
Abstract
Background:
Several studies have reported on the safety and feasibility of percutaneous nephrolithotomy (PCNL) under local anesthesia (LA). The aim of this systematic review is to assess the perioperative outcomes of PCNL under LA.
Methods:
Three electronic databases, including MEDLINE, EMBASE, and Web of Science, were searched for relevant English-language studies published from January 1980 to March 2023. The systematic review has been performed according to the Cochrane style and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis. The primary outcomes include stone-free rate (SFR) and conversion to general anesthesia (GA). Secondary outcomes include postoperative complications.
Results:
Of 301 articles that were extracted, 42 full-text articles were selected, of which 36 were excluded, yielding a total of 6 articles in our results. A total of 3646 patients were included in this review. The SFR of PCNL under LA ranged between 69.9% and 93.3%. PCNL under LA was not tolerated by 19 (0.5%) patients: 6 patients had conversion to general anesthesia, 2 had conversion to epidural anesthesia, and 11 had their procedure terminated. The overall complication rates varied from 4.8% to 21% across studies. Grade I–II complications were reported in 2.4%–16.7% of cases, while grade III–IV complications were encountered in 0.5%–5% of patients.
Conclusions:
In this review, we found a few studies that examined the outcomes of PCNL under LA, which highlight the feasibility and safety of PCNL under LA and the low conversion rate to GA.
Introduction
Percutaneous nephrolithotomy (PCNL) is considered a first-choice treatment for large renal stones (>2 cm) as it offers the best stone-free rate (SFR) compared with other modalities such as shock wave lithotripsy and retrograde intrarenal surgery (RIRS). 1 PCNL is associated with postoperative complications that are more pronounced in frail and morbidly obese patients and patients with advanced chronic obstructive pulmonary disease (COPD). 2 –4
PCNL is usually performed under general anesthesia (GA) due to pain and the perceived risks of sudden patient movements, resulting in kidney parenchyma injury or pelvicaliceal system perforation; better control of breathing; and better tolerability for patients. 5,6 The disadvantages of GA are associated with pulmonary, vascular, and neurologic systems—problems associated with electrolyte balance and the endotracheal tube especially during the change of position from lithotomy to prone. 5
Moreover, there are no robust data to support conservative management of staghorn stones. 7 Therefore, several efforts have been attempted to explore the safety and feasibility of PCNL under local anesthesia (LA), where the side effects of GA itself might affect the outcomes of the surgery, such as in frail patients, elderly patients, and patients with severe COPD. In 2011, Chen et al. reported their early experience of PCNL under LA. 8 Subsequently, larger studies utilizing different mixtures of LA anesthesia have evaluated SFRs and the tolerability of the procedure. 9 –11
The aim of this systematic review is to assess the outcomes of PCNL under LA. The primary outcomes include SFR and conversion to GA. Secondary outcomes include operative time and complications.
Methods
Evidence acquisition: criteria for considering studies
Inclusion criteria
All studies reporting on PCNL for kidney stone disease, performed under LA with or without sedation.
Studies in the English language reporting on a minimum of 20 patients.
Patients of all age groups.
Exclusion criteria
Animal studies, case reports, and laboratory studies.
Studies of PCNL under GA or neuraxial anesthesia, where data on LA could not be separated for those who underwent general or neuraxial anesthesia.
Studies examining PCNL for nonurolithiasis conditions or ureteral stones.
Studies on PCNL under LA using a previously established tract.
Studies using the same data as a more recent study, where the longest follow-up or largest number of patients were included.
Studies that explicitly did not report SFRs.
Search strategy and study selection
The present systematic review has been performed according to the Cochrane style and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis. Bibliographic databases, namely MEDLINE, EMBASE, and Web of Science, were searched for relevant English-language studies published from January 1980 to March 2023.
The search terms included combinations of “local,” “regional,” “locoregional,” “loco-regional,” “nerve” with “anesthesia,” “anesthesia,” “analgesia,” “block” and “PCNL,” “percutaneous nephrolithotomy,” “percutaneous nephrolithotomy,” “percutaneous nephrolithotripsy,” “percutaneous stone lithotripsy,” “ECIRS,” “endoscopic combined intrarenal surgery,” “miniPCNL,” “mini-PCNL,” “microPCNL,” and “micro-PCNL.” Boolean operators (AND, OR) were used to refine the search.
Filters were applied as appropriate in each search engine to include only human subject studies and articles in English and exclude conference abstracts. A chain search of the references of all included articles was done to identify further relevant articles. Authors of individual studies were contacted if data were unclear or unavailable. A cutoff of 20 patients was decided to include centers with minimum endourological experience in this procedure.
