
Abstract
Introduction:
Nutcracker phenomenon is the compression of the left renal vein between the superior mesenteric artery (SMA) and the abdominal aorta. Nutcracker syndrome refers to the presence of nutcracker phenomenon with symptoms. Between 2016 and 2022, we performed 18 robot-assisted laparoscopic extravascular renal vein stent (RALERVS) placements. We sought to assess patient-reported outcomes of RALERVS placement by a single institution.
Methods:
We performed a single-center retrospective review of 18 patients with a minimum of 3 months follow-up. Symptoms were assessed utilizing a questionnaire conducted with a 5-point Likert scale at a minimum of 3 months postoperatively. Five on the Likert scale was severe while 1 was none. Primary study outcomes compared pre- and postoperative patient-reported symptom scores.
Results:
Twelve out of 18 patients responded to the survey. The average length of time from date of operation to completion of survey was 2.6 years. Average age of the cohort was 36 years with a mean BMI of 19.4 kg/m2. There was only one man. Mean operative time was 137 minutes and mean estimated blood loss was 12 mL. Mean preoperative SMA angle was 19° and mean postoperative SMA angle was 36°. Patients reported that flank pain, abdominal pain, nausea, headaches, back pain, pelvic pain, and early satiety improved (p < 0.05). Ten of 12 respondents would recommend RALERVS for nutcracker syndrome.
Conclusion:
RALERVS demonstrates an effective treatment for nutcracker syndrome. Patients reported improved symptoms at 3 months postoperatively across multiple domains. Further studies need to be conducted to assess long-term durability of the extravascular renal vein graft.
Introduction
Nutcracker phenomenon, first reported in 1950, is the entrapment of the left renal vein between the superior mesenteric artery (SMA) and the abdominal aorta. 1 Nutcracker syndrome refers to the presence of nutcracker phenomenon with symptoms including hematuria, intermittent left flank pain, early satiety, nausea, emesis, pelvic congestion syndrome, and dyspareunia. 2 CT, Doppler ultrasonography, and venogram are used to diagnose nutcracker syndrome.
Although no clear consensus exists for diagnosis with imaging, Doppler ultrasonography measuring a diameter five times larger of the left renal vein near the hilum to that of the left renal vein posterior to the SMA may indicate nutcracker syndrome. 3 Peak velocity blood flow ratio of 5:1 at the aorta–mesenteric portion of the renal vein compared with the proximal renal vein is another criteria for nutcracker syndrome. CT findings include an angle between the SMA and aorta of 35° or less, a ratio of the diameter of the left renal vein at the hilum to that posterior to the SMA of 5 or greater, and the beak sign.
The beak sign describes a dilated region and an acutely narrowed segment resembling a bird's beak. 4 Our experience has been to demonstrate retrograde or high-velocity flow in the left renal vein through Doppler ultrasonography or venogram. 5
Nutcracker syndrome is associated with other concomitant diagnoses. These diagnoses include pelvic congestion, Ehlers–Danlos syndrome, and May–Thurner syndrome. May–Thurner syndrome is the partial obstruction of the left common iliac vein by the right common iliac artery. Clinical sequelae of May–Thurner syndrome include left deep vein thrombosis and left leg pain, swelling, and venous stasis.
Treatment of nutcracker syndrome includes weight gain, vascular transposition, renal autotransplantation, nephrectomy, endovascular renal vein stent placement, or extravascular renal vein stent placement. Extravascular stent placement around the left renal vein has been performed laparoscopically. 6 –9 Our institution reported the first robot-assisted laparoscopic extravascular renal vein stent (RALERVS) placement, followed by an updated case series. 5,10
This study reports the first patient-reported outcomes for RALERVS placement. We developed our own questionnaire with common symptoms reported by nutcracker syndrome patients. Primary study outcomes were compared with the pre- and postoperative patient-reported symptom scores.
Methods
After IRB approval was obtained, we performed a retrospective review and phone survey of all patients undergoing RALERVS between 2016 and 2022 by a single surgeon (J.A.C.) at a single academic institution. All surgical procedures were completed using the Da Vinci SI and Da Vinci XI surgical systems (Intuitive Surgical, Inc., Sunnydale, CA). All patients were older than 18 years with symptoms and imaging consistent with nutcracker syndrome. All patients had either renal vein Doppler ultrasonography or venogram to confirm dynamic obstruction. The decision to proceed with RALERVS was made by shared decision making after counseling on all treatment options.
