
Abstract
Background:
Numerous continence-sparing radical prostatectomy techniques have been developed to enhance postoperative early continence (EC) recovery; however, evidence regarding the best approach remains controversial. The objectives are to provide a critical appraisal of various prostatectomy techniques, based on the evidence of quality-assessed randomized control trials (RCTs); to summarize the immediate continence and the EC reported; and to propose a new standardization for continence outcomes reporting.
Methods:
Data acquired from five medical registries were reported to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards. Evidence from published, English, full-text RCTs reporting postoperative urinary continence outcomes within 6 months from surgery was included. The heterogeneity of surgical techniques and continence definitions did not allow a meta-analysis. All RCTs were critically appraised, and quality assessed.
Results:
In total, 39 RCTs were included: 19 of 39 studies were low-quality RCTs, presenting small cohort, monocentric, or single-surgeon data. The best RCT-supported evidence is in favor of robot-assisted radical prostatectomy (RARP) compared with laparoscopic radical prostatectomy (LRP) and of the Retzius-sparing (RS) technique over the traditional prostatectomy. Other techniques such as bladder neck and puboprostatic ligament (PPL) preservation, posterior reconstruction with or without combination of anterior suspension technique, and nerve-sparing (NS) approach seem to enhance EC. Oppositely, the endopelvic fascia preservation, bladder neck mucosa eversion/plication/slings, and the selective ligature of dorsal venous complex (DVC) were not significantly associated with EC improvements. RCTs are lacking on pubovesical complex-sparing, seminal vesicle preservation, anterior reconstruction of the puboprostatic collar, musculofascial reconstruction, and DVC suspension to the periosteum of the pubic bone techniques.
Conclusions:
RARP and RS have high-quality evidence supporting their ability to enhance postoperative EC recovery. NS, bladder neck, and PPL preservation may contribute to better EC recovery, although the evidence level is low. Further multicenter RCTs are needed to establish the optimal combination of standard surgical techniques. A new continence outcome-reporting standardization was proposed.
Introduction
Urinary incontinence is a significant cause of postoperative morbidity after radical prostatectomy (RP). Although the problem of the long-term incontinence after robot-assisted RP (RARP) may be considered almost resolved, with 12-month continence rates up to 97%, immediate and early incontinence continue to negatively impact patients' quality of life. 1
Numerous continence-sparing surgical techniques have been developed to enhance patient's postoperative early continence (EC) recovery. 2 These rely on three paradigms: first, preservation of anatomical integrity; second, reconstruction of the anatomical structures to support urinary continence; and third, reinforcement of the structures related to continence.
The etiology of postprostatectomy incontinence has not yet been completely understood. Factors proposed as predictors for urinary incontinence after RP are a short membranous urethral length, older age, long operative time, high body mass index, low preoperative serum albumin level, previous transurethral resection of the prostate, and a wide bladder neck opening during surgery. 3,4 Continence status before surgery, operative technique, surgeon, and postoperative factors could also influence postoperative continence. 5 Nonetheless, surgeon factor is believed to affect functional outcomes, with literature demonstrating that the time to EC varies with technical modifications. 1,5
Despite the immense variety of studies describing various surgical techniques, the validation of a standard set of techniques to expedite patient's postoperative continence remains yet to be established. 6
There is no qualitative systematic review reporting the EC outcomes from randomized controlled trials (RCTs; level evidence 1b) in the currently available literature. 7 Furthermore, heterogeneity of continence definition and outcomes reporting are evident, highlighting the need for a new standardization. 8
The aims of this study are first, to provide the first systematic review of RCTs in the field of continence-sparing RP techniques and to evaluate the available RCTs according to standard criteria for quality assessment; second, to summarize the immediate continence (IC) and EC outcomes and to critically appraise the eligible RCTs to highlight which RP techniques best provide an evidence-based approach to enhance postoperative IC and EC recovery; and finally, to propose a new standardization for IC and EC outcomes reporting.
Materials and Methods
Search strategy
Five different online databases and medical registries were searched: PubMed, Embase, ScienceDirect, Scopus, and Cochrane Central library. An advanced search was run for all data sources, combining MESH terms with Boolean operators. The key words “prostatectomy,” “continence,” and “randomized” were used simultaneously in addition to the name of the surgical technique and its synonyms to further refine the search strategy. Figure 1 summarizes a search example, run on PubMed.