Two reviewers (M.S. and A.F.) independently identified all the studies that fit the inclusion criteria, and discrepancies were resolved after consultation with the senior author (B.K.S.).
Level of evidence, data extraction, and analysis
The levels of evidence and grades of recommendation were assigned according to the Centre for Evidence-Based Medicine (CEBM) guidelines. 12 The following variables were extracted from the studies: the year of publication, country, study type, total number of patients, number of subjects in each arm if applicable, patient age, gender, body mass index, American Society of Anesthesiologists (ASA) score, presence of complete or incomplete staghorn stones, type of LA used, use of sedation, conversion to GA, patient position, and access type (ultrasound [US] vs fluoroscopic vs endoscopic guidance).
These data were collated using Microsoft Excel (version 12.2.4). Because of the heterogeneity of data, a meta-analysis could not be performed and a narrative synthesis was therefore carried out.
Results
Following our search criteria, 301 articles were extracted, of which 131 articles were excluded as they were duplicates and 128 were excluded by title and abstract screening. The remaining 42 full-text articles were reviewed, of which 36 were excluded, yielding a total of 6 articles in our results (Fig. 1, Table 1).
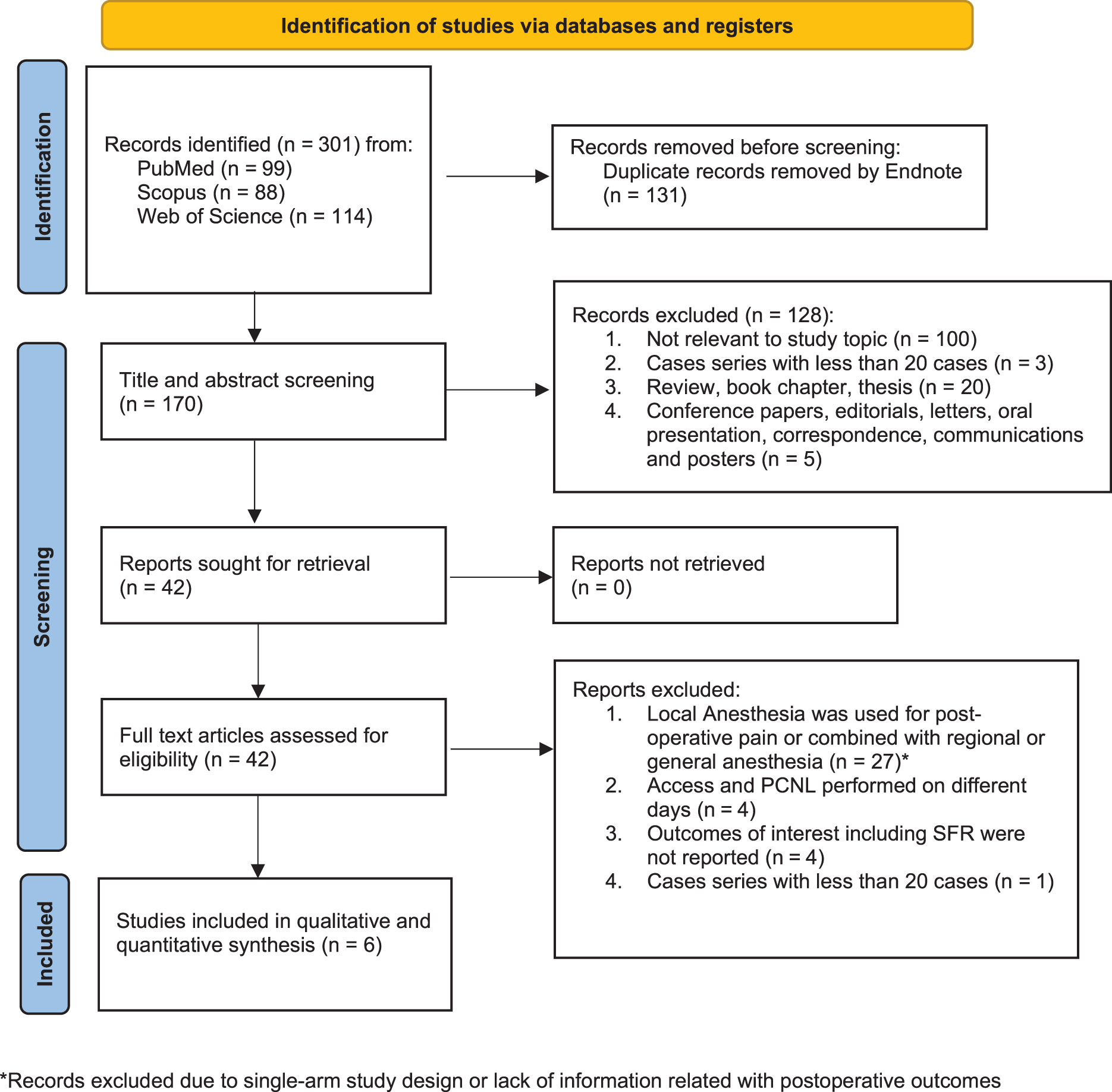
Evidence acquisition flow chart.
