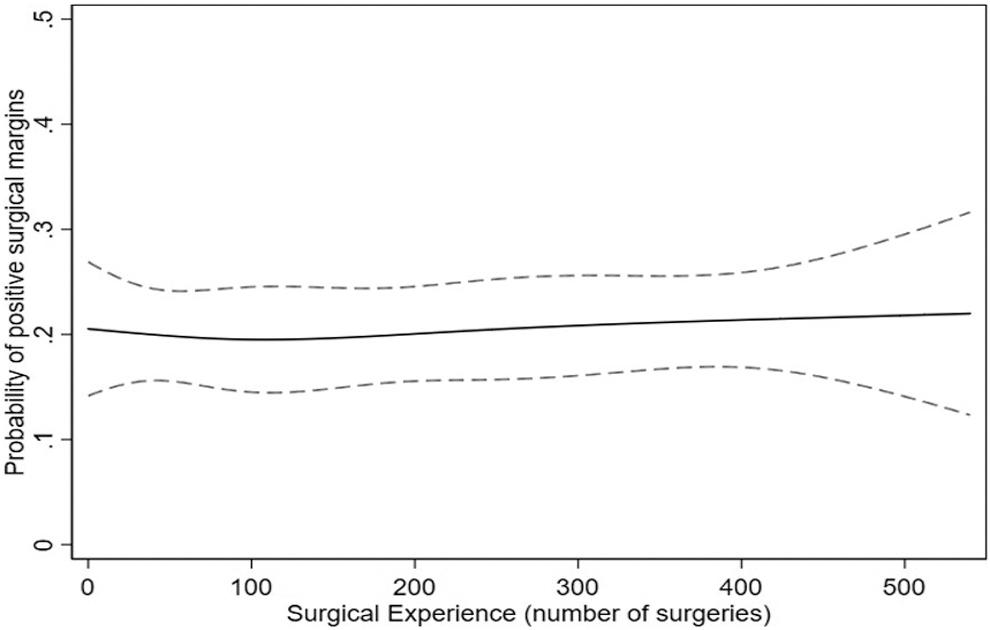
Overall learning curve for PSMs. Predicted probability (solid line) and 95% confidence intervals (dashed line) for PSM, controlling for PSA, pathological stage, frozen section, and Gleason score, are plotted against increasing surgeon experience. PSM = positive surgical margin.
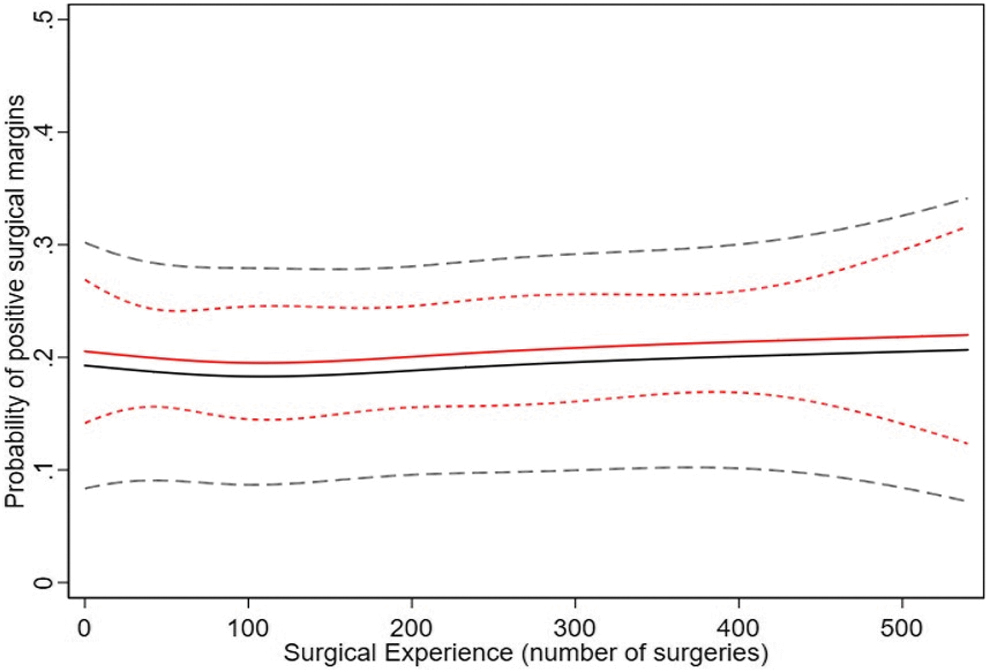
Learning curve for PSMs according to surgeons' generation. Predicted probability (solid line) and 95% confidence intervals (dashed line) for PSM, controlling for PSA, pathological stage, frozen section, and Gleason score, are plotted against increasing surgeon experience: first-generation surgeon (black lines) vs second-generation surgeon (red lines).
Discussion
It is commonly believed that a surgeon with extensive surgical experience will deliver good results to their patients. This often translates into inquiries from patients about the number of procedures a surgeon has performed. Previous studies have shown that in radical prostatectomy, regardless of surgical approach (open, conventional, or robot-assisted laparoscopic), perioperative, oncologic, and functional outcomes improve with surgeon experience and generation. 1 –7,10,11 Similar findings have been reported for other urologic cancer surgeries such as radical cystectomy. 12,13
In this study, we sought to evaluate the statement of robot-assisted radical prostatectomy, which was implemented relatively recently, in 2010, and has since expanded in our tertiary care academic hospital, thus providing a good model for such an evaluation. We analyzed the learning curve of performing PLND as well as the number of LNs removed, which may serve as a good indicator of surgical proficiency. However, this parameter is rarely studied and may be confounded by other factors other than surgical performance, such as the extent of the preoperative work-up. In our study, both learning curves showed improvement over time with an initial decline and over generations of surgeons, in line with previous studies. 14,15 Regarding the decision to perform PLND, we can assume that inexperienced surgeons initially focus on performing radical prostatectomy as the primary goal. As they gain experience and operative times decrease, we assume that the time saved is devoted to PLND.