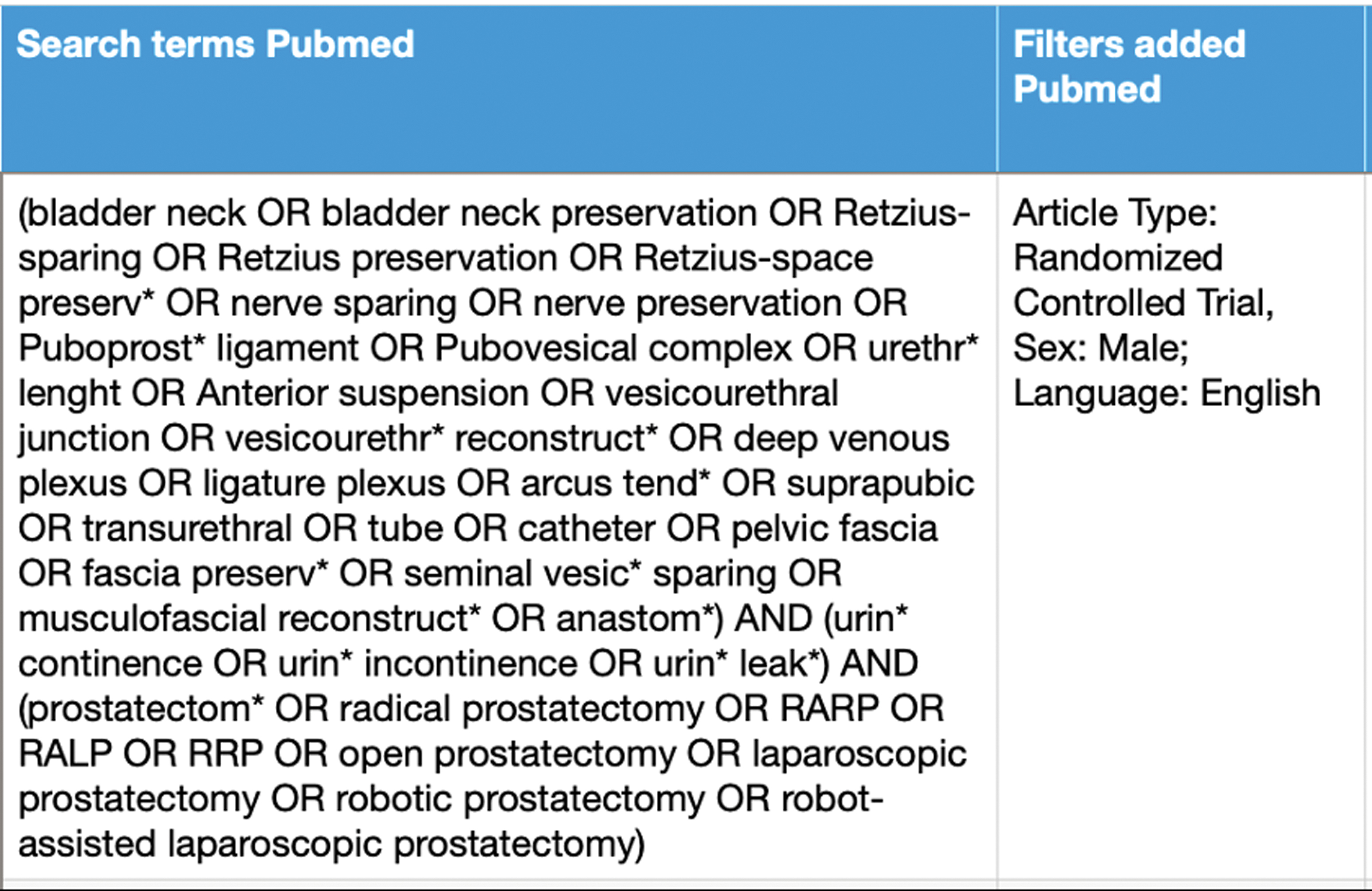
Search terms, Boolean operators and filters used for PubMed. Color images are available online.
Outcomes from identification, screening, and assessment of the searched records are summarized in Figure 2 and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards. 9
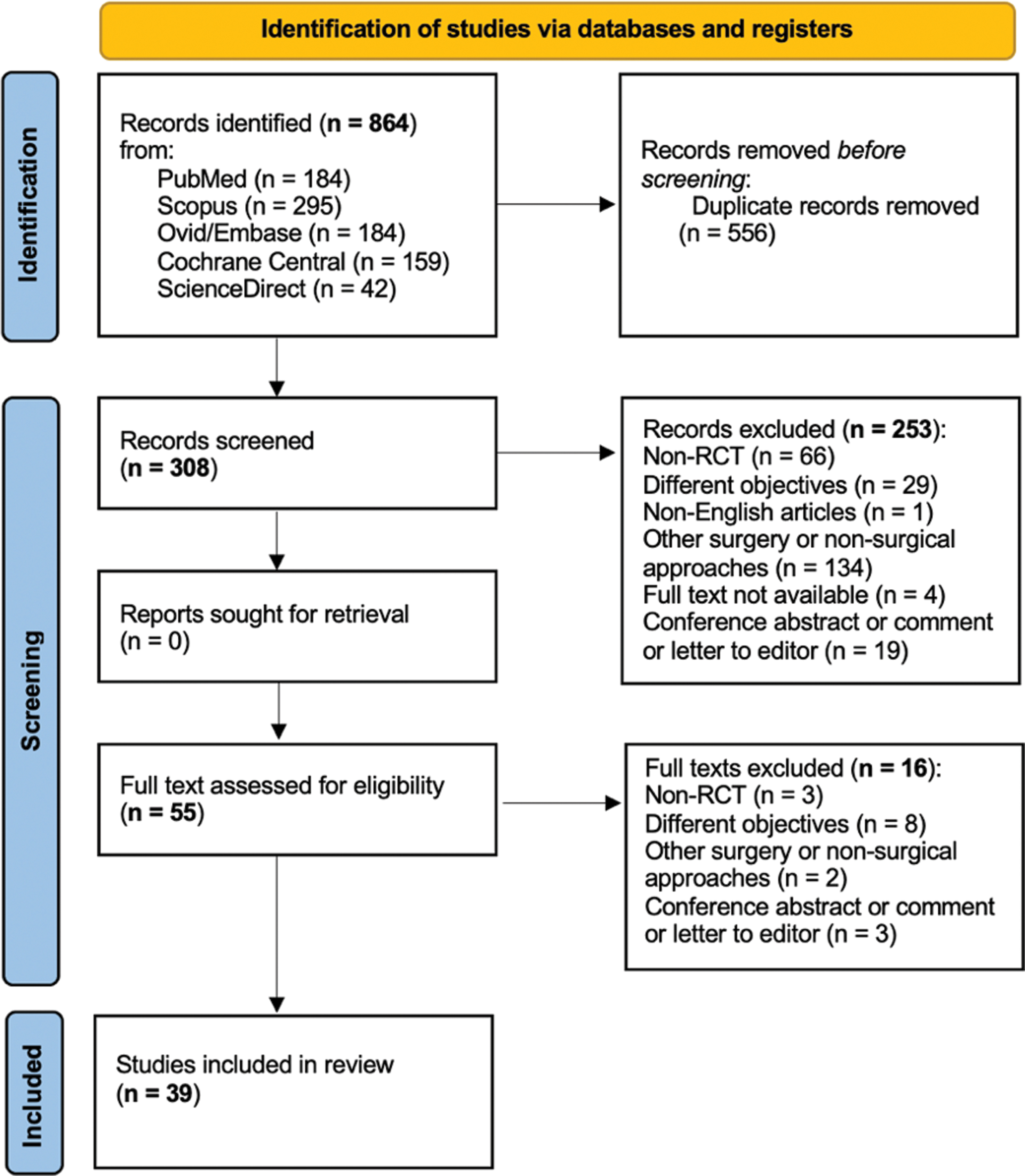
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart for systematic review. Color images are available online.
Study selection and ethics
Inclusion and exclusion criteria were defined according to the PICOS filtering process and are reported in Table 1.
PICOS: Inclusion and Exclusion Criteria
RCT = randomized control trial; UC = urinary continence.
After records identification (n = 864) and duplicates removal (n = 556), two independent reviewers (S.I. and G.C.) screened all search records (n = 308) according to titles and abstracts. The full text of any potentially relevant publication (n = 55) was retrieved for review, and studies were selected based on the criteria previously outlined. Any disagreement regarding study selection was resolved through discussion and consultation with a third reviewer (A.D.A.) to reach a consensus. As this is a systematic review, ethical approval was not required.
Study design
The heterogeneity of continence definitions and continence outcomes reporting prevented an aggregation of quantitative data in a meta-analysis. Hence a qualitative systematic review with a narrative synthesis was conducted to address the research question.
Critical appraisal