Study Characteristics and Demographic Information
BMI = body mass index; IQR = interquartile range; SD = standard deviation.
This review includes one randomized control trial, one prospective study, and four retrospective studies. None of the studies reported power or sample size calculations (Tables 1 and 2). The number of patients included were 3646 (Tables 1 –3). Study characteristics and demographic data are found in Table 1.
Access, Fragmentation Device, and Exit Strategy in the Included Studies
Procedural Outcomes in the Reported Studies
AV = arteriovenous fistula; LOS = length of stay; SFR = stone-free rate; UTI = urinary tract infection.
Use of LA in PCNL
The procedure starts with infiltration of the skin with LA. Thereafter, using a spinal needle (some authors utilize US guidance), the muscle and perirenal capsule are infiltrated with LA. 8 –11,13,14 A variety of LA mixtures were used, but most studies relied on lidocaine as the main component of the anesthetic mixture. Five of six studies reported on the use of intravenous (IV) sedation as an adjunct to LA (Table 4).
Intraoperative Anesthesia Used and Pain Control
GA = general anesthesia; IV = intravenous; LA = local anesthesia; US = ultrasound; VAS = visual analog scale.
Surgical procedure
Position
The most frequent position used during PCNL under LA was the prone position, followed by the lateral position. 8 –11,14 El-Shaer and colleagues reported on the outcomes of PCNL under LA using the modified supine Valdivia position. 13 None of the included studies examined the feasibility and safety of performing PCNL under LA in the supine position.
Access type
US guidance was used in four studies and two reported using a combination of US and fluoroscopy. 8 –11,13,14
Sheath size
Three studies used a standard access sheath (≥22F) and three used a miniaccess sheath (14–20F). None of the procedures were performed using ultramini- or micro-PCNL. 8 –11,13,14
Number of tracts
Most of the patients included in this review were treated with single-tract access. However, several authors reported on the use of multiple tracts (as many as five tracts) to complete the procedure without the need for additional anesthesia. 8 –11,13,14
Subcostal vs intercostal vs supracostal access
A substantial number of cases were completed using subcostal access; however, supracostal access was obtained in selected cases to perform PCNL under LA without increasing the complication rate or the need to convert to GA. 8–9,11
Lithotripter
A combination of pneumatic and ultrasonic lithotripter and laser was used for PCNL under LA. There was no clear contraindication to the use of any lithotripter under LA. 8 –11,13,14
Standard vs tubeless vs totally tubeless
While five of the six studies relied on the use of a nephrostomy tube after PCNL, Yu and colleagues used vacuum-assisted sheaths and reported that 66.7% of their procedures were tubeless. 14 On the other hand, none of the reported cohorts were totally tubeless (Table 1). 8 –11,13,14
Perioperative outcomes
Stone-free rate
The SFR of PCNL under LA ranged between 69.9% and 93.3% (Table 2). The need for a second-look PCNL or an auxiliary procedure to treat residual stones was reported by two studies, which ranged between 6.7% and 29.5%. 8 –11,13,14
Postoperative complications
Most of the studies used Clavien-Dindo classification to report postoperative complications. The overall complication rates varied from 4.8% to 21% across studies. Grade I–II complications were reported in 2.4%–16.7% of patients, while grade III–IV complications were encountered in 0.5%–5% of patients. There were no reported perioperative mortality rates. The reported blood transfusion (1 unit or more) rates ranged between 0% and 3.5% (Table 2). 8 –11,13,14
Operative time and length of stay
The operative time of PCNL under LA ranged between 42 and 89 minutes; however, it was not clear if this included time from anesthesia induction to establishing the PCNL tract. 8 –11,13,14 Only four studies reported on length of stay (LOS), which varied between 1.5 and 5 days.
Postoperative pain
Several studies used the visual analog scale (VAS) to assess intraoperative pain during the procedure. 8 –11,13,14 The mean intraoperative VAS ranged between 3.1 and 3.9. PCNL under LA was not tolerated by 19 (0.5%) patients: 6 patients had conversion to general anesthesia, 2 had conversion to epidural anesthesia, and 11 had their procedure terminated. Complete anesthetic and intraoperative pain control details are found in Table 4.