Surgical details
As described in our prior case series, patients were positioned in a modified flank position with the bed flexed at 9° and rotated 17° to achieve a full flank position. 5 Insufflation access was obtained with a Veress needle at the umbilicus. Fifteen millimeters CO2 was used for insufflation pressure throughout the operation. The robotic camera port was placed lateral to the umbilicus and two additional robotic ports were triangulated to the upper left quadrant. A 12-mm assistant port was placed in the left lower quadrant.
After docking the robot, the colon was reflected medially exposing the left renal vein. Dissection was carried out from the branching of the adrenal vein at the left renal vein to the insertion of the inferior vena cava. The distance between the renal vein ostium and adrenal vein was measured using a ruler. A 1-cm diameter ringed polytetrafluoroethylene vascular stent was cut to the measured length and then bivalved. The stent was placed around the left renal vein and secured to itself and the adventitia of the underlying aorta. The adventitia of overlying the SMA was secured to the graft using 3-0 silk to prevent the SMA from rolling off the vein and reobstructing.
Study and analysis
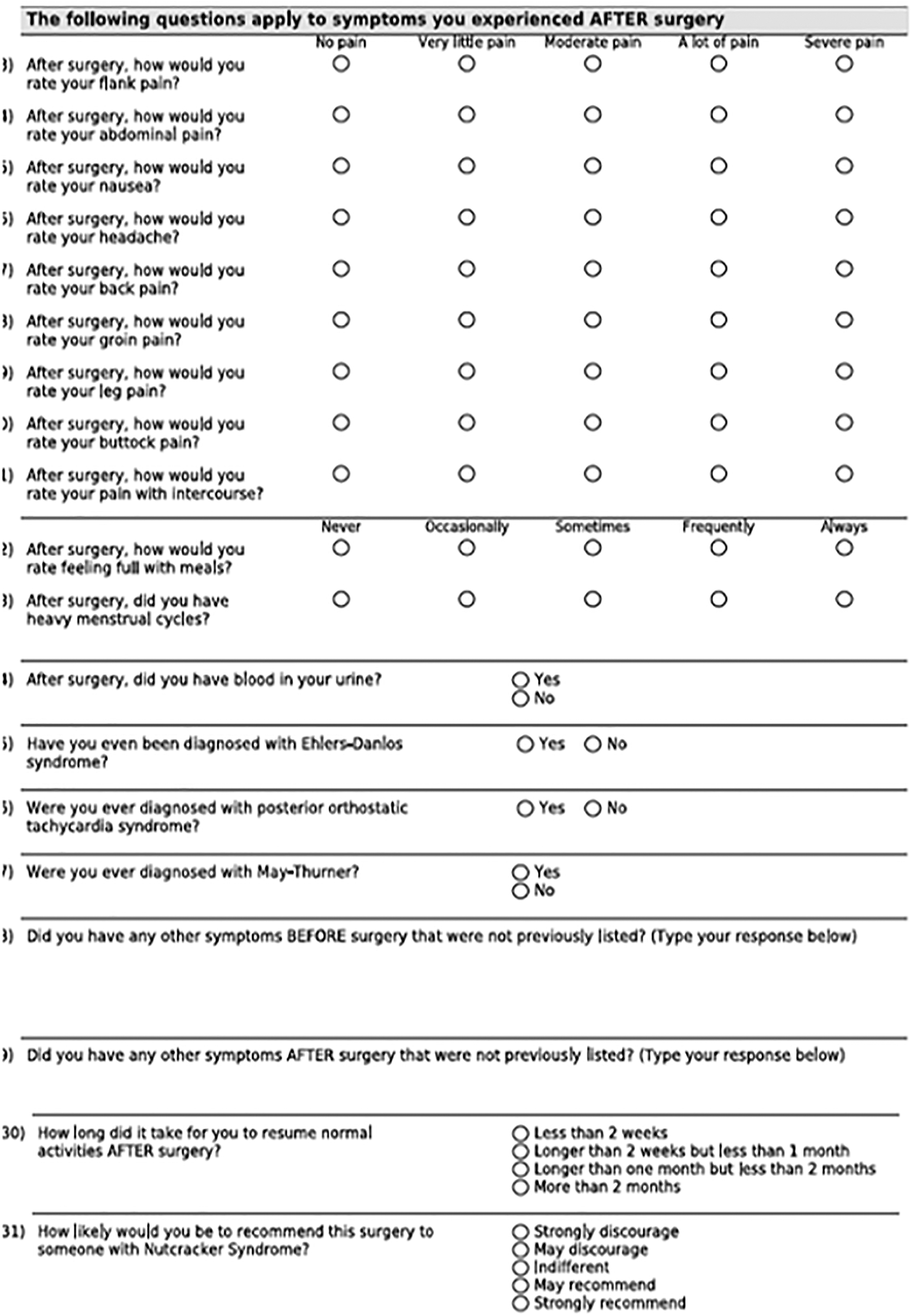
We conducted a phone survey utilizing a questionnaire (Fig. 1). Symptoms were assessed utilizing a questionnaire with a 5-point Likert scale. Five was severe on the Likert scale while 1 was none. The minimum follow-up was 3 months after the date of surgery. We compared outcomes before and after surgery. Time to recovery was recorded. We assessed how likely the patient was to recommend surgery. We conducted summary analysis and Student t-test using Excel and R-studio statistical software.