A Critical Appraisal Skills Programme (CASP) checklist was completed to critically assess this systematic review and all the eligible studies for inclusion (Supplementary Appendices SA1 and SA2).
Data abstraction and reporting
Data were independently extracted by two reviewers (S.I. and G.C.) and checked for any discrepancies. In all cases of missing or incomplete data, the corresponding authors were contacted, but no additional information was provided.
While scrutinizing the postoperative continence outcomes, a discrepancy between the use of continence definition (use of 0 or 1 pad per day, absence of urinary leakage or ≤30 g urinary leakage) was identified, as well as the heterogeneity in the reporting of postoperative continence outcomes. To simplify data reporting, the outcomes reported by the RCT authors 0–7 days after catheter removal were grouped under IC outcomes and the remaining under EC outcomes. Data on continence definition, measurements, and outcomes were summarized for narrative analysis.
Results
Characteristics of the studies included in systematic review
Records screening identified a total of 39 RCTs exploring postoperative continence outcomes after RP. The included studies were conducted between 2001 and 2021. Duration of each RCT study data collection varied from 3 to 55 months excluding patient follow-up. Sample sizes ranged from a minimum of 42 to a maximum of 718 patients, based on the implied surgical technique and the institution where the prostatectomies were carried out. 10,11
Descriptive characteristics of each study are outlined in Table 2.