As reported by Hu and colleagues, 14 the number of removed LNs increases with surgeon's experience. This can be explained by the reduction in operative time, and by the fact that the number of nodes is an easily memorized parameter that can be easily incorporated into a personal surgical assessment. In both generations, the number of LN was first reduced at the beginning of the experience and then increased throughout the experience, with a plateau reached after 200 to 250 operated patients. The fact that the number of PLNDs performed and the LN count started at a higher level for the second generation than for the first may be interpreted as a good transfer of knowledge between the generations of surgeons in the frame of the internal educational program.
Many previous studies have examined the rate of PSM and biochemical recurrence after radical prostatectomy. 1 –7,11,16 –19 Most have suggested that PSM rate improved with surgeon or institutional experience, underlying the overall progress made through teaching processes and accumulated experience. However, the volume of experience required varied across studies, whether it was a single surgeon, 20 a single surgical group, 2,21 or a multi-institutional study, 1,6,18 and the technique used. 3,5,7 Robot-assisted radical prostatectomy has an indeterminate learning curve, and the shape of the curves varies depending on the parameter selected, such as operative time, transfusion rate, complications, or hospital stay, among others.
For PSM, the volume is not clearly defined, and a recent study suggested that an experience of up to 1600 patients would be required to reach a PSM rate of <10%, and that for pT3 tumors, the curve begins to plateau after 1000 to 1500 cases. 18 In our study, surgeons failed to demonstrate an improvement regarding PSM over time and generations. Different surgeons with the same experience showed differences in PSM rates, suggesting that they tend to repeat the same mistakes throughout the procedures.
Analyzing the data, we observed that patients with T3 disease who did not undergo NeuroSAFE did not benefit from nerve sparing, particularly when advanced abnormalities were detected on MRI. However, nerve sparing was selectively performed for T3 tumors only if there was no obvious nerve invasion on MRI images and when NeuroSAFE results were negative. Therefore, we conclude that nerve sparing was not a confounding factor in this particular cohort.
An important aspect to consider in the preoperative assessment is the inclusion of MRI scans, which could potentially have an impact on the results between the first and second generations. However, despite the utilization of MRI, the results did not show any improvement in PSM rates. This suggests that surgeons may rely more on the NeuroSAFE technique rather than solely on MRI findings. It is important to note that NeuroSAFE focuses on the bilateral peripheral layers of the prostate and does not encompass all aspects of the organ.
Our study demonstrates that “surgical experience,” based solely on the number of patients operated on, is not an adequate proxy for oncologic quality. Other factors should play a role in oncological improvement. This raises the question of whether a structured curriculum is an important predictive factor of quality, as suggested by Secin et al. 6 and Vickers et al. 7 In addition, “Quality Assurance” concepts may be a key quality factor, as surgical improvement is a continuous process based on learning from previous successes and mistakes, properly analyzed and interpreted.
Another important point to discuss is how surgical and oncologic outcomes improve with generations. When comparing the probability of LN dissection and number of LNs removed, the second generation performed significantly better and immediately higher at the beginning of the experience. This is probably related to the experience the second generation gained when assisting the previous generations. However, assessing its own progresses when comparing continuous numbers, such as number of removed nodes, this method of self-evaluation is not suitable for complex assessments, such as the status of surgical margins in relation to anatomic and pathological complexities.
The main limitation of our study is its single-center retrospective design, but it reflects daily practice in a real-world setting. Our objective was to examine whether the outcomes at a large center are primarily influenced by the volume of cases, particularly concerning PSMs and LN dissection. It was not our intention to generalize these findings to other centers performing robotic prostatectomy. However, this could still be the case at any center performing robotic prostatectomy in high volumes. The main value is that all surgeons performing RALP and all patients without any selection or exclusion were included, and only dedicated uropathologists analyzed all specimens, which eliminates pathological bias. These data are based on pathological findings only and not on long-term biochemical results that could theoretically lead to differences in oncologic outcomes, although it is well documented that pathological and biochemical findings are highly correlated. 17
Conclusions
With experience and training, surgeons have improved their ability to perform robot-assisted radical prostatectomy, including determining when to perform PLND and increasing the number of LNs removed. However, there has been no improvement in reducing the incidence of PSMs over time and across generations.
Based on these results, we conclude that using the number of patients operated on as the sole metric for assessing the pathological quality after robot-assisted laparoscopic prostatectomy is inadequate. Other factors may also play an important role in achieving better oncologic outcomes. To ensure and validate ongoing surgical improvements, we recommend structured training programs and the implementation of quality assurance processes.
Footnotes
Authors' Contributions
T.A.: Conceptualization, Methodology, and investigation.
P.G.: Statistical analysis.
S.E.: Analysis and interpretation of data.
F.R.: Analysis and interpretation of data.
B.R.: Critical revision of the article.
S.W.: Critical revision of the article.
D.M.: Analysis and interpretation of data.
T.S.: Conceptualization and critical revision of the article.
B.G.: Supervision, Conceptualization, Methodology, and investigation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.