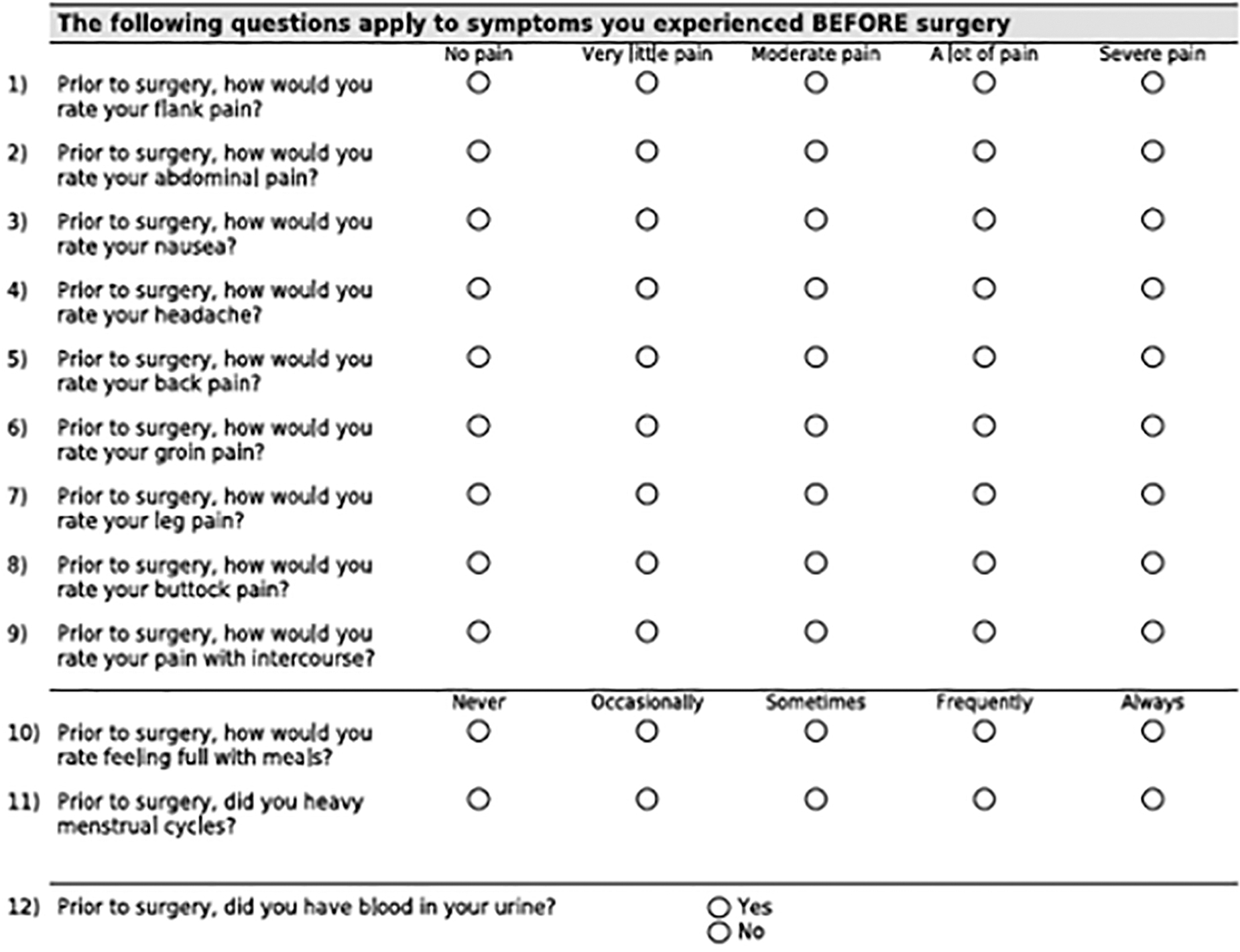
Survey questionnaire.