Characteristics of included Randomized Control Trials and Quality Assessment
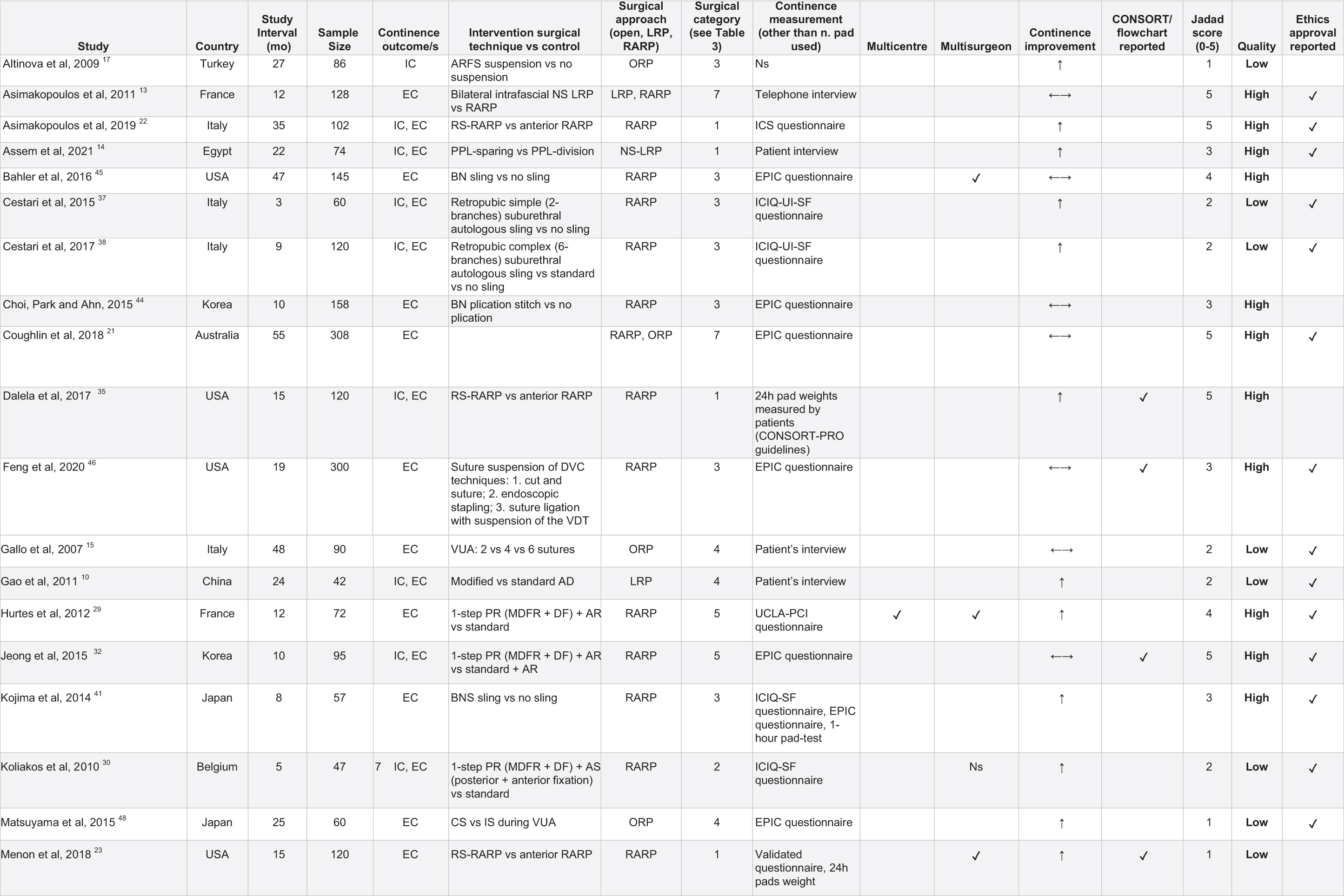
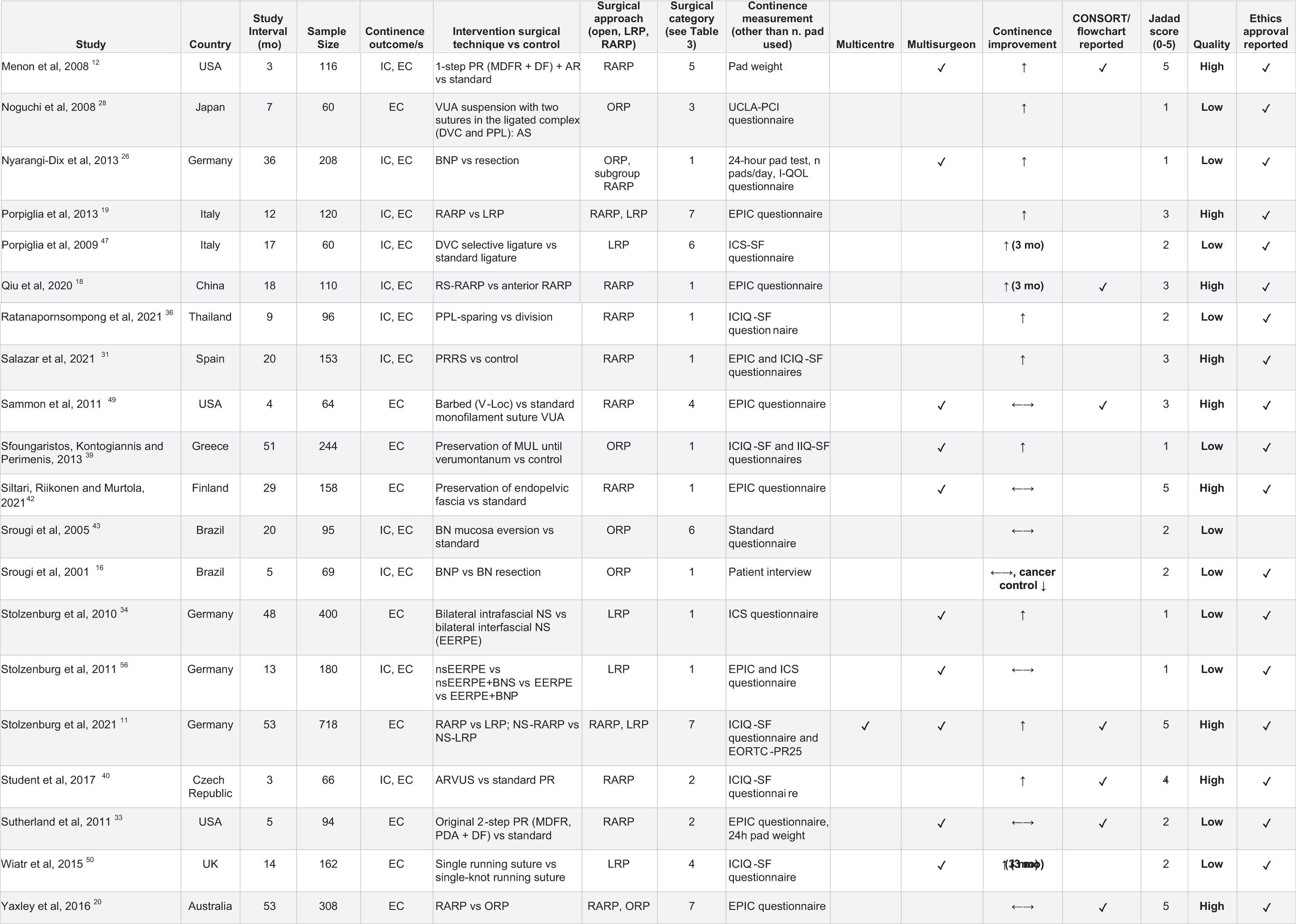
AD = apical dissection; AR = anterior reconstruction; AS = anterior suspension; BNP = bladder neck preservation; BNS = bladder neck suspension; CS = continuous suture; DF = Denonvilliers' fascia; DVC = dorsal venous complex; EC = early continence; EPIC = Expanded Prostate Cancer Index Composite; IC = immediate continence; ICS-SF = International Continence Society-Short Form; ICIQ-SF = International Consultation on Incontinence Questionnaire-Short Form; I-QOL = Incontinence Quality of Life; IS = interrupted suture; MDFR = median dorsal fibrous raphe; ORP = open radical prostatectomy; PPL = puboprostatic ligament; PR = posterior reconstruction; RARP = robot-assisted radical prostatectomy; RS = Retzius sparing; UCLA-PCI = University of California Los Angeles Prostate Cancer Index; VUA = vesicourethral anastomosis.
Heterogeneity in postoperative continence definition
Continence outcomes were not homogeneously reported among the authors. Definition of continence was measured in pads used in a day (absolute number) and/or urinary leakage (grams). There was also variability regarding continence being either strictly defined as the use of no pads per day or as the use of maximum one pad per day. Differences were also noticed among the authors' definition of “use of one pad.” Some defined as one “safety” pad for patient reassurance in case of urinary leakage, whereas others used one pad required because of minor urine leakage.