Discussion
Our systematic review is the first article reporting on outcomes of PCNL performed under LA. We identified six articles that described the outcomes of PCNL under LA. 8 –11,13,14 The SFR ranged from 69.9% to 93%. On the other hand, postoperative complication rates ranged between 2.4% and 16.7% for grade I–II complications and 0.5% and 5% for grade III–IV complications.
Most of the studies included patients with ASA score ≤3; only two studies that assessed the feasibility of PCNL under LA included patients with ASA grade. 4,10,11 Treatment of staghorn stones in highly comorbid and frail patients is a controversial issue among endourologists. While conservative management of staghorn stones might be an option in a select group of patients, staged flexible ureteroscopy has been described to treat staghorn stones in high-risk patients. 7,15
Nevertheless, with the increase in collective experience in performing PCNL, across the globe, there are emerging data showing the safety and feasibility of PCNL under LA, which might be an underutilized treatment modality for these patients.
In a prospective randomized study, there were no significant differences in operative times, LOSs, SFRs, or complication rates of PCNL performed under spinal anesthesia compared with PCNL performed under LA. 13 While the spinal anesthesia group reported less pain during the surgery compared with the LA group, the latter group had lower postoperative pain at 6 and 12 hours after surgery. In another study, Wang and colleagues compared the outcomes of PCNL under GA and LA and found no significant differences in operative times, LOSs, SFRs, or complication rates of PCNL. 16
Of the 3646 patients included in this review, 8 patients required conversion to another anesthesia modality and 11 cases were terminated due to intraoperative chills. 8 –11,13,14 This low conversion rate is consistent with what has been previously reported for RIRS procedures under LA. In addition, 17 it emphasizes the importance of pre-op counseling of the patient to manage their intraoperative expectations.
There is increasing evidence that elderly patients might benefit from avoiding exposure to GA as it is linked to an increase in the risk of cognitive dysfunction and metabolic derangements. 18 For example, Balentine and his colleagues utilized the American College of Surgeons National Surgical Quality Improvement Project to compare the perioperative outcomes of elective inguinal hernia repair under local or GA in elderly patients.
They found that elective inguinal hernia repair under LA was associated with a reduction in postoperative complications in patients aged 75+ years (95% CI −0.11 to −1.13) as well as shortened operative time in patients <75 years. 19 In addition, they projected national cost savings for greater use of LA, ranging from $9 million to $45 million annually. 19
The American College of Surgeons and the American Geriatrics Society recommendations for the care of elderly encouraged surgeons from all subspecialities to identify procedures where avoidance of GA might be linked to improved perioperative outcomes. 20 While data on PCNL under LA are scarce, this comprehensive review highlights the feasibility and safety of PCNL under LA.
However, we failed to identify ideal candidates for PCNL under LA. This is due to lack of an explicit objective description of patients' comorbidities and stone complexity using validated scores such as the Charlson Comorbidity Index and Guy's stone score. 21,22 Moreover, the lack of data on stone complexity hindered our efforts to conduct a meaningful comparison of different perioperative outcomes and SFRs between different modalities of anesthesia used during PCNL.
Furthermore, the coronavirus disease 2019 pandemic has changed surgical practice in large parts of the world, with emphasis on shifting toward outpatient/ambulatory surgeries for different conditions. 22 In concert with these changes, the burden of stone disease and cost of treatment is on the rise. 23 Therefore, there has been heightened interest in exploring the safety and feasibility of ambulatory PCNL to mitigate the cost of PCNL as well as increase patient access to this procedure. 22
While LA ureteroscopy has been well described, the use of LA as an alternative for GA in PCNL procedures might also help hasten the process of establishing the ambulatory PCNL pathway. 17
Future directions
In this review, we found a few studies that examined the feasibility and outcomes of PCNL under LA. There is a need for clinical trials comparing the safety and effectiveness of PCNL under LA and other different regional anesthetic techniques that emphasize including enhanced recovery after surgery protocols as an integral part of the study design.
Moreover, these trials should report on stone complexity, perioperative comorbidity, and frailty using validated scores and tools. 24,25 In addition, efforts are needed to identify novel outcome measures such as patient mobility, functional recovery, and inflammatory biomarkers.
Future studies should focus on determining the proper dose and type of local anesthetic used in PCNL and identification of a suitable patient population for these procedures.
Footnotes
Authors' Contributions
M.S. was involved in article writing, data collection, and data interpretation. A.F. was involved in article writing and data collection. P.M. and S.P. were involved in article editing and project supervision. B.S. was involved in concept and design of the study, article editing, and project supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.