Results
Twelve out of 18 patients responded to the survey. The average response time from operation date to survey date was 2.6 years. The average age of the cohort was 36 years, and the mean BMI was 19.4 kg/m2. Only one respondent was male. Five patients had May–Thurner syndrome. Other concomitant diagnoses included pelvic congestion and Ehlers–Danlos syndrome (Table 1).
Demographic, Imaging, and Operative Data for Robot-Assisted Extravascular Stent Placement for Nutcracker Syndrome
SMA = superior mesenteric artery.
Mean preoperative superior mesenteric angle was 19° and improved to 36° postoperatively. There were no Clavien–Dindo grade 2 or higher complications. The average length of stay was 1.5 days.
Patients reported statistically significant improvement in flank pain, abdominal pain, back pain, nausea, headaches, pelvic congestion, and early satiety (Fig. 2). Early satiety had the highest preoperative score and the mean symptom score improved by 1.9 points. Flank pain and abdominal pain had the greatest magnitude of improvement after the procedure, 2.3 points. All nine patients who had flank pain noted improvement postoperatively. Ten patients would strongly recommend RALERVS. More than half of respondents stated recovery time was 2 to 4 weeks.

Mean patient-reported outcomes after pre- and post-robot-assisted laparoscopic extravascular renal vein stent placement symptom scores. *p < 0.05.
Discussion
This is the first patient-reported outcomes study for RALERVS. This procedure improved many of the symptoms associated with nutcracker syndrome. It is highly effective for early satiety, flank pain, pelvic congestion, abdominal pain, headaches, and nausea. This can be a life changing surgery for patients who have this rare syndrome and is supported by the high level of recommendation from patients who underwent the procedure. In a recent cross-sectional survey for nutcracker syndrome, 30% of respondents stated that they were unable to work and filed for disability. 11 Over half of the respondents stated that nutcracker syndrome impacted their work significantly.
Although the recent cross-sectional survey characterized the symptoms and burden of nutcracker syndrome patients, the study did not report patient outcomes after procedures. The most common intervention was renal autotransplantation (8 out of the 22 respondents). Only 2 out of the 22 patients underwent extravascular stent placement. Furthermore, the study did not track frequently encountered symptoms beyond flank pain such as headaches and early satiety.
We find that nutcracker patients often endorse headaches and early satiety. The literature for early satiety is sparse. However, there is a case report regarding the association of nutcracker syndrome with Wilkie's syndrome, which is the reduced SMA angle and reduced aorta–SMA distance causing duodenal compression, resulting in postprandial pain and emesis. 12 Nutcracker syndrome patients likely have similar pathophysiology to that of Wilkie syndrome contributing to the early satiety. The proposed pathophysiology for headaches is the increased collateral venous pressure in lumbar veins, leading to edema and thrombosis in smaller vessels around the spine and dural sac. 13,14
Although these patient outcomes are promising for a novel procedure, we believe it is critical to set reasonable expectations preoperatively. First, some of the symptoms may not resolve, particularly those associated with pelvic congestion. Second, although most patients recovered in 4 weeks, three patients reported recovery of >8 weeks. The frequently most cited reason was mid-back pain. We hypothesize that the back pain may be attributed by the retroperitoneal location of the surgery along with the low BMI of the cohort. Third, as mentioned in our prior case series, chylous ascites may develop given the lymphatic channels encountered during surgery. 5 Therefore, we judiciously use bipolar electrocautery and place all our patients on a medium chain triglyceride diet postoperatively.
There are a few limitations to this patient-reported outcomes study. First, 12 out of 18 patients responded to the phone survey. This is higher than most phone surveys, however, one would expect that the novelty of this condition may have generated more responses. The six nonrespondents could not be reached through telephone. Second, the durability of this procedure is still unknown. The earliest respondent was from 2016 and the average length of time from operation date till survey completion was 2.6 years.
Third, the study had recall bias. It was retrospective and required patients to recall symptoms pre- and postoperatively. Nevertheless, this is the first such attempt at understanding patient-assessed outcomes and sharing this information with the surgical community and patients with this rare syndrome is warranted.
Conclusion
This study can aid surgeons in counseling patients for robot-assisted extravascular stent placement. Surgeons can set expectations for patients on which symptoms may improve postoperatively. Further follow-up is needed to demonstrate continued durability.
Footnotes
Authors' Contributions
J.F. contributed to conceptualization, formal analysis, investigation, and writing—original draft; H.D.K. was involved in investigation and writing—review and editing; M.A.A. carried out writing—review and editing; J.A.C. carried out conceptualization and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project did not require any funding,