The outcome measurement also differs among the RCTs. The majority of authors reported patient's “subjective continence” measurements through the completion of internationally validated questionnaires (i.e., Expanded Prostate Cancer Index Composite [EPIC], International Consultation on Incontinence Questionnaire - Urinary Incontinence Short Form [ICIQ-UI-SF], International Continence Society [ICS], International Continence Society-Short Form [ICS-SF], Incontinence Impact questionnaire Short Form [IIQ-SF], University of California Los Angeles Prostate Cancer Index [UCLA-PCI] questionnaires), but others adopted the use of pads per day (Tables 4 and 5).
A minority of authors reported the “objective continence,” measured in pad weights. Criteria implying continence were again variable, ranging between ≤30 g urine leakage per day in one RCT and a stricter 0 g per day as used by the majority. 12 An alternative approach was to use patient feedback regarding their continence status from clinic or telephone follow-up appointments. 10,13 –16 Finally, one author did not report the method used to measure the continence. 17
Heterogeneity was also noticed regarding definition of IC and EC among the authors. IC was mostly reported at catheter removal, which ranged from 5 to 14 days based on the RP approach and technique used. However, one author defined IC as the continence outcomes measured 7 days after catheter removal. 18 Definition of EC also varied with a range of different time intervals within 6 months from surgery.
Data extraction tables
Data obtained from RCT baseline characteristics, surgical factors, RCT design, reporting, and quality assessment, according to the Jadad scale, are detailed in Table 2. Surgical techniques have been grouped into different surgical categories and reported in Table 3 to summarize the studies currently available.
Surgical Category for Each Technique and References
Per-Protocol (PP) analysis.
Intention-to-treat (ITT) analysis.
ARFS = anterior rectus fascial sling; LRP = laparoscopic radical prostatectomy; ns-EERPE = nerve-sparing extraperitoneal endoscopic radical prostatectomy; NS = nerve sparing.
Quality assessment of the included RCTs
Quality assessment was conducted using the Jadad scale criteria (Supplementary Appendix SA3). Of the included RCTs, 19 of 39 studies were low-quality studies (Jadad score 0–2). Common criticisms included the absence of a description of patients lost to follow-up, lack of double-blind randomization, and a lack of an appropriate randomization methodology (e.g.: computer-generated sequences or random number allocation). Only 20 out of 39 studies were considered high-quality randomized trials (Jadad score 3–5). The detailed critical appraisal of the included RCTs provides further insight into the quality assessment of the studies (Supplementary Appendices SA1 and SA2).
Literature gaps
The literature is devoid of a prospective randomized study for the following surgical techniques: pubovesical complex preservation, seminal vesicle preservation, and anterior reconstruction of the puboprostatic collar (i.e.: anterior musculofascial reconstruction or reattachment of the arcus tendineus to the bladder neck).
IC and EC outcomes from included RCTs
Different techniques have been shown to significantly improve IC and EC at different times of follow-up, with reports varying from 0 to 7 days for IC and from 10 days to 6 months for EC outcomes. Among the significant results obtained, a high-quality study design was found in trials assessing the following techniques: Retzius-sparing (RS), nerve-sparing (NS) and puboprostatic ligament (PPL) preservation for both IC and EC; posterior reconstruction (PR) of the rhabdosphincter with or without anterior suspension (AS); and the vesicourethral junction reconstruction for EC.
All outcomes on IC and EC, as well as the surgical interventions and their statistical significance, are detailed in Tables 4 and 5, respectively. To better summarize the evidence gathered from RCTs, the available studies on each surgical technique were grouped and reported in Table 6. Significant outcomes and time of continence measurement after surgery are highlighted as well as their quality assessed in this systematic review.
Comparison of Immediate Continence from Randomized Control Trials
Per-Protocol (PP) analysis.
Intention-to-treat (ITT) analysis.
ARVUS = advanced reconstruction of vesicourethral support; EERPE = extraperitoneal endoscopic radical prostatectomy; ns-EERPE = nerve-sparing extraperitoneal endoscopic radical prostatectomy; PRRS = posterior reconstruction of the rhabdosphincter.
Comparison of Early Continence from Randomized Control Trials
PP analysis.
ITT analysis.
MUL = maximal urethral length; PDA = posterior counterpart of detrusor apron.
Continence Outcomes from Randomized Control Trial Evidence Filtered by Technique and Study Design Quality
Bold font = significant continence outcomes.
Discussion
Last decade, Asimakopoulos and colleagues witnessed the paucity of data in the literature regarding high-quality evidence in the field of continence-sparing RP. 13
With the advent of novel prostatectomy techniques and the publication of multiple studies in the field of postprostatectomy EC achievements, it was deemed necessary to investigate the current literature with a focused approach on RCT-proved surgical methods.
Open radical prostatectomy, laparoscopic radical prostatectomy, and RARP outcomes
In our review, three RCTs compared RARP with laparoscopic radical prostatectomy (LRP), in all of them RARP provides statistically significant EC improvement at 3 months. 11,13,19 Asimakopoulos et al. and Porpiglia and colleagues also demonstrated significant improvement in continence at 1 month and 6 months after surgery. 13,19 Yaxley et al. and Coughlin et al. compared the RARP with open radical prostatectomy (ORP) approaches and reported no significant difference at the 3- and 6-month follow-ups. 20,21 All these studies were high-quality RCTs. Another systematic review, which incorporated non-RCT data, has shown that RARP is associated with a statistically significant advantage in urinary continence recovery, compared with both ORP and LRP. 1
RS-RARP and bladder neck preservation techniques outcomes
Three RCTs reported the benefits of a RS approach on EC, concurring with a recent meta-analysis. 18,22 –24 Another study comparing four different techniques of RARP concluded that RS without bladder neck preservation (BNP) was associated with the poorest continence outcomes at 1 week and 1 month, suggesting that BNP might be responsible for the beneficial effect of the RS approach. 25 Concerning BNP, the evaluated RCTs yielded conflicting results, as reported in Table 6. 16,26 Nyarangi-Dix and associates proved EC enhancement at 6-week, 3-month, and 6-month continence for BNP. 26
On the contrary, Srougi and coworkers also interrupted the randomization process in their RCT, following histology reports of the BNP group that provided a statistically significant difference in surgical margin, compared with the control arm. 16 Both studies were low-quality RCTs. Another systematic review and meta-analysis showed that BNP during RP improved EC and decreased BN stricture rates without compromising oncologic control. 27 Considering the limited and conflicting evidence obtained from RCTs regarding these techniques, outcomes retrieved from recent systematic reviews should be considered.
EC-enhancing surgical techniques based on RCT evidence
Available RCT evidence demonstrated that the AS of dorsal venous complex (DVC) and AS with concomitant PR of the rhabdosphincter enhance EC, with the latter technique being proved by high-quality RCTs. 28 –30 Salazar et al. showed in their high-quality RCT that the PR of the rhabdosphincter alone can improve EC; however, the findings of Jeong et al. (high-quality study) and Sutherland et al. (low-quality study) contradict this. 31 –33 The modified apical dissection proposed by Gao and coworkers has shown significant improvement at 1-month EC, but not at 3-month continence. 10
Two RCTs on NS techniques showed significant EC improvements at 1- and 6-month follow-up intervals, with one study being of high-quality according to the Jadad scale. 34,35 PPL preservation was proved by two RCTs to enhance EC, one of them being of high quality, similarly to the retropubic suburethral slings described by Cestari et al., which instead lacked to demonstrate a high-quality RCT design. 14,36 –38 Equally, urethral length preservation (low-quality study) and vesicourethral junction reconstruction (high-quality study) obtained promising results. Finally, the BN suspension technique described by Kojima et al. (high-quality study) showed improvement at 1-month EC. 39 –41
Surgical techniques that do not enhance EC based on RCT evidence
Different techniques highlighted in Table 6 failed to show statistically significant EC improvement: endopelvic fascia preservation, BN mucosa eversion, BN plication, and BN sling. 42 –45 The selective ligature of the DVC arm described by Feng et al. and Porpiglia et al. was not significantly associated with EC improvements, with some EC enhancement at 3-month follow-up. 46,47 Different laparoscopic and robotic suturing technique-based RCTs did not report any significant results in continence improvements and might be considered worthy options rather than definitive recommendations to be adopted in surgical practice. 15,48 –50
Appraisal of the included RCTs
Half of the included studies were low quality in nature, limiting the internal validity and generalizability of the results and acting as an obstacle to drawing conclusions on the efficacy of the surgical techniques under investigation. However, this should be seen as a flaw of the available evidence and not of the systematic review per se. Furthermore, patients diagnosed with high-risk prostate cancer were excluded from three of the RCTs included in this review, and this might be considered a limitation in these studies, perhaps because low-risk disease encouraged less aggressive approaches with more careful preservation of anatomical structures, thus leading to better continence outcomes. 22,23,35
As summarized in Table 2, Hurtes and colleagues and Stolzenburg and colleagues conducted the only two multicenter and multisurgeon randomized trials on RP techniques, and less than a third of the included RCTs (11/39) were conducted in a single institution by multiple surgeons. 11,29 Therefore, the majority of the published RCTs examining continence-sparing RP techniques are single-surgeon studies. Although some believe that conducting all interventional prostatectomy techniques by the same surgeon is a study strength as it reduces the variation associated with the surgeon experience, other authors report that a study being a single-institution and single-surgeon experience with small number of patients is a drawback for technique dissemination and results reproducibility in other centers. 13,14,32,46,48
Heterogeneity of continence definitions and the new standardization proposal
Most RCTs defined “immediate continence” as the patient's continence status at catheter removal. Consensus or standardization of this definition is lacking. Authors vary in the time between catheter removal and their assessment of IC. Qiu and associates defined IC as the continence outcomes reported by patients at day 7 after catheter removal, Menon and coworkers and Porpiglia and coworkers have reported IC at day 2 after catheter removal. 12,18,19 Similarly, the timeframe for assessment and definition of EC varied between 1 and 6 months after surgery.
Timing of postoperative catheter removal was also variable. A trial without catheter was first done within 7 days after surgery for patients undergoing RARP, and >7 days in the majority of LRP and ORP procedures. Surgical and patient factors may have additionally influenced this timing.
A wide range in rates of postprostatectomy incontinence has been reported in the literature because of the lack of homogeneity in the definition of continence and differences in the methods used to evaluate and report it. 8 The ICS recommended the 1-hour pad-weighting test. 51 Likewise, a 24-hour pad weight leakage has been proved to be useful; however, it may vary significantly on different days of collection, rendering the measurement less precise and reliable. 52
Evaluating continence is challenging, particularly considering the discrepancies in the perception of urinary incontinence between doctor and patient after prostatectomy. 53 Only 14.7% of patients who were considered continent by their doctor also considered themselves to be continent, suggesting conflict between the clinical definitions and measures (based on pad use) and the patient subjective definition of urinary continence.
When comparing patients' continence self-assessment and the measurement of pads used per day, patient self-assessment coincides more with the definition of 0 pads per day rather than that of 0–1 pad per day. 53 Kojima and colleagues already recommended the use of the definition of 0 pads as “it is easily measured objectively, leaves no room for interpretation, and agrees best with the patients' self-assessment.” 54 Moreover, the use of both a validated questionnaire and objective continence measurements is known to achieve better accuracy in postoperative continence determination. 41 In their prospective study on continence and incontinence evaluation after prostatectomy, Holm and colleagues suggested that incontinence may be reported as any leakage and not only as pad use, with grading done on a symptom scale. 55
The heterogeneity of outcome reporting impedes the combination of valuable quantitative data, resulting in the literature gaps investigators have been facing in the past two decades.
We, therefore, propose a new standardization of continence outcomes reporting, as detailed in the Supplementary Appendix SA4. The duration of postoperative catheterization will more heavily influence the “very-early continence” (VEC) than others, and, therefore, may be less valuable in patients with prolonged (>14 days) postoperative catheterization time. Finally, it is important to validate the continence outcomes by adopting one of the following criteria: Use of a validated patient questionnaire and obtain information regarding the number of pads used in a day (social continence), provided nonuse of pads corresponds to return to continence. Use of a validated patient questionnaire and obtain pad weight (objective continence) measuring the urinary leakage in grams, provided no urine leak corresponds to return to continence.
Future perspectives and recommendations
In view of the major findings obtained from this review, the only surgical technique that both proved to enhance postprostatectomy EC and was evidenced by high-quality RCTs was the RARP, when an RS-RARP approach was adopted. Other techniques such as the suspension of the dorsal vascular plexus, the PR technique with or without combination of the AS technique, the BNP, the NS approach, and the PPL preservation seem to enhance EC with different degree of evidence both for the quality of their RCTs and IC and EC outcomes, as summarized in Table 6. Similarly, new techniques described in the literature such as the vesicourethral junction reconstruction, the urethral length preservation, and the retropubic suburethral slings did show promising results and more high-quality research should be advocated to further analyze the consistency of the reported outcomes.
Furthermore, functional results observed in all RCTs should also be interpreted in the light of other surgical and patient factors. Student et al. for instance reported that their outcomes were determined by a combination of techniques. 40 It is common knowledge that a well-conducted surgical procedure, a comprehensive preoperative clinical assessment, and an effective postoperative care are essential to achieving a high rate of urinary continence recovery. 2
To face the long-standing heterogeneity of postprostatectomy IC and EC outcome reporting, urologists should be encouraged to report their results using more stringent continence criteria. Defining the return to continence as the nonuse of pads and absence of urinary leakage is encouraged in our newly proposed standardization for postprostatectomy continence outcome reporting. The use of continence definition encompassing the use of a safety pad should be abandoned, to further reduce heterogeneity of continence measurement.
We have assessed data from RCTs up to 6 months after surgery to find which technique best achieves continence, highlighting the currently available data to help decision-making process and to guide future study designs. However, the choice of the best surgical technique should always be based on patient and surgeon factors, health care resources availability, as well as long-term overall functional and oncologic outcomes. On this merit, other trials not included in this review have investigated the effectiveness of localized prostate cancer treatments, such as the PROTECT Study. 57
Limitations of the review
Despite the study design employing only RCTs for inclusion represents a strength of this review, approximately half of the included studies were low quality when assessed by the Jadad scale. More stringent inclusion criteria, such as only double-blind RCTs or RCTs employing appropriate methods of randomization and high-quality Jadad score, could further refine the PICOS filtering process. Further limitations include the exclusion of systematic reviews and non-English full-text articles RCTs, which provide level 1 evidence.
This study also lacks a meta-analysis; however, as described, the heterogeneity of the reported outcomes and the variety of the included surgical techniques did not prompt for quantitative data combinations, and this should be seen as a flaw of the available literature rather than a limitation of the review design.
In conclusions, early recovery of urinary continence after prostatectomy remains a challenge to be overcome. The current RCT evidence is limited, often low-quality and heterogenous. More high-quality multicenter RCTs, with consistent criteria, are needed to establish a standard surgical technique, or a combination of techniques, to enhance postoperative EC return. Available RCT evidence suggests that RARP is superior to LRP in achieving EC, when an RS-RARP approach is adopted.
Other techniques such as the suspension of the dorsal vascular plexus, the PR with or without combination of the AS technique, the NS approach, the BN, and the PPL preservation have suggested further improvements to continence but require further investigation. We suggest the adoption of the new time-dependent definitions of confidence for future assessment of post-RP continence outcomes.
Footnotes
Authors' Contributions
S.I. contributed to conceptualization, methodology, validation, data curation, writing—original draft, writing—review and editing, and project administration; G.C. was involved in methodology, validation, and data curation; G.E. carried out methodology and supervision; L.O. took charge of writing—original draft and writing—review and editing; P.F. took charge of writing—original draft and writing—review and editing; T.P. and R.G. took charge of writing—review and editing; E.F.-A. and R.M. were involved in writing—review and editing and supervision; and A.D.A. was in charge of conceptualization, methodology, writing—original draft, writing—review and editing, project administration, and supervision.
Author Disclosure Statement
All the authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
Supplementary Appendix SA4